

Purpose
In the time of the global coronavirus disease 2019 (COVID-19) pandemic, preoperative confirmation of COVID-19 infection in patients in need of surgery is critical for the safety of medical staff and patients. Our purpose in this study was to analyze the experience with preoperative COVID-19 screening tests on naso-pharyngeal swabs in pediatric patients requiring surgery.
Methods
From May 1st to December 31st, 2020, we retrospectively reviewed the medical records of patients under 18 who had undergone elective and emergency pediatric surgery in Kangwon National University Hospital. During this period, all patients were tested for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) preoperatively on their nasopharyngeal smears (Allplex™ 2019-nCoV Assay, Xpert® Xpress SARS-CoV-2). Patients were divided into 2 groups before (group A) and after (group B) the introduction of Xpert® Xpress SARS-CoV-2, and the COVID-19 positive rate was confirmed by classifying the patients into 4 groups according to the risk of COVID-19 infection as assessed by clinical judgment.
Results
We screened 45 patients, of whom 35 (77.8%) were asymptomatic patients, and 10 (22.2%) had a fever. Elective surgery was done after checking the screening results in all cases. For emergency surgery patients (n=25), before the introduction of Xpert® , only 3 out of 13 (23%) patients had emergency surgery after the screening results were confirmed. However, after the introduction of Xpert® , all patients had emergency surgery after the screening results were confirmed. All patients were confirmed negative.
Conclusion
Clinical judgment on the risk of COVID-19 infection and the introduction of the Xpert® test for emergency surgery patients resulted in safe surgery for all patients without COVID-19 exposure.
In the time of the global coronavirus disease 2019 (COVID-19) pandemic, preoperative confirmation of COVID-19 infection in patients in need of surgery is critical for the safety of medical staff and patients. Our purpose in this study was to analyze the experience with preoperative COVID-19 screening tests on naso-pharyngeal swabs in pediatric patients requiring surgery.
From May 1st to December 31st, 2020, we retrospectively reviewed the medical records of patients under 18 who had undergone elective and emergency pediatric surgery in Kangwon National University Hospital. During this period, all patients were tested for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) preoperatively on their naso-pharyngeal smears (Allplex™ 2019-nCoV Assay, Xpert® Xpress SARS-CoV-2). Patients were divided into 2 groups before (group A) and after (group B) the introduction of Xpert® Xpress SARS-CoV-2, and the COVID-19 positive rate was confirmed by classifying the patients into 4 groups according to the risk of COVID-19 infection as assessed by clinical judgment.
We screened 45 patients, of whom 35 (77.8%) were asymptomatic patients, and 10 (22.2%) had a fever. Elective surgery was done after checking the screening results in all cases. For emergency surgery patients (n=25), before the introduction of Xpert®, only 3 out of 13 (23%) patients had emergency surgery after the screening results were confirmed. However, after the introduction of Xpert®, all patients had emergency surgery after the screening results were confirmed. All patients were confirmed negative.
Clinical judgment on the risk of COVID-19 infection and the introduction of the Xpert® test for emergency surgery patients resulted in safe surgery for all patients without COVID-19 exposure.
Infection of novel coronavirus disease 2019 (COVID-19) outbreak in Wuhan, China, in 2019 spread rapidly worldwide. In March 2020, the WHO declared the COVID-19 outbreak to be a pandemic [1]. Since COVID-19 shows a high transmission rate and high death rate in the elderly and vulnerable groups with underlying diseases, quarantine in hospitals where these vulnerable groups stay are very important [2]. For an in-hospital infection, transmission between inpatients is easy, complications and deaths due to infection increase, and the number of hospital rooms decreases because of the isolation of infected patients, leading to disruption of the in-hospital medical system [3]. A case can cause infection of medical staff, spreading to a wider range of patients and leading to loss of medical resources.
Establishment of preoperative COVID-19 screening guidelines for patients who need surgery is important in order to avoid infection of patients and medical staff in the operating room and postoperative respiratory complications. For suspected patients, though there are common guidelines, such as delaying surgery until there is confirmation of COVID-19 infection, checking confirmation if surgery is inevitable, and wearing personal protective equipment during surgery, guidelines should eventually be applied flexibly according to the characteristics of the medical institution and the target patient [4, 5].
In this study we analyzed experience with preoperative COVID-19 screening tests for patients in need of elective and emergency pediatric surgery at a regional secondary hospital in order to provide more efficient screening test guidelines in a similar medical environment in the future, which could result in safer operations for patients and medical staffs.
From May 1st to December 31st, 2020, we retrospectively reviewed the medical records of patients under 18 who had undergone elective and emergency surgery at the Department of Pediatric Surgery at Kangwon National University Hospital. For screening, we extracted RNA from naso-pharyngeal smears, and detected the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) virus gene by real-time reverse transcription polymerase chain reaction (RT-PCR). From May 1st to August 31st, 2020, we used the Allplex™ 2019-nCoV Assay (Seegene, Inc., Seoul, Korea; hereinafter Allplex™) [6] for both elective and emergency surgery patients; the results were reported within 6 hours (group A). Patients for elective surgery were required to get tested within 3 days prior to surgery, and patients for emergency surgery were required to be tested right after they were scheduled to get surgery. As of September 1st, 2020, excluding patients for elective surgery, we used Xpert® Xpress SARS-CoV-2 (Cepheid, Sunnyvale, CA, USA; hereinafter Xpert®) [7, 8], which allows rapid reporting of results for emergency surgery patients separately from elective surgery patients, and the results were reported within an hour (group B). For analysis of the results, we classified patients in each group into the following 4 groups according to the clinically assessed COVID-19 infection risk.
• Class I (no risk): patients who have already been tested negative at other hospitals or patients with no suspected infection, because they had no sign of fever or respiratory symptoms.
• Class II (low-risk): patients with no symptoms other than a fever of 38°C or higher.
• Class III (high-risk): patients with symptoms of upper respiratory tract infection (URI) regardless of fever, or with lesions suspicious of pneumonia on chest radiography.
• Class IV (definite): patients who had already been or had just been tested positive.
Within each group, the timing of the reporting of test results and the timing of surgery were checked according to class. For class III and class IV cases, in accordance with the surgery guidelines of the Korean Surgical Society for COVID-19 confirmed patients, medical staffs participating in surgery were required to wear level D personal protective equipment and a powered air purifying respirator, get surgery in a designated room, and have the test result checked. Cases of class I and class II had had surgery right after test results were checked [9]. This study was conducted after getting approval from the Institutional Review Board of Kangwon National University Hospital (KNUH-2021-02-009).
During the study period, a total of 49 patients underwent surgery. We analyzed the data of 45 patients, excluding 4 who had not been tested. Average age was 9.5 years, and the sex ratio of male to female was 1.8:1. Of the 20 cases (44.4%) of elective surgery, inguinal herniorrhaphy was the most common reason (15, 33.3%). Of the 25 cases (55.6%) of emergency surgery, appendectomy was the most common type (20, 44.4%). Fever was found in 10 cases (22.2%), but there were no cases of URI or pneumonia on chest radiography. All of the patients who received the screening test were found to be negative, and there were no patients who had been transferred from other hospitals who tested positive (Table 1).
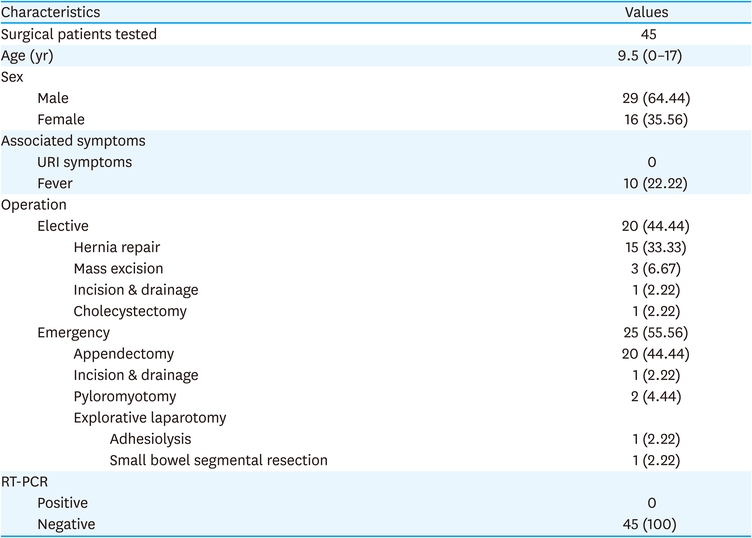
Table 1
Patient characteristics
There were 35 cases (77.8%) in class I and 10 cases (22.2%) in class II. There were no patients in class III or IV during the study period (Table 2).

Table 2
COVID-19 status according to the patient classification
For patients who needed elective surgery, we did the surgery after checking the screening results in all cases. For emergency surgery patients, before introduction of Xpert® (group A), only 3 (23%) out of 13 patients had emergency surgery after we confirmed the screening results. But after introduction of Xpert® (group B), we did emergency surgery after confirming the screening test results in all cases (Table 3). No patients had developed COVID-19-related symptoms and no follow-up tests had been conducted after surgery.

Table 3
Timing of surgery and COVID-19 screening test in patients with emergent surgical condition (n=25)
The aim of this study was to show our experiences regarding preoperative COVID-19 screening tests for pediatric surgery patients at the time of the unprecedented COVID-19 pandemic, for the purpose of making surgery safe for both patients and medical staff. Puylaert et al. [10] reported that about 1.5% of asymptomatic patients were tested as positive in the study of preoperative COVID-19 screening tests using chest computed tomography (CT) or RT-PCR on naso-pharyngeal smear samples alone or together in 2093 adult patients. Tilmans et al. [11] reported that the planned surgery could be safely done by using a combined examination of RT-PCR and chest CT. However, as is well known, the COVID-19 positive rate differs significantly from country to country, as does the range of available medical resources from country to region, so it is inevitable that appropriate modifications and combinations of test methods to suit each situation are necessary. In addition, in emergency situations where quick judgment is required, guidelines different from the ones for planned surgery will be needed. Considering the problem of radiation dose, it is usually inappropriate to routinely use chest CT as a preoperative screening test in pediatric patients. Because antigen-antibody reactions may not appear within 7 to 10 hours after onset of symptoms [12, 13, 14], they are also not suitable as a preoperative screening test that requires accurate diagnosis. For these reasons, we did preoperative screening tests with RT-PCR alone on naso-pharyngeal smears for pediatric surgery patients in this study and obtained good results.
In the first half of the study period (group A), we universally applied Allplex™ as a screening test in all patients regardless of the type of surgery. Merindol et al. [15] reported 96.9% sensitivity and 100% specificity of Allplex™ for SARS-CoV-2, suggesting the usefulness of Allplex™ as a screening test. Xpert®, which we used in emergency surgery patients in the second half of the study period (group B), could report results within 45 minutes by integrating the processing of naso-pharyngeal smears, RNA extraction, and RT-PCR. It also showed a positive agreement of 99.5%–100% and a negative agreement of 95.8%–100% with the existing RT-PCR-based test results, including Allplex™ [16, 17]. However, since Xpert® costs 5 times more than Allplex™, it is necessary to selectively apply it to appropriate patient groups.
Our institution changed emergency-room operation guidelines after COVID-19 pandemic to accommodate only a limited number of people in the same space in order to avoid possible transmission between patients, which inadvertently lead to reduced patient turnover rate in emergency-room. Our institute is a regional secondary care center, where mild-symptom patients are in the majority, and most cases of emergency surgery in children were for acute appendicitis. Because most patients with acute appendicitis visit the hospital with a fever, we performed appendectomy first for patients with only a fever but without respiratory symptoms in the first half of the screening test period (group A), and checked the test results later. However, for pediatric patients, because a high viral load may be seen in asymptomatic cases, and because their symptoms end up being mild, preoperative COVID-19 screening is essential regardless of the presence or absence of visible symptoms [18, 19]. This problem could be overcome by introduction of Xpert® in the latter half of the screening test period (group B), allowing all emergency surgery patients to be checked for preoperative test results prior to surgery.
Of the 4 cases where preoperative screening was not done, 3 were missed because specific guidelines were not provided at the beginning of introducing screening tests. One case was a newborn infant with gastroschisis for whom the test was not possible, since the surgery was done at the time of birth.
This study has several limitations. In Group A patients, the fact that surgery was done without waiting for the screening test results to be reported, because there were no specific respiratory symptoms, could be regarded as an insufficient measure and thus as a weakness of this result. Though there are no clear guidelines for pediatric surgical patients yet, we think screening tests such as Xpert® that can report results quickly in real time could be a good alternative measure.
Second, though Lin et al. [20] confirmed 12 cases (0.93%) of COVID-19 in preoperative screening of 1,295 pediatric surgery patients, our study was done with a small sample; since we had no cases of classes III or IV, it was difficult to confirm the practical benefits of screening tests. Having such a small sample reflects the realistic situation of regional secondary care centers, in that people prefer to go to or be transferred to a large hospital if their state is judged to be even a little serious.
Third, though we did not do postoperative RT-PCR follow-up during this study period, there were no positive cases of COVID-19 confirmed after surgery. Depending on the results of further studies in the future, postoperative RT-PCR follow-up could be another way to improve the safety of patients and medical staff.
In conclusion, clinical judgment on COVID-19 infection risk and the introduction of the Xpert® test for emergency surgery patients allowed efficient preoperative testing during the study period. There were no confirmed cases of patients before surgery and no cases of medical staff who were exposed to COVID-19 during surgery; so, the operation could be done safely for both patients and medical staff.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: M.S.B.
Data curation: L.K.J., M.S.B., C.S.J., C.G., P.S.B., H.S.K., K.Y.H., K.H.
Formal analysis: L.K.J., M.S.B.
Investigation: L.K.J., M.S.B.
Methodology: L.K.J., M.S.B.
Supervision: M.S.B.
Validation: M.S.B.
Writing - original draft: L.K.J.
Writing - review & editing: M.S.B.
