

Among the 5 different Todani subtypes of choledochal cyst, type II choledochal cyst is known to be the rarest. A 13-month-old female who had underlying congenital portal vein stenosis and portal hypertension presented sudden hematemesis and abnormality in liver function test. Upon evaluation with a liver ultrasonography, a 1.7 cm-sized cystic lesion near the common bile duct and duodenum was incidentally discovered, and further imaging with magnetic resonance cholangiopancreatography, upper gastrointestinal series, computed tomography, and percutaneous transhepatic cholangiography revealed type II choledochal cyst. The patient underwent choledochal cyst excision with Roux-en-Y hepaticojejunostomy and had no acute postoperative complications.
Among the 5 different Todani subtypes of choledochal cyst, type II choledochal cyst is known to be the rarest. A 13-month-old female who had underlying congenital portal vein stenosis and portal hypertension presented sudden hematemesis and abnormality in liver function test. Upon evaluation with a liver ultrasonography, a 1.7 cm-sized cystic lesion near the common bile duct and duodenum was incidentally discovered, and further imaging with magnetic resonance cholangiopancreatography, upper gastrointestinal series, computed tomography, and percutaneous transhepatic cholangiography revealed type II choledochal cyst. The patient underwent choledochal cyst excision with Roux-en-Y hepaticojejunostomy and had no acute postoperative complications.
Choledochal cyst is a rare congenital disorder with an estimated prevalence of 1 in 13,000 to 1–2 million live births [1]. It is more commonly found in Asia and the female:male ratio is known to be 3:1 to 4:1 [2]. In 1959, Alonso-Lej et al. [3] first proposed a classification system of choledochal cysts, and in 1977, Todani et al. [4] suggested a modified system which has gained wide acceptance up to this day. According to the Todani classification, type I, cystic dilatation of the common bile duct (CBD), and type IVa, the combination of extrahepatic and intrahepatic cysts, are most frequently encountered, whereas type II, single bile duct diverticulum, is rarest, constituting approximately 0.8%–5% of all choledochal cyst cases [5]. In this case report, we describe a 13-month-old female who was diagnosed with Todani type II choledochal cyst.
A 13-month-old female from the United Arab Emirates was referred to the Pediatric Surgery Department of Seoul National University Children's Hospital (SNUCH) for surgical management of Todani type II choledochal cyst. The patient had underlying idiopathic portal vein stenosis, portal hypertension, chronic lung disease, neonatal sepsis, and alpha thalassemia. At 11 months, the patient was admitted to Dubai Hospital due to sudden hematemesis, and her initial lab results revealed hemoglobin 8.2 g/dL, white blood cell 16,300/µL, platelet 164,000/µL, total bilirubin 0.5 mg/dL, albumin 3.0 g/dL, gamma glutamyl transferase 77 IU/L, alkaline phosphatase 344 IU/L, aspartate transaminase/alanine transaminase 193/305 IU/L. An esophagogastroduodenoscopy showed grade 3 esophageal varices at the lower esophagus, and the patient underwent esophageal band ligation twice. Upon liver ultrasonography, an irregular cystic lesion at the porta hepatis was incidentally found. A magnetic resonance cholangiopancreatography (MRCP) showed Todani type II choledochal cyst, and the patient was referred to SNUCH for surgery.
After admission, a follow-up MRCP (Fig. 1) and ultrasonography (Fig. 2) revealed a 1.7 cm-sized cystic lesion around the CBD and duodenum showing no definite communication with the CBD, indicative of a duodenal duplication cyst causing biliary obstruction or an unusual choledochal cyst or choledochocele. To evaluate the relationship between the cystic lesion and the duodenum, a upper gastrointestinal series and computed tomography were taken and showed mild narrowing at the proximal duodenum with no evidence of communication between the cyst and the duodenum. However, the structural continuity between the cyst and the biliary tree still remained unclear, so a percutaneous transhepatic cholangiography (Fig. 3) was performed and revealed a cystic lesion located at the confluence level between the common hepatic duct (CHD) and cystic duct (CD) with possible communication with the CD, highly suggestive of Todani type II choledochal cyst.
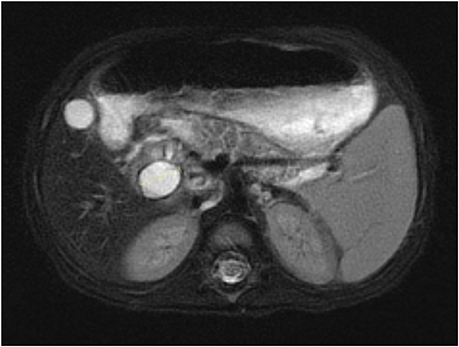
Fig. 1
Magnetic resonance cholangiopancreatography showing 1.7 cm-sized cystic lesion.
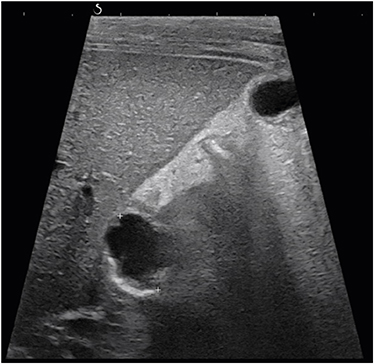
Fig. 2
Ultrasonography showing 1.7 cm-sized cystic lesion.
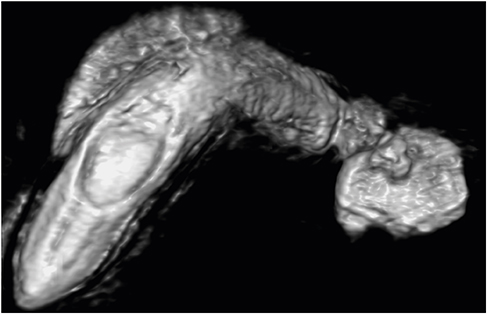
Fig. 3
Percutaneous transhepatic cholangiography showing 1.7 cm-sized cystic lesion.
The patient received laparoscopic choledochal cyst excision and Roux-en-Y hepaticojejunostomy. Intraoperatively, the cystic lesion was identified to be a diverticulum emerging from the CD, closely adjacent to the lateral side of the duodenum 1st–2nd portions (Fig. 4). There was major difficulty dissecting the CHD due to severe inflammation around the cyst, and conversion to open surgery was performed. The pathology report identified the excised cyst as a benign cystic lesion of bile duct origin with chronic active inflammation. The patient recovered well and was discharged 3 weeks after surgery without acute complications. She visited the outpatient clinic 1 week after discharge, and there were no significant abnormalities observed.
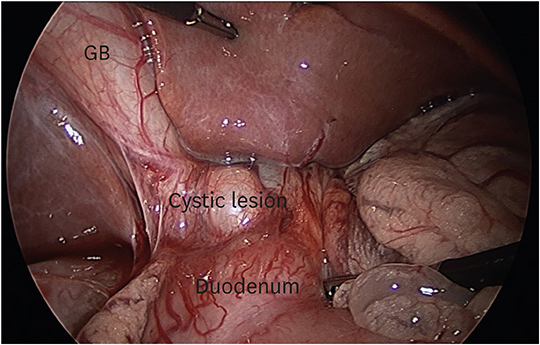
Fig. 4
Intraoperative laparoscopic view of type II choledochal cyst. The cystic lesion was identified to be a diverticulum emerging from the cystic duct.
GB: gallbladder.
Only a number of previous studies have reported on Todani type II choledochal cyst due to the extreme rarity of the disease. The largest study was done by Ouaissi et al. [6], which consisted of 19 patients diagnosed with type II choledochal cyst in multiple centers across Europe. Liu et al. [7] described a 4-year-old asymptomatic female who was incidentally diagnosed with type II choledochal cyst. Yamashita et al. [8] discussed a 58-year-old male who showed jaundice and was found to have duodenal papilla carcinoma along with type II choledochal cyst. Kono et al. [9] reported on a 40-year-old female who presented with abdominal pain and was diagnosed with type II choledochal cyst associated with pancreaticobiliary maljunction. According to these studies, the clinical presentation of patients with type II choledochal cyst can vary, including abdominal pain, jaundice, pancreatitis, cholangitis, and synchronous cancer [10]. Considerations for differential diagnoses are duodenal diverticulum, pancreatic pseudocysts, pancreatic cystic tumors, impacted gallstone, cholangiocarcinoma, biliary stricture, or gallbladder duplication [11]. Simple resection of the diverticulum is considered as the standard treatment for type II choledochal cyst, although complete surgical excision of the involved portion of the extrahepatic bile duct resection is required in a significant number of patients [12, 13]. The patient discussed in our particular case was initially admitted to the hospital at 11 months due to esophageal varices, though after esophageal band ligation, there were no remaining signs of active bleeding. This allowed for consideration of surgical resection of the choledochal cyst at 13 months of age. Long-term prognosis of type II choledochal cyst patients who received early total resection is reported to be excellent [14].
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H.Y.
Data curation: K.J., K.D.
Formal analysis: K.J., H.J.W.
Methodology: K.D.
Supervision: H.J.W., K.H.Y.
Visualization: K.J.
Writing - original draft: K.J.
