1Division of Pediatric Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
2Department of Plastic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
Copyright © 2015 by the Korean Association of Pediatric Surgeons
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.



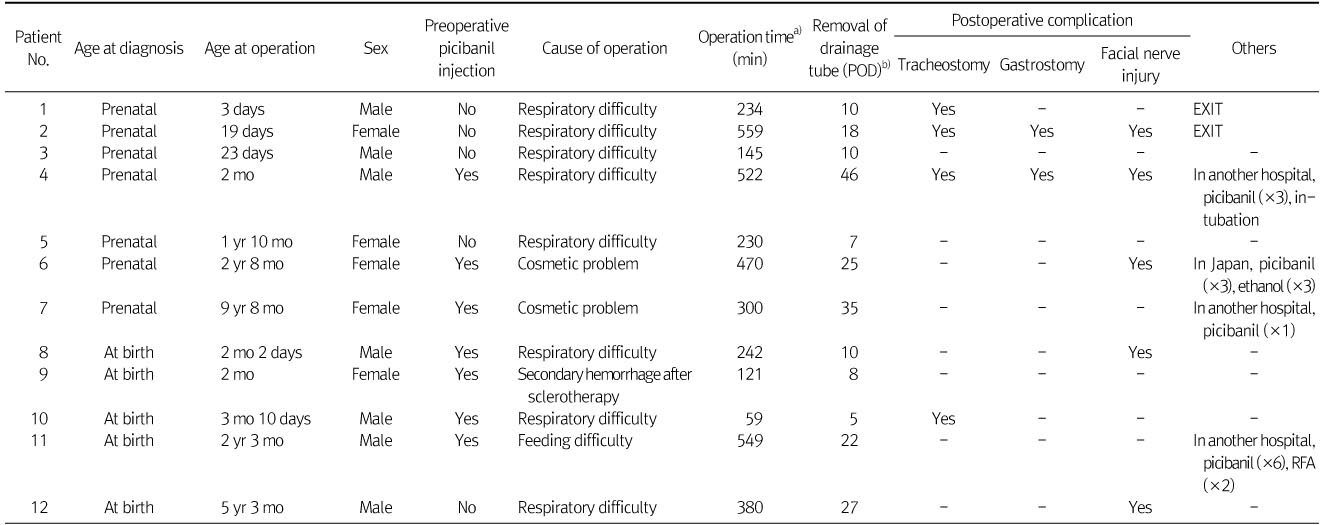
Preoperative Characteristics of 12 Patients with Cervical Lymphangioma and perioperative Details
POD, postoperative day; EXIT, ex utero intrapartum treatment; RFA, radiofrequency ablation.
a)Median 300 min, range 59-559 min. b)Mean 19 days, range 7-46 days.
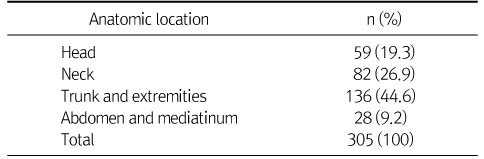
Distribution of Our Patients according to the Anatomic Location of Lymphangiomas
POD, postoperative day; EXIT, ex utero intrapartum treatment; RFA, radiofrequency ablation.
a)Median 300 min, range 59-559 min. b)Mean 19 days, range 7-46 days.