INTRODUCTION
The complication of protruding preperitoneal fat (PPF) is very rare even though PPF is frequently encountered during hernia surgery. It is called a cord lipoma in the surgical literature
1-
3. Herein, we report a case of a hemorrhagic complication of PPF causing swelling and discomfort in the groin. By preoperative ultrasonography, this was misidentified as an incarcerated inguinal hernia containing omental fat.
CASE REPORT
A 5-year-old boy, who had no history of hernia, was admitted with 4 days duration of swelling and discomfort on right groin during exercise. He had undergone a successful appendectomy 12 days prior and was discharged on 4th postoperative day. His groin symptoms developed on the 8
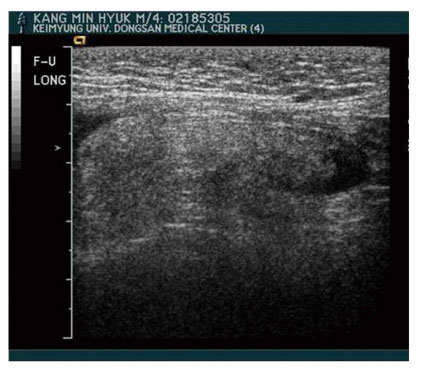
th day of post appendectomy and worsened steadily. On physical examination, asymmetrical swelling without redness on the right groin in the pubic region and mild scrotal swelling were observed with palpable thickened spermatic cord. Neither tenderness or rebound tenderness were noted. Ultrasonography showed an apparent right inguinal hernia containing omental fat (
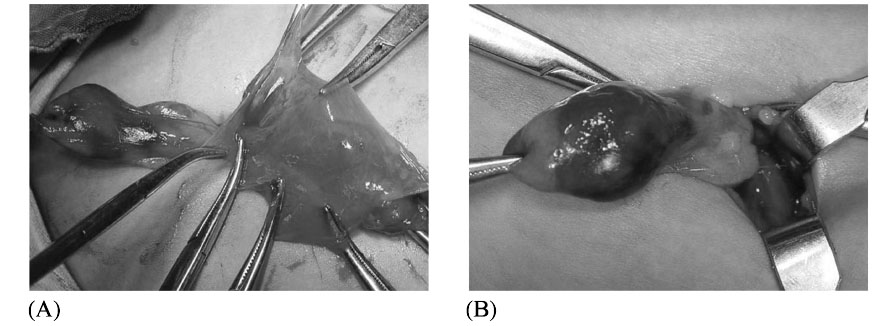
Fig. 1). On operation, we found a bulbous hemorrhagic fat mass attached to the anterolateral portion of the spermatic cord structures and a transparent thin hernia sac located in anteromedial portion of the cord without containing structures (
Fig. 2A). The hemorrhagic fat lobule extended to the level of the constricted internal ring and was obviously normal in color above the internal ring (
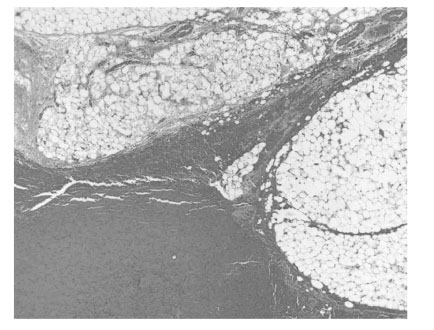
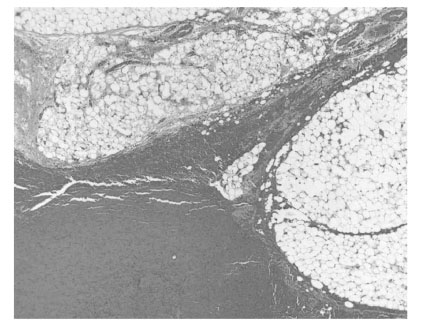
Fig. 2B). After separation of the fat mass from the cord structure, the hernia sac was ligated at the level of the internal ring and excised. A hemorrhagic PPF measuring about 3.0 × 2.0 × 1.5 cm. was also excised at the level of the internal ring. The wound was closed in layers and protected by collodion. Pathology showed hemorrhage of lipoma (
Fig. 3).
DISCUSSION
The most common complication of inguinal hernia is incarceration. If it is not reduced, an emergency operation is needed. Containing structures can include small bowel, appendix, omentum, colon, or rarely Meckel's diverticulum. In girls, the ovary, fallopian tube, or both are usually incarcerated.
Lipomatous lesion of the cord is a continuation of preperitoneal fat through the deep inguinal ring
2 and has been reported as a lipoma of the cord. It is a common feature in an adult male population
1-
3. Lilly and Arregui
3 said that all lipomas of the cord have connection to the retroperitoneal fat whether seen as a protrusion of extra-peritoneal fat or separate.
The prevalence of cord lipomas was 75% in adult male post-mortem subject, who have no hernia observed
2. Most cord lipomas are incidentally encountered during the operative repair of the inguinal hernia with variable prevalence from 22.5%
3 to 72.5%
1 in adults. However, there are only a limited number of reports in pediatric ages. Kovalivker et al
4. noted that the presence of protruding extra- peritoneal fat is always bilateral and is an important predictor of contralateral hernia and an excellent indicator for performing a contralateral groin exploration, especially in children over one year of age. Carilli et al
1. also believed that herniation of extra-peritoneal fat through the inguinal canal should be counted as an inguinal hernia requiring treatment.
Preoperative diagnosis of PPF is very difficult. A few have inguinal pain and swelling. Even ultrasonography is helpful in patients with equivocal physical findings and in those with acute inguinoscrotal swelling
1,
5, the hernia sac may be hard to discern on sonography if there is no protruding intra-abdominal structures or fluid within the sac. Moreover, groin sonography cannot always differentiate PPF from indirect inguinal hernia containing omentum
3. Both are potential mimics on sonography by showing an elongated hyperechoic mass that can be traced back to the internal ring but a lipoma is generally smaller and more homogeneous
5.
Computed tomography (CT) may differentiate inguinal canal lipoma from the fat-containing inguinal hernia by showing a well demarcated superior wall which can be traced back to their extra-peritoneal fat origin lateral to the inferior epigastric vessels in inguinal canal lipoma but no recognizable superior walls in hernia fats
6. Recently Garvey
7 reported that lipoma of the spermatic cord was responsible for false-positive CT results when they used CT for the diagnosis of clinically occult groin hernia.
Although it is difficult to say that what causes hemorrhage in PPF in our case, we assume that it may result from a sudden increase of intra-abdominal pressure by pain or coughing after appendectomy. The resultant contraction of the abdominal muscle may cause compression of the insinuated PPF at the tight internal ring. Constriction of the internal ring leads to venous and lymphatic obstruction and subsequent swelling of the fat as in the incarcerated hernia. This compression provoked venous congestion and subsequent bleeding to PPF base.
When the PPF is very small in size, it is ignored during high ligation of the hernia repair. If fat is large enough to cause clinical misdiagnosis, it is strongly recommended to remove it at the level of the internal ring when hernia sac is excised for making a differential diagnosis from the recurrent inguinal hernia
1.
We believe that symptomatic PPF caused by hemorrhage is an extremely rare complication in a patient with clinically occult inguinal hernia. A PPF should be considered as the one of the possible diagnosis if fat tissue is noted in inguinal canal in preoperative study.
REFERENCES
- 1. Carilli S, Alper A, Emre A. Inguinal cord lipomas. Hernia 2004;8:252-254.
- 2. Heller CA, Marucci DD, Dunn T, Barr EM, Houang M, Dos Remedios C. Inguinal canal "lipoma". Clin Anat 2002;15:280-285.
- 3. Lilly MC, Arregui ME. Lipomas of the cord and round ligament. Ann Surg 2002;235:586-590.
- 4. Kovalivker M, Lazar L, Erez I, Motovic A. The value of protruding extraperitoneal fat in predicting contralateral inguinal hernia. Pediatr Surg Int 1993;8:38-40.
- 5. Yang DM, Kim HC, Lim JW, Jin W, Ryu CW, Kim GY, et al. Sonographic findings of groin masses. J Ultrasound Med 2007;26:605-614.
- 6. Fataar S. CT of inguinal canal lipomas and fat-containing inguinal hernias. J Med Imaging Radiat Oncol 2011;55:485-492.
- 7. Garvey JF. Computed tomography scan diagnosis of occult groin hernia. Hernia 2012;16:307-314.
Fig. 1Ultrasonography showed omental fat containing hernia sac.
Fig. 2Intraoperative findings showing a bulbous hemorrhagic fat mass on the anterolateral portion of the spermatic cord structure and a transparent thin hernia sac in anteromedial position of the cord without containing structure (A). The fat lobule showed obviously normal in color at the level of internal ring (B).
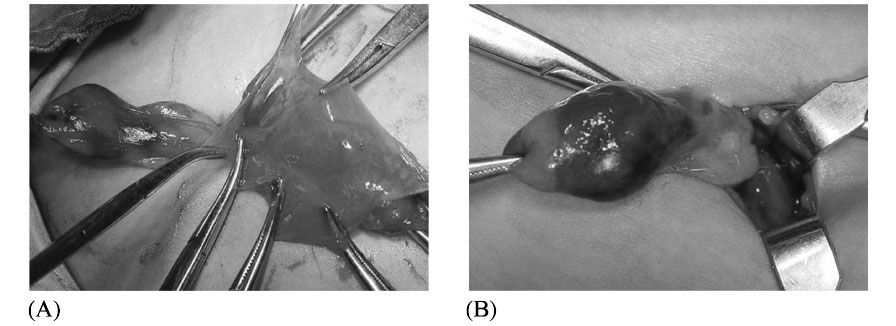
Fig. 3Microscopic findings showing hemorrhage of lipoma (H & E).
Citations
Citations to this article as recorded by