

Purpose
The aim of this study was to compare the clinical features and examine the safety and feasibility of laparoscopic surgery versus open surgery in children with solid pseudopapillary tumors (SPTs).
Methods
Patients under age 18 diagnosed with SPT who underwent surgery for the condition at our single institution from January 2005 to December 2019 were retrospectively analyzed. The demographics and postoperative outcomes in the two groups were compared according to the surgical method and tumor locations.
Results
The 25 patients consisted of 23 females and two males with a mean age at surgery of 13.2 years (range, 6 to 18 years). The lesions were located in the pancreatic head (n=7, 28.0%), and body or tail (n=18, 72.0%). Fifteen patients (60.0%) were treated with laparoscopic surgery. In all patients, there was no difference in intraoperative and postoperative outcomes between the two groups. When analyzed according to tumor location, complications including postoperative pancreatic fistula did not show significant differences with the surgical method in both the head group and body or tail group.
Conclusion
Compared to open surgery, the clinical outcomes and complication rate of the laparoscopic approach in pediatric SPT patients was not significantly different. Therefore, laparoscopic surgery for SPTs in pediatric patients may be a feasible option.
The aim of this study was to compare the clinical features and examine the safety and feasibility of laparoscopic surgery versus open surgery in children with solid pseudopapillary tumors (SPTs).
Patients under age 18 diagnosed with SPT who underwent surgery for the condition at our single institution from January 2005 to December 2019 were retrospectively analyzed. The demographics and postoperative outcomes in the two groups were compared according to the surgical method and tumor locations.
The 25 patients consisted of 23 females and two males with a mean age at surgery of 13.2 years (range, 6 to 18 years). The lesions were located in the pancreatic head (n=7, 28.0%), and body or tail (n=18, 72.0%). Fifteen patients (60.0%) were treated with laparoscopic surgery. In all patients, there was no difference in intraoperative and postoperative outcomes between the two groups. When analyzed according to tumor location, complications including postoperative pancreatic fistula did not show significant differences with the surgical method in both the head group and body or tail group.
Compared to open surgery, the clinical outcomes and complication rate of the laparoscopic approach in pediatric SPT patients was not significantly different. Therefore, laparoscopic surgery for SPTs in pediatric patients may be a feasible option.
Solid pseudopapillary tumors (SPTs) comprise 2%–3% of primary pancreatic tumors in all age groups and are most common in young female patients [1, 2]. SPT has been recognized as benign with a low-grade malignant nature with the potential to metastasis [3, 4]. Surgery is the most definitive treatment because of its effectiveness, and complete resection has a good prognosis in 95% of the patients [2, 5, 6].
Recently, minimally invasive surgery was associated with cosmetic excellence, early recovery after surgery with shorter hospital stay, and reduced rates of complication rates such as intraoperative blood loss [7]. Also, in pediatric patients, minimally invasive surgery is widely and increasingly performed because of increasing expertise and feasibility [8, 9, 10, 11]. More than 500 laparoscopic surgical resections have been performed in adult patients with SPT. In contrast, the laparoscopic approach for SPT in children has not been frequently reported in the literature [7, 12].
The aim of this study was to compare the clinical features and examine the safety and feasibility of laparoscopic surgery versus open surgery in children with SPTs.
Between January 2005 and December 2019, 30 patients under age 18 with SPT who had undergone surgical resection at our hospital were retrospectively reviewed. 5 patients who underwent pancreaticoduodenectomy or total pancreatectomy were excluded from the analysis comparing open versus laparoscopy (Fig. 1). Demographics and clinical data were collected. The patient demographics including age, sex, body weight at surgery, operation date, the operative procedure, other organ resection, operation time, blood loss, and resection margin status were collected and analyzed the medical records. The size of the tumor was measured as the largest point of the tumor on preoperative computer tomography (CT). Postoperative data such as time to oral intake, length of the postoperative hospital stay, postoperative complications, mortality, and recurrence rate were collected from the medical records. Postoperative complications were checked as cases with a score of 3 or higher according to the Clavien-Dindo (CD) classification or having a postoperative pancreatic fistula (POPF). The POPF data were classified into biochemical leak (grade A), and grades B and C according to the International Study Group of Pancreatic Fistula (ISGPF) definitions [13, 14].
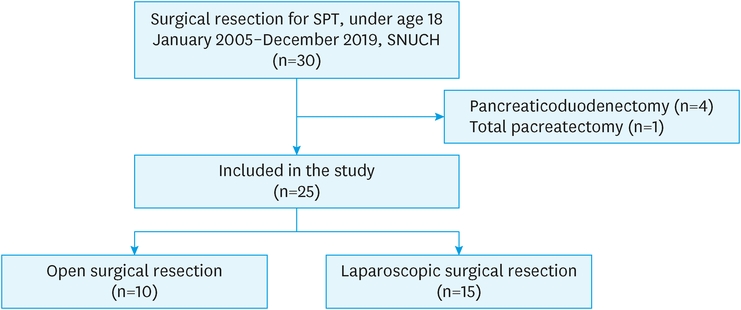
Fig. 1
Flow chart of patient selection.
SPT, solid pseudopapillary tumor; SNUCH, Seoul National University Children’s Hospital.
The patients were divided into two groups according to the operation method (open group vs. laparoscopy group) and according to tumor location (head group vs. body or tail group). Each group divided by tumor location was also analyzed according to the surgical method. The average follow-up period was 51 months, 68 months (range, 7–115 months) for the open group, and 34 months (range, 15–142 months) for the laparoscopic group. A stapler was used for all cases in laparoscopic distal pancreatectomy (LDP), whereas in the case of open distal pancreatectomy (ODP), a stapler was used in some cases and sutures were used in others for stump closure. This study was approved by the Institutional Review Board of Seoul National University Hospital (number 1811-053-983).
The distribution of continuous variables is reported as the mean with standard deviation (SD) or median with interquartile range (IQR). The categorical variables are presented as numbers and percentages. The comparison between the two groups was carried out using a non-parametric test such as χ2 test, Fisher’s exact test or Mann-Whitney U test. Statistical analysis was performed using SPSS 25.0 for Windows software (SPSS Inc, Chicago, IL, USA). A p-value of less than 0.05 indicated local statistical significance.
The mean patient age was 13.2 years and 23 (92.0%) were female. Fifteen patients underwent laparoscopic surgery (60.0%). Eighteen patients had a lesion on the body or tail (72.0%). Seventeen patients underwent distal pancreatectomy (68.0%) and eight patients (32.0%) underwent enucleation (Table 1).
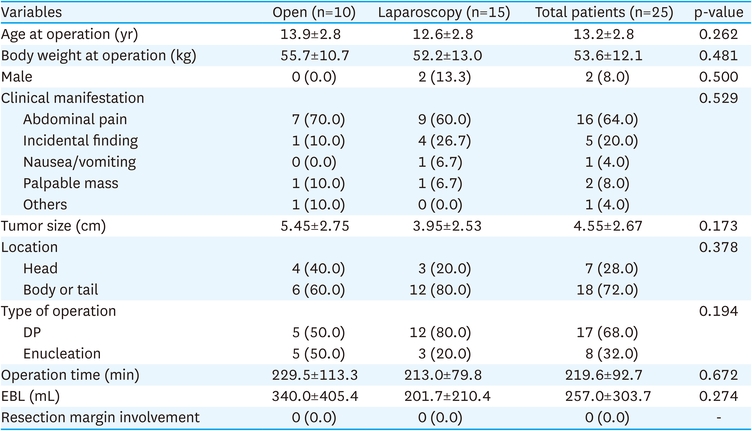
Table 1
Demographic and surgical data
There was no difference in demographics such as age, gender, weight, tumor size, tumor location and the type of operation between the open group and the laparoscopic group. Of the 15 patients in the laparoscopic group, 12 patients had body or tail tumors and underwent distal pancreatectomy. The remaining three patients with tumors located in the head underwent enucleation.
In the postoperative outcomes, there was no difference between the laparoscopic group and the open group, including POPF, radiologic intervention, reoperation, time to oral intake, and postoperative hospital stay length. There was no tumor recurrence during the total follow-up period or mortality in either group (Table 2).
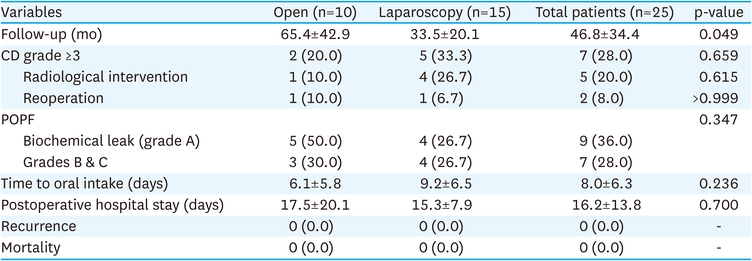
Table 2
Postoperative outcomes
For patients with tumors on the head, there was no difference in demographics and tumor size between the open group and the laparoscopic group. Enucleation was performed in all cases in the laparoscopic and the open group. All three patients who underwent laparoscopic enucleation developed a grade B POPF, and two of them underwent radiological intervention. However, there was no statistical difference between the open group and the laparoscopic groups in time to oral intake and length of stay after surgery in patients with head tumors (Table 3).
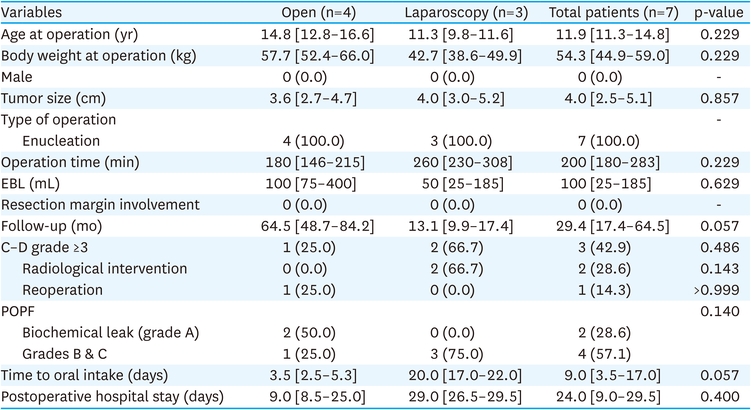
Table 3
Patient characteristics and postoperative outcomes in head SPTs
In the case of body or tail tumors, there was also no significant difference in demographics between the two groups except tumor size. Tumor size tended to be significantly larger in the open group. Type of operation was no statistical difference between the open group and the laparoscopic group. One patient in the open group underwent enucleation, and the remaining open group patients and all patients in the laparoscopic group underwent distal pancreatectomy. There was no difference in complications according to radiological intervention or reoperation, incidence of POPF, time to oral intake, and postoperative hospital stay duration between the two groups of patients with tumors on the body or tail (Table 4).
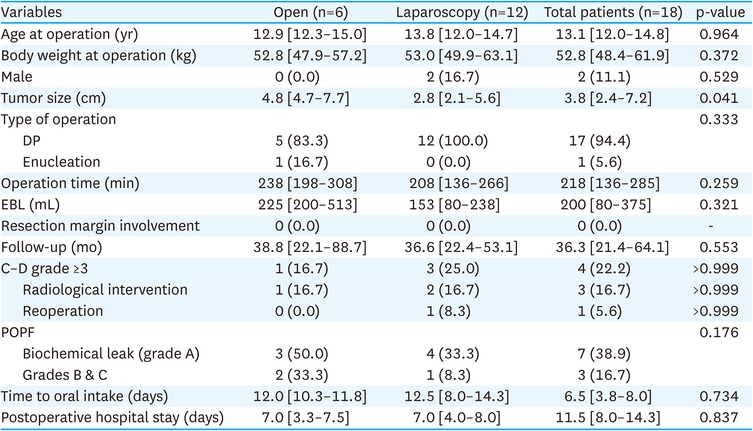
Table 4
Patients characteristics and postoperative outcomes in body or tail SPTs
SPT is the most common pediatric pancreatic tumor, but has a favorable prognosis with surgical excision [15]. Although laparoscopic technique is a major procedure with minimally invasive surgery in recent surgical trends, there are fewer studies on laparoscopic surgery for SPT in children. Our study showed that complications requiring radiological intervention or reoperation and the occurrence of a POPF were not statistically different between the laparoscopic group and the open group in the entire patient cohort.
In 2011, Cavallini et al. [16] performed a retrospective review of 10 patients who underwent laparoscopic surgery for SPT. Of the 10 patients, three patients in this case series were children. Six patients did not experience any event during postoperative period, and all patients were alive and disease-free. Although they reported that laparoscopic surgery was safe for SPT, the study suggested that its application in pediatric cases is still being developed. Petrosyan et al. [17] reported three cases of laparoscopic pancreatic surgery for pediatric SPT. All three cases were tumors in the pancreatic tail and there were no intraoperative or postoperative complications. This study enhanced the knowledge of minimally invasive SPT treatment in pediatric patients.
For more detailed results, according to tumor location, we divided the patients into the head group and the body or tail group and performed a reanalysis. Among the initially enrolled patients, in head tumors, various surgical methods were included in the case of laparotomy compared to laparoscopic group who had only enucleation. However, conventional pancreatectomy such as pancreaticoduodenectomy or total pancreatectomy include anastomosis, and have higher risks of surgical complications with technical difficulties rather than enucleation. As a result, we performed the analysis excluding these operation cases. Zhou et al. [18] performed a study comparing open and laparoscopic method for pancreatic head tumors. In that study, the operation time was longer in the laparoscopic group (open group vs. laparoscopic group; 260.5 vs. 330.0 minutes, p<0.001), but the estimated blood loss was less than that of the open group (open group vs. laparoscopic group: 200.0 vs. 150.0 mL, p<0.001). Similarly, in the present study, for estimated blood loss (EBL), there was no statistically significant difference, but the mean value was lower in the laparoscopic group (open group vs. laparoscopy group: 340.0 vs. 201.7 mL). This may not have been statistically significant due to the small number of patients in groups.
Cho et al. [19] reported that indications for the enucleation of SPTs in pediatric patients. Although they did not compare the laparoscopic approach and open surgery, they showed that enucleation could be attempted instead of conventional pancreatectomy for head tumors. They reported that the patients in the enucleation group had a higher rate of grade B POPFs than the patients in the conventional pancreatectomy group, but the time to oral intake and hospital stay were shorter. In our study, grade B POPFs occurred in all patients who underwent laparoscopic enucleation, but they were resolved by maintaining Jackson-Pratt (JP) drainage or percutaneous drainage without reoperation. A preoperative pancreatic stent was applied to 2 patients who underwent laparoscopic enucleation.
A few studies have been conducted on the advantages of LDP compared to ODP. The first was a 30-patient series comparing 15 case-controlled LDPs and 15 historical ODPs by Velanovich [20]. POPF rates were similar between the LDP and ODP groups, but the median length of hospital stay was shorter for LDP patients. A previous study reported that patients underwent LDP started oral intake in less than half the time required for patients with ODP [21]. Kooby et al. [22] performed a multicenter retrospective review between 2002–2006 comparing the perioperative outcomes of LDP with the traditional open approach. They reported 26% and 32% of pancreatic fistula rates among patients who underwent LDP and ODP, respectively. Namgoong et al. [6] performed a retrospective study of 22 pediatric patients who underwent distal pancreatectomy for SPT. Although there was no difference in postoperative complications, the LDP group started oral intake earlier and had earlier discharges from the hospital. They concluded that LDP was a safe option for pediatric SPT compared to ODP.
Similar to those studies, in the present study, although not statistically significant, the incidence of grade B or C POPF in body or tail tumors was 8.3% in the laparoscopic group, which was tended to lower than that in the open group. However, studies showing fewer POPFs in LDP are still controversial, and most of the studies had limitations in that they were based on adults.
Our study had several limitations. First, the study included a retrospective design and a relatively low number of cases. The comparison of open surgery and laparoscopic surgery by a large, randomized, controlled clinical trial is ideal, but was not performed in this study. Second, in the head group, all cases of laparoscopic approach were enucleation, so there was no comparison about conventional pancreatectomy such as Whipple’s operation or pylorus-preserving pancreaticoduodenectomy. Recently, as conventional pancreatectomy through minimal invasive surgery such as laparoscopy or robotic surgery is increasing, long term additional research is needed [23, 24]. Third, the first case of laparoscopic surgery for SPT in our institution was performed in 2012, and since then, the number of minimally invasive surgeries including laparoscopic and robotic surgery has gradually increased (Fig. 2). It was difficult to compare them at the same time because the treatment plan was different according to the time period.
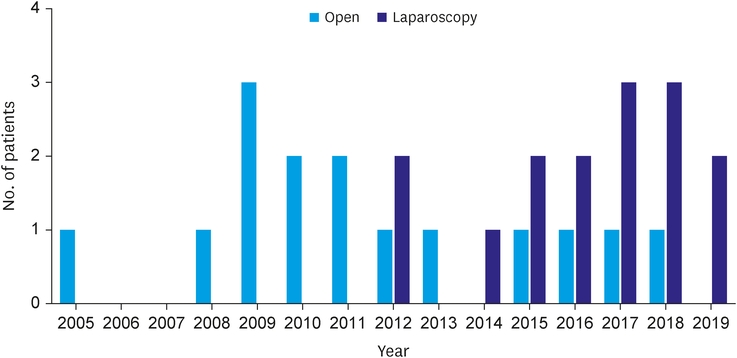
Fig. 2
Distribution of surgical method by year.
In conclusion, both head tumor and body or tail tumor, the complication rate and the clinical outcomes of the laparoscopic approach in pediatric SPTs was not significantly different than that of open surgery. Therefore, laparoscopic surgery for SPTs in pediatric patients may be a feasible option.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H.Y.
Data curation: H.H.
Formal analysis: Y.J.K., K.D.
Methodology: H.H., Y.J.K., K.D.
Writing - original draft: H.H.
Writing - review & editing: Y.H.B., K.H.Y.
