
 , Sung Min Lee1
, In Geol Ho1
, Kyong Ihn1
, Seok Joo Han1
, Sung Min Lee1
, In Geol Ho1
, Kyong Ihn1
, Seok Joo Han1

Purpose
Most patients with perinatally detected subhepatic cysts receive information suggestive of a suspected diagnosis of choledochal cyst (CC). However, it is not uncommon to be finally diagnosed with cystic biliary atresia (CBA), a disease with a more unfavorable prognosis. This study aimed to investigate the distribution of the final diagnoses of perinatally detected subhepatic cysts and to compare patients diagnosed with CC and CBA.
Method
We performed a retrospective review of patients with subhepatic cysts detected using ultrasonography during perinatal period, between January 2012 and December 2022.
Result
This retrospective study included 52 patients with perinatal subhepatic cysts. Of these, 71.2% (37/52) were diagnosed with CC, 15.4% (8/52) with CBA, and 5.8% (3/52) with duplication of the alimentary tract. Only 1.9% (1/52) of the patients were diagnosed with biliary atresia, gallbladder duplication, mesenteric lymphatic malformation, or were normal. Of all patients, 86.5% (45/52) were diagnosed with CC or CBA, with CBA accounting for 17.8% (8/45). There were no statistically significant differences between the CC and CBA groups regarding the gestational age at which the cyst was first detected and the final size of the cyst measured on prenatal ultrasound.
Conclusion
Subhepatic cysts detected during the perinatal period are typically diagnosed as CC. However, this study revealed that 15.4% of all patients were diagnosed with CBA, despite no significant differences in prenatal ultrasound findings. Therefore, it is essential to consider the possibility of CBA in cases of perinatally detected subhepatic cysts.
Most patients with perinatally detected subhepatic cysts receive information suggestive of a suspected diagnosis of choledochal cyst (CC). However, it is not uncommon to be finally diagnosed with cystic biliary atresia (CBA), a disease with a more unfavorable prognosis. This study aimed to investigate the distribution of the final diagnoses of perinatally detected subhepatic cysts and to compare patients diagnosed with CC and CBA.
We performed a retrospective review of patients with subhepatic cysts detected using ultrasonography during perinatal period, between January 2012 and December 2022.
This retrospective study included 52 patients with perinatal subhepatic cysts. Of these, 71.2% (37/52) were diagnosed with CC, 15.4% (8/52) with CBA, and 5.8% (3/52) with duplication of the alimentary tract. Only 1.9% (1/52) of the patients were diagnosed with biliary atresia, gallbladder duplication, mesenteric lymphatic malformation, or were normal. Of all patients, 86.5% (45/52) were diagnosed with CC or CBA, with CBA accounting for 17.8% (8/45). There were no statistically significant differences between the CC and CBA groups regarding the gestational age at which the cyst was first detected and the final size of the cyst measured on prenatal ultrasound.
Subhepatic cysts detected during the perinatal period are typically diagnosed as CC. However, this study revealed that 15.4% of all patients were diagnosed with CBA, despite no significant differences in prenatal ultrasound findings. Therefore, it is essential to consider the possibility of CBA in cases of perinatally detected subhepatic cysts.
Fetal abdominal cysts are rarely encountered and are most commonly identified during the third trimester [1]. Abdominal cysts are associated with various conditions, ranging from normal to serious, and may require surgical interventions after birth. Subhepatic cysts can be diagnosed as choledochal cyst (CC), alimentary tract duplication, lymphatic malformation, or cystic biliary atresia (CBA) [1-3]. In cases where a subhepatic cyst is discovered during the perinatal period, many are initially suspected of having CC. However, it is not uncommon to diagnose CBA instead of CC after additional evaluations, such as magnetic resonance imaging (MRI) or hepatobiliary scan.
Similarities exist between some cases of CC and CBA. Notably, both entities can present with obstructive jaundice, and a subhepatic cyst in hilar area can be observed on imaging evaluations such a prenatal ultrasound or MRI [4,5]. However, it is typically known that CBA’s prognosis is worse than that of CC [4]. Therefore, overlooking the possibility of CBA in patients with subhepatic cysts observed during the perinatal period may lead to potential issues.
This study aimed to investigate the distribution of the final diagnoses of perinatally detected subhepatic cysts, and compare the characteristics of patients diagnosed with CC and CBA.
We performed a single-center retrospective review between January 2012 and December 2022. Patients identified as having a subhepatic cyst on ultrasound either during the prenatal period or within the first week after birth and who underwent both evaluation and surgery for the cyst in our institution were included in this study. Patient who only underwent cyst evaluation at our institution and did not undergo surgery were excluded. We retrospectively reviewed the medical records of the included patients to collect data on sex, gestational age, birth weight, final diagnosis, surgical procedure, prenatal ultrasound findings, preoperative ultrasound findings, and laboratory test results. In cases where perinatal ultrasound images were unavailable owing to the examination being performed at other hospitals, the perinatal ultrasound findings were summarized based on the statements provided by the patient’s parents. This study was approved by the Institutional Review Board and Ethics Committee of Severance Hospital (approval number: 4-2023-0552).
Statistical analyses were performed using the SPSS software (version 18.0; SPSS Inc., Chicago, IL, USA). The variables are expressed as median values with ranges or percentages. Mann-Whiney U and Fisher’s exact tests were used to compare the CC and CBA groups. Statistical significance was set at p<0.05.
A total of 52 patients were identified to undergo surgery for perinatally detected subhepatic cyst (Table 1). Among them, CC was the most commonly diagnosed disease, accounting for 71.2% (37/52), followed by CBA at 15.4% (8/52). Alimentary tract duplications were diagnosed in 3 patients (5.8%), and non-CBA, gallbladder duplication, and mesenteric lymphatic malformation were observed in one patient each.
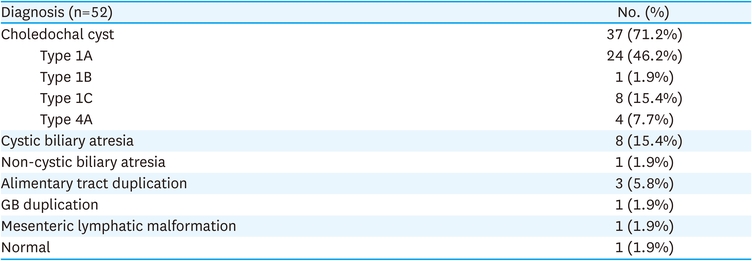
Table 1
Diagnoses of perinatally detected subhepatic cyst
Forty-five of the 52 patients (86.5%) were diagnosed with CC or CBA, indicating that most cases with perinatally detected subhepatic cysts were associated with biliary system disorders. Among these, CBA accounts for 17.8%. Table 2 compares patients diagnosed with CC and CBA. The two groups had no significant differences in prematurity (8.1% vs. 12.5%, p=0.56), birth weight (median, 3.16 vs. 3.28 kg, p=0.59, and combined anomalies (10.8% vs. 12.5%, p=1.00). There were statistically significant differences between the two groups in the level of direct bilirubin (median, 0.7 vs. 3.6 mg/dL, p<0.01), γ-glutamyl transferase (γ-GT) (median, 136.0 vs. 431.5 IU/L, p=0.02), aspartate aminotransferase (AST; median, 42 vs. 60 IU/L, p=0.03), and alkaline phosphatase (ALP; median, 219 vs. 404 IU/L, p=0.04). Of the 45 patients, 43 had a subhepatic cyst observed on prenatal ultrasound, whereas cysts were first observed within the first week after birth in two patients. One patient had intrauterine growth restriction (IUGR), but no cyst was observed on the prenatal ultrasound performed at our institution. However, a cyst was detected by ultrasonography after birth. The other patient was referred from another hospital with hematochezia, and a cyst was incidentally observed on ultrasonography. There was no record of prenatal ultrasound images, and the parents provided no statements regarding the prenatal ultrasound for this patient. Notably, both the patients were diagnosed with CC.
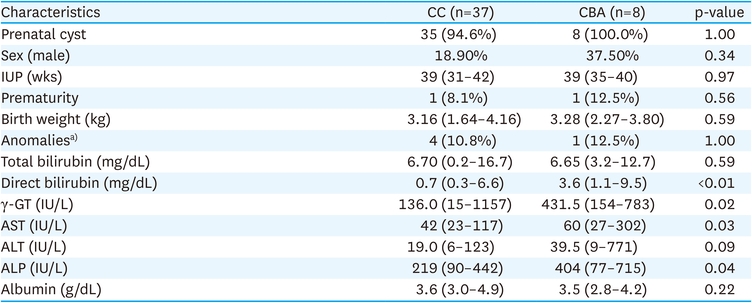
Table 2
Comparison of patients diagnosed with CC and CBA
The gestational age at which cysts were initially detected on prenatal ultrasound and the size of the cysts measured at the latest assessment were compared between patients diagnosed with CC and those diagnosed with CBA (Table 3). These values did not significantly differ between the two groups. In addition, there were no differences in the cyst size measured using preoperative ultrasonography. However, ultrasound imaging or records could be used to obtain information about gestational age and latest size in only a few patients; this posed limitation in the analysis.

Table 3
Comparison of ultrasonographic findings
In this study, among patients with perinatally detected subhepatic cysts, 71.2% were diagnosed with CC. The next most common diagnosis was CBA (15.4%). Furthermore, based on the medical records, patients with CBA did not receive any information regarding the possibility of CBA associated with the observed prenatal cyst. Instead, they were informed about the possibility of CC during the prenatal or immediate postnatal periods.
CBA and CC can potentially cause obstructive jaundice and are both observed as subhepatic cysts in hilar area on ultrasonography; however, they differ significantly in their prognosis. CC is associated with the possibility of malignant transformations such as cholangiocarcinoma or gallbladder cancer. However, after complete excision, long-term outcomes are favorable [6,7]. In contrast, biliary atresia (BA) often experiences progression to liver cirrhosis even after Kasai portoenterostomy, with a two-year native liver survival rate of approximately 50%. Delayed surgery can cause severe liver damage requiring immediate liver transplantation [8-11]. CBA has a relatively favorable prognosis compared with BA, but there is a clear difference in prognosis between CC and CBA. Therefore, differentiation is important [4,12].
Several previous studies have compared patients with CC and CBA. No significant differences were observed in these studies regarding sex, age, or body weight. However, direct bilirubin, AST, and alanine aminotransferase (ALT) levels were significantly higher in the CBA group, and total bilirubin levels varied across studies. The level of γ-GT either showed no significant difference or was not analyzed. Notably, some studies have reported that the size of cysts on preoperative ultrasonography was significantly smaller in the CBA groups [4,5,13,14]. This study found no significant differences in sex, age, and body weight; however, there were significant differences in the levels of direct bilirubin, AST, and γ-GT. In addition, no significant difference was observed in cyst size.
Previous studies have not shown statistically significant differences in cyst size at specific gestational age. However, there was a tendency for the cyst size to remain constatnt or gradually decreased in the CBA group, while to increase in the CC group [14,15]. In this study, when comparing prenatal ultrasound findings of subhepatic cysts in patients with CC and CBA, there were no significant differences in the gestational age at which the cysts were first detected and in the size of the cysts. However, dut to the limited number of patients with accurately documented gestational age and cyst size, there were limitations in the analysis, and we were unable to analyze changes in cyst size. Interestingly, in cases of non-CBA diagnosed in this study, the cyst was also observed on prenatal ultrasound. However, its size gradually decreased, and was invisible on the last prenatal ultrasound. This patient was evaluated early suspicion of non-CBA based on these findings. Well-documented ultrasound findings and imaging allowed for a rapid diagnosis and surgery. Therefore, this case suggests that closely monitoring of perinatally detected subhepatic cysts through ultrasound can be helpful for the final diagnosis.
This study has a few limitations. First, this retrospective study was conducted at a single institution and included a small number of patients. Therefore, the generalization of the results to a broader population may be limited. In addition, regarding prenatal ultrasound findings, not all images were reviewed, and some were based on parental statements, thereby introducing limitations. Future research could be designed as multicenter study with a larger sample size, and the data could be based on a direct review of images rather than relying on parental statements to enhance the study’s reliability.
In conclusion, this study demonstrated that subhepatic cysts detected during the perinatal period are most commonly diagnosed as CC. However, a considerable number (15.4%) of the patients were diagnosed with CBA. Furthermore, continuous and accurate ultrasound records were able to assist in the final diagnosis. Therefore, it is essential to be aware of the possibility of CBA diagnosis in subhepatic cysts detected during the perinatal period and the importance of careful ultrasound monitoring.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Y.H.J., H.S.J.
Data curation: Y.H.J.
Formal analysis: Y.H.J.
Investigation: Y.H.J., H.S.J.
Methodology: Y.H.J., H.S.J.
Project administration: Y.H.J., H.S.J.
Resources: H.S.J., I.K.
Supervision: H.S.J.
Validation: H.S.J., I.K.
Writing - original draft: Y.H.J.
Writing - review & editing: L.S.M., H.I.G., I.K., H.S.J.
