

Purpose
The purpose of the article was to review the thirteen years of experience and evaluate the usefulness of open inguinal hernia repair (OIHR) with transinguinal laparoscopic exploration of contralateral groin (TILE), the prevalence of contralateral patent processus vaginalis (CPPV), and the incidence of metachronous inguinal hernia after negative laparoscopic examination in pediatric patients with unilateral inguinal hernia.
Methods
We analyzed data from children aged 15 years and younger who underwent inguinal hernia repair between 2007 and 2019. We performed an OIHR with TILE to assess the contralateral groin, and TILE was accomplished via ipsilateral hernia sac. We collected the medical records and analyzed demographics, operation-related information, including the prevalence of CPPV and the incidence of metachronous contralateral inguinal hernia (MCIH).
Results
Of the 1,702 patients with unilateral inguinal hernia, 440 patients (25.9%) had CPPV. The risk factors of CPPV were younger age, female, and left inguinal hernia. The operation results of OIHR with TILE, such as postoperative pain, cosmetic results, recurrence rate, and recovery time was similar to other reports, including open and laparoscopic repair, if not better than LIHR. There were no complications associated with transinguinal laparoscopic exploration. Also, 28 patients (2.2%) with obliterated PV still developed an MCIH later.
Conclusion
OIHR with TILE is valuable and safe to detect CPPV in the laparoscopic era. There has been some development (2.2%) of MCIH after negative laparoscopic exploration, which suggested that even though PPV is a significant risk factor for developing a pediatric inguinal hernia, other factors also might be involved in the pathophysiology of pediatric inguinal hernia. OIHR with TILE may be a good surgical option because it compensate for the weakness of OIHR alone and has some advantages of LIHR alone. Two methods can also complement each other and might be tailored to the particular needs of individual patients.
The purpose of the article was to review the thirteen years of experience and evaluate the usefulness of open inguinal hernia repair (OIHR) with transinguinal laparoscopic exploration of contralateral groin (TILE), the prevalence of contralateral patent processus vaginalis (CPPV), and the incidence of metachronous inguinal hernia after negative laparoscopic examination in pediatric patients with unilateral inguinal hernia.
We analyzed data from children aged 15 years and younger who underwent inguinal hernia repair between 2007 and 2019. We performed an OIHR with TILE to assess the contralateral groin, and TILE was accomplished via ipsilateral hernia sac. We collected the medical records and analyzed demographics, operation-related information, including the prevalence of CPPV and the incidence of metachronous contralateral inguinal hernia (MCIH).
Of the 1,702 patients with unilateral inguinal hernia, 440 patients (25.9%) had CPPV. The risk factors of CPPV were younger age, female, and left inguinal hernia. The operation results of OIHR with TILE, such as postoperative pain, cosmetic results, recurrence rate, and recovery time was similar to other reports, including open and laparoscopic repair, if not better than LIHR. There were no complications associated with transinguinal laparoscopic exploration. Also, 28 patients (2.2%) with obliterated PV still developed an MCIH later.
OIHR with TILE is valuable and safe to detect CPPV in the laparoscopic era. There has been some development (2.2%) of MCIH after negative laparoscopic exploration, which suggested that even though PPV is a significant risk factor for developing a pediatric inguinal hernia, other factors also might be involved in the pathophysiology of pediatric inguinal hernia. OIHR with TILE may be a good surgical option because it compensate for the weakness of OIHR alone and has some advantages of LIHR alone. Two methods can also complement each other and might be tailored to the particular needs of individual patients.
Inguinal hernia is the most common surgical disease in children, with an overall incidence rate of 0.8%–4.4%. Most patients are diagnosed with a unilateral hernia, and bilateral hernias are only observed in 10%–20% of patients [1, 2]. Meanwhile, about 3.6%–29% [3] of patients with unilateral inguinal hernias develop metachronous hernias on the contralateral side after surgery. Since this metachronous contralateral inguinal hernia (MCIH) requires subsequent additional surgery, the parental concern is the need for a second operation and anesthesia and its complication risk or surgery cost. Therefore, if possible, it is necessary to predict the MCIH occurrence in advance and prevent it.
Patent processus vaginalis (PPV) is known as the leading cause of pediatric inguinal hernia [4], so checking the patency of processus vaginalis (PV) on the other side before or during surgery and performing the simultaneous operation is a beneficial method to prevent unnecessary additional surgery [5].
With the advent of laparoscopy, laparoscopic inguinal hernia repair (LIHR) in children has become an option of treatment, and it has been increasingly used in recent years. The proponents of LIHR proclaim that the advantages of LIHR are minimal invasiveness, smaller incision with cosmetic results, detection of contralateral patent processus vaginalis (CPPV), and reduced incidence of MCIH [6]. However, some studies have shown that the procedure also has disadvantages. Some of these include consumption of many resources, longer operative time, and metabolic change of young children due to the CO2 pneumoperitoneum [6, 7]. Moreover, some existing studies report laparoscopic surgery has a higher recurrence rate than open surgery [8]. Thus, the use of laparoscopy as the primary surgical procedure for inguinal hernia in children remains controversial. In this background, we attempted to confirm the usefulness of the open inguinal hernia repair (OIHR) with transinguinal laparoscopic exploration of contralateral groin (TILE) by reviewing the operative data and tracking the prevalence of CPPV and the incidence of MCIH after negative examination for 13 years.
We analyzed the retrospective data of children aged 15 years and younger who underwent OIHR between January 2007 and December 2019. During the 13-year study period, 2,266 patients underwent OIHR. One hundred fifty-two patients had a bilateral inguinal hernia. Four hundred eight patients were lost to follow-up, and four patients with a unilateral inguinal hernia did not undergo contralateral transinguinal exploration.
Contralateral transinguinal laparoscopic exploration was performed on 1702 patients with a unilateral inguinal hernia. According to the results, the parents of all patients were informed about the procedure, and they provided consent for performing contralateral laparoscopic examination during surgery and providing additional surgery of the contralateral side.
Patients were admitted to the hospital in the afternoon or evening before the operation day and kept fasting for 4 hours before surgery. Patients were discharged in the afternoon or evening on the operation day once they were stable hemodynamically and tolerating feeding well.
An inguinal skin crease incision was made on the affected side about 1cm in length. The Scarpa's fascia was incised and the external oblique aponeurosis was opened. The urogenital fascia was picked up and the spermatic cord and gonadal vessels, and vas deferens were carefully dissected from the hernia sac. The hernia sac was divided.
A 2.5-mm trocar was inserted into the abdominal cavity through the opened ipsilateral hernia sac and secured with a silk tie. Carbon dioxide insufflation was accomplished at a pressure of 6–8 mmHg. A 70° telescope was inserted through the trocar to check the contralateral internal ring. Positive laparoscopic exploration was defined as the presence of an apparent defect in the contralateral internal ring, bulging of the contralateral side during gas inflation, palpable gas or crepitus in the contralateral groin, or inner bubble around the internal ring visualized during external compression of the contralateral groin [9] (Fig. 1). We use several adjunctive maneuvers such as extermal compression or veil manipulation using telescope tip. If there was still suspicion of patency, surgery proceeded, so no chance of occult PPV was present.
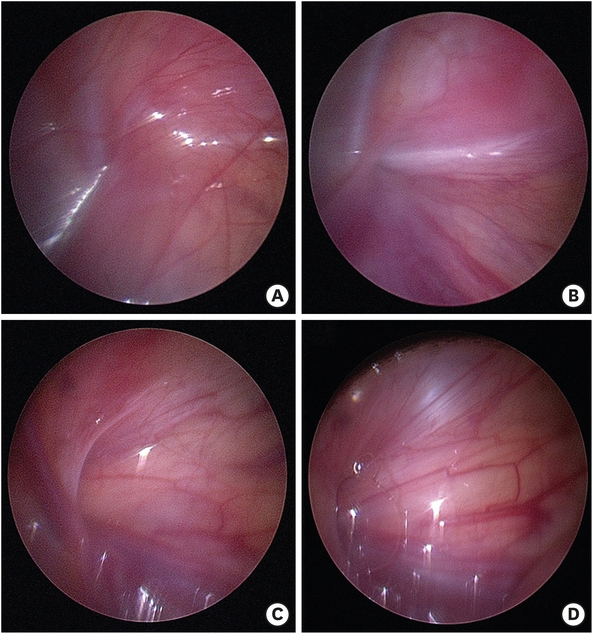
Fig. 1
Laparoscopic finding of contralateral internal ring: (A, B) presenting negative contralateral patent processus vaginalis, (C, D) presenting positive contralateral patent processus vaginalis. (A) No veil. (B) Concave type but not perforated. (C) Defect in the contralateral internal ring. (D) Bubble visualized during external compression.
After exploration, the scope was withdrawn and the trocar was removed. The neck of the hernia sac was suture ligated with black silk and resected. The incised aponeurosis of the external oblique muscle and Scarpa’s fascia were closed. After subcuticular suture, the skin was closed with a skin bond. If a contralateral hernia or CPPV was identified on TILE, the contralateral hernia repair was performed.
Demographic data such as those on age, sex, and the side of hernia were collected. Statistical analysis was performed using the t-test with the Statistical Package for the Social Sciences software, and a cross-analysis was conducted using the chi-square test. A p-value <0.05 was considered statistically significant.
All procedures involving human participants were conducted in accordance with the ethical standards of the institutional research committee (CNUH 2020-03-022) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Consent for research was waived because the study is a retrospective review.
In total, 2,266 pediatric patients underwent open repair for an inguinal hernia during the 13-year study period. However, 412 who did not undergo transinguinal laparoscopic exploration or were lost to follow-up were excluded from the study. Finally, 1,854 patients were included in the analysis (Fig. 2).
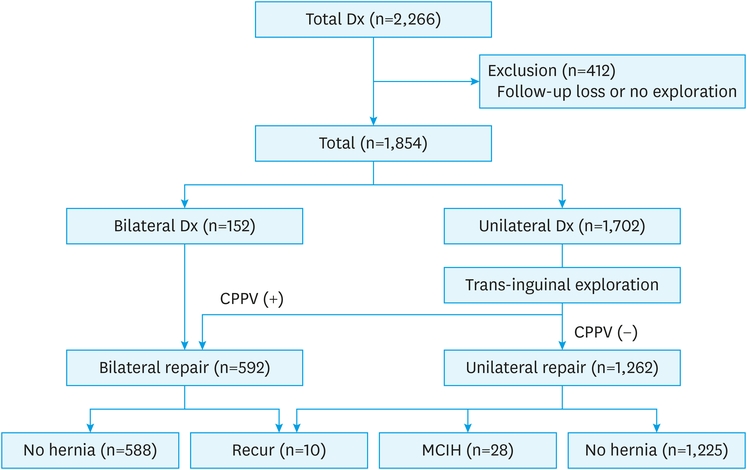
Fig. 2
Numbers of pediatric patients with inguinal hernia.
Dx, Diagnosis of inguinal hernia; CPPV, contralateral patent processus vaginalis; MCIH, metachronous contralateral inguinal hernia.
There were 1,179 boys and 675 girls. The average age at surgery was 38.3 months (n=1,011 children, aged over 2 years and n=843, aged below 2 years). The preoperative diagnoses were right hernia (n=958), left hernia (n=744), and bilateral hernia (n=152). The bilateral hernia was more common in younger children, particularly those aged below two years. (Table 1).
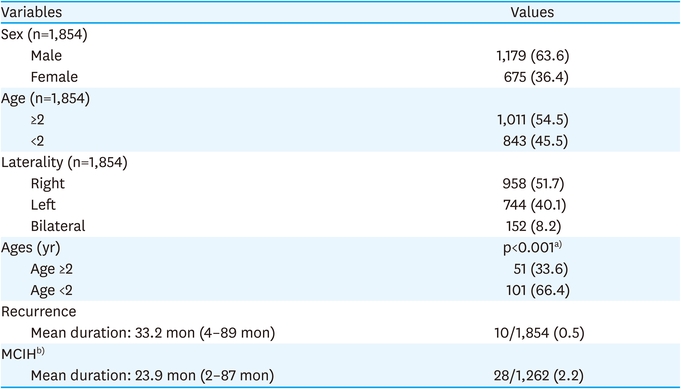
Table 1
Patients demographic data
TILE was performed on 1,702 patients who were diagnosed with unilateral inguinal hernia before surgery. Based on the laparoscopic examination, 440 patients presented with CPPV. There were 188 girls and 252 boys with positive CPPV. The proportion of girls with CPPV was higher than that of boys. In addition, 258 patients with positive CPPV were under two years old. Patients with CPPV were more likely to be younger. The incidence of CPPV was higher in patients aged below two years. Also, The CPPV was detected more frequently in the left inguinal hernia. 227 CPPVs were found in the right inguinal hernia, and 213 CPPVs were detected in the left inguinal hernia (Table 2).
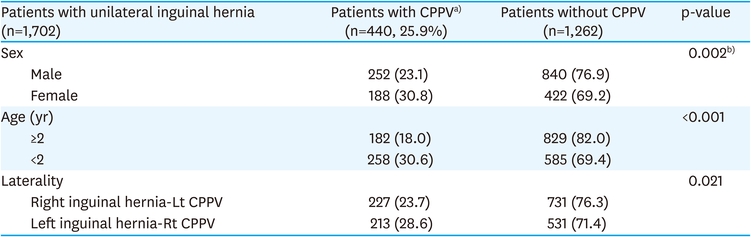
Table 2
Findings of trans-inguinal laparoscopic exploration
In total, 28 (2.2%) children without CPPV based on a thorough contralateral transinguinal exploration developed MCIH, which required subsequent additional operation. Twenty boys and eight girls were diagnosed with MCIH. MCIH occurred in 13 of the right inguinal hernia patients and 15 of the left hernias. The average age of patients who developed MCIH was 37 months (n=16, children aged over 2 years and n=12, children aged below two years). There was no correlation between gender, age, and laterality of initial hernia and the occurrence of MCIH (Table 3).
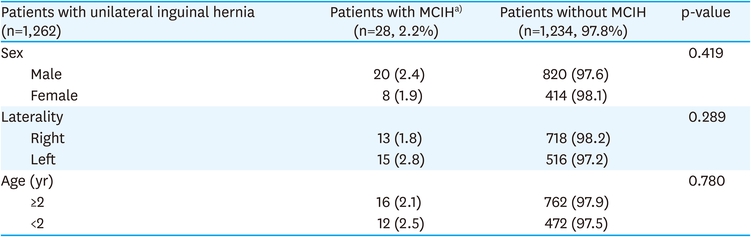
Table 3
Risk factors of MCIH with negative laparoscopic exploration
There were 10 cases (0.5%) of recurrence (one girl: nine boys). All the recurrences were detected in the first hernia side. One boy initially had a right-side hernia repair without CPPV, but the Lt-CPPV was found in the second operation (Table 4).
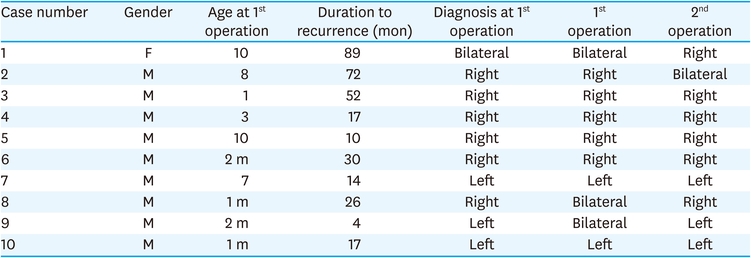
Table 4
The cases of recurrence
Currently, many centers perform LIHR in pediatric inguinal hernias. The biggest weakness of OIHR compared to LIHR is the inability to evaluate CPPV. By implementing TILE together with OIHR, it is thought that this weakness can be compensated. According to previous studies, TILE requires very short additional time to OIHR alone, and it can also be expected to reduce medical expenses by lowering the MICH rate [10]. OIHR surgery requires only 1 to 1.5 cm incision in the inguinal crease and TILE needs no additional incision. It is almost invisible with naked eyes after healing, thereby annuls the cosmetic effects of LIHR. The recurrence rate of OIHR would be similar, if not better, than LIHR [6, 11]. Moreover, complications associated with laparoscopic surgery are rarely observed in TILE. Because laparoscope is used for a very short time, which means the maintenance time of the CO2 pneumoperitoneum is also very short, so it’s thought that the risk of metabolic change is low. In addition, since only a telescope is inserted into the peritoneal cavity and no other laparoscopic instruments are used, the possibility of injury caused by these instruments is very low.
With the wide acceptance of laparoscopic surgery, the identification of CPPV is becoming more straightforward, and CPPV found during laparoscopic surgery is reported to occur up to 21%–47% [6, 12]. In this study, CPPV was confirmed in 25.9%, after which high ligation was performed, and no MCIH occurred in the patients who underwent surgery. In this study, the incidence of CPPV was significantly higher in younger age (<2 years old), female gender, and left side hernia. This finding is consistent with the results of studies that reported the incidence of other MCIH [13, 14]. It is also known that bilateral hernia is more frequently diagnosed in female patients, younger age, and left-sided hernia. Although it cannot be a piece of direct evidence that the occurrence of CPPV causes the occurrence of MCIH, this finding suggests some association. Therefore, it would be better to check the other side with a laparoscope for a patient with a high risk of CPPV and MCIH.
CPPV is reported in about 30% of unilateral inguinal hernia patients [13]. However, despite the relatively high prevalence of CPPV in unilateral childhood inguinal hernia, some pediatric surgeons argue that a PPV at exploration does not necessarily mean possible development of a hernia at a later stage, so the routine investigation of the contralateral inguinal region is not needed [15]. It is also a controversial question whether surgery is necessary for detected CPPV without any symptoms found because not all PPVs occur as a hernia [16]. However, the follow-up period had been very limited to the pediatric age period in most of the ‘don’t need report’. The incidence of inguinal hernias has a bimodal distribution, with peaks at early childhood and old age [17]. Also, a prospective cohort study indicated that asymptomatic PV is a risk factor for developing inguinal hernia in adults [18]. So, to the best of the author’s knowledge, CPPV should be viewed as a possible factor in developing inguinal hernia beyond the pediatric period. Moreover, considering that the patient is a young child, it is often impossible to discriminate whether it is a simple asymptomatic CPPV or hidden hernia. That is why the authors performed routine transinguinal laparoscopic contralateral groin exploration.
One interesting finding in this study was that 28 patients developed MCIH despite negative laparoscopic exploration. There are three possible causes for this to be thought of (1) CPPV exists but is not found at the time of surgery; (2) PPV obliterated but recanalized due to surgery; (3) Completely new PPV occurs again (It can be thought of as acquired indirect hernia).
When it comes to the first theory, according to the recent meta-analysis, transinguinal approach, narrow scope angle, high abdominal pressure, and narrow CPPV definition has been reported as related risk factors for MCIH [19]. In our study, transinguinal approach may be associated with a lower CPPV rate compared to the existing literature. Not only the limitation of transinguinal camera angle but also the lack of laparoscopic instruments to help the diagnosis could affect the low CPPV diagnosis rate. But the authors used a 70-degree wide-angle telescope, low abdominal pressure, and the use of a broad definition of PPV. Therefore, it is thought that the limitations of the transinguinal approach could be covered to some extent.
In the case of the second hypothesis, there is a report that a drastic morphologic change occurs in the opposite obliterated internal ring due to the internal inguinal ring narrowing during surgery, which causes the obliterated inguinal ring to open again [20, 21]. In previous studies, most MCIH occurred within one year or two years, but in our research, the average interval of MCIH was 23.9 months. Assuming that the internal inguinal ring is reopened due to a sudden morphological change and if a hernia occurs due to this effect, symptoms have likely occurred shortly after the surgery.
Therefore, other factors other than simply PPV play a part in the pathophysiology of the MCIH with a negative PV. As in adults, peritoneal protruding gradually may be occurred inside the inguinal canal due to the lack of defense mechanism of the inguinal canal [22, 23], and it can be considered that a hernia occurred due to this. To confirm this, additional research is needed.
This study has several limitations. The is a retrospective study, and the follow-up for MCIH is relatively short, so beyond the pediatric age, adulthood changes could not be confirmed.
Laparoscopic examination via the hernia sac during open high ligation is a useful diagnostic tool to confirm the presence of CPPV. We were able to detect contralateral PPV in about 25.9% of patients. Some MCIH cases had negative CPPV, which means other mechanisms other than PPV were involved in developing an inguinal hernia.
The proclaimed advantages of LIHR were also found in OIHR with TILE. Although all surgical techniques have limitations of one sort or another, the benefits of one surgical technique don’t necessarily mean the disadvantages of the other technique, especially in pediatric inguinal hernia repair.
OIHR with TILE may be a good surgical option because it compensate for the weakness of OIHR alone and has some advantages of LIHR alone. Two methods can also complement each other and might be tailored to the particular needs of individual patients.
Conflicts of interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: P.J., S.J.
Formal analysis: K.M., P.J.
Investigation: K.M., P.J.
Methodology: P.J.
Writing - original draft: K.M.
Writing - review & editing: P.J., S.J.
