
 , Suhyun Ha1
, Hyunhee Kwon1
, Jung-Man Namgoong1
, Hee Mang Yoon2
, Pyeong Hwa Kim2
, Dae Yeon Kim1
, Suhyun Ha1
, Hyunhee Kwon1
, Jung-Man Namgoong1
, Hee Mang Yoon2
, Pyeong Hwa Kim2
, Dae Yeon Kim1

Purpose
Complicated vascular anomalies, characterized by encasing vital organ or diffusely locating unresectable lesion, pose therapeutic challenges with limited response to conventional treatment such as surgical resection or sclerotherapy. Sirolimus, an mammalian target of rapamycin inhibitor, has shown promising therapeutic effects in patients with vascular anomalies by inhibiting vascular endothelial growth factor, as reported in several studies. Here, we analyzed the treatment outcomes of patients who received sirolimus for complicated vascular anomalies at our institution.
Methods
Patients treated with sirolimus at the Department of Pediatric Surgery, Asan Medical Center from January 2018 to December 2021 were included. Sirolimus was administered twice daily at a dose of 0.8 mg per body surface area (BSA), with dose adjustments to achieve a target drug concentration of 8–12 ng/mL. Adverse drug effects and therapeutic responses were periodically assessed. Treatment efficacy was evaluated based on clinical findings pre- and post-sirolimus administration, absolute volume reduction of lesions through imaging tests (magnetic resonance imaging; MRI), and relative volume reduction adjusted to the patient's BSA.
Results
There were 16 females (50.0%) and 16 males (50.0%), with a median follow-up period of 41 months after sirolimus administration. Vascular anomaly types included lymphatic malformations (41%), venous malformations (28%), lymphovenous malformations (19%), and others (12.5%). The most common adverse effect was oral ulcer (6 patients). MRI volumetry revealed volume decreases in 17 patients (53.1%) with 22 patients (71%) exhibited lesion decreases relative to BSA. Notably, 9 patients (28.1%) had markedly decreased volume reduction based on absolute volume, and 12 (38.7%) based on volume compared to BSA.
Conclusion
Over a 2-year follow-up, sirolimus was effective in treating patients with complicated vascular anomalies, when administered with cautious consideration of side effects. A multidisciplinary approach is needed for evaluating treatment outcomes in these patients, necessitating further long-term research on adverse effects.
Complicated vascular anomalies, characterized by encasing vital organ or diffusely locating unresectable lesion, pose therapeutic challenges with limited response to conventional treatment such as surgical resection or sclerotherapy. Sirolimus, an mammalian target of rapamycin inhibitor, has shown promising therapeutic effects in patients with vascular anomalies by inhibiting vascular endothelial growth factor, as reported in several studies. Here, we analyzed the treatment outcomes of patients who received sirolimus for complicated vascular anomalies at our institution.
Patients treated with sirolimus at the Department of Pediatric Surgery, Asan Medical Center from January 2018 to December 2021 were included. Sirolimus was administered twice daily at a dose of 0.8 mg per body surface area (BSA), with dose adjustments to achieve a target drug concentration of 8–12 ng/mL. Adverse drug effects and therapeutic responses were periodically assessed. Treatment efficacy was evaluated based on clinical findings pre- and post-sirolimus administration, absolute volume reduction of lesions through imaging tests (magnetic resonance imaging; MRI), and relative volume reduction adjusted to the patient's BSA.
There were 16 females (50.0%) and 16 males (50.0%), with a median follow-up period of 41 months after sirolimus administration. Vascular anomaly types included lymphatic malformations (41%), venous malformations (28%), lymphovenous malformations (19%), and others (12.5%). The most common adverse effect was oral ulcer (6 patients). MRI volumetry revealed volume decreases in 17 patients (53.1%) with 22 patients (71%) exhibited lesion decreases relative to BSA. Notably, 9 patients (28.1%) had markedly decreased volume reduction based on absolute volume, and 12 (38.7%) based on volume compared to BSA.
Over a 2-year follow-up, sirolimus was effective in treating patients with complicated vascular anomalies, when administered with cautious consideration of side effects. A multidisciplinary approach is needed for evaluating treatment outcomes in these patients, necessitating further long-term research on adverse effects.
Vascular anomalies include various diseases, which are classified to vascular tumors and malformations, according to the International Society for the Study of Vascular Anomalies (ISSVA) classification [1]. The first version of the ISSVA classification was adopted in 1996, and has been revised several times since, and new diseases/conditions and subtypes have since been included in subsequent revisions, and a numerous causative genes have been identified. The characteristics of vascular anomalies that grow and/or expand can lead to a variety of clinical symptoms depending on their location. These symptoms range from chronic pain to disfigurement and can even affect vital organs such as the trachea, resulting in dyspnea. Conventional therapeutic options such as surgery or sclerotherapy are often inadequate for addressing complicated vascular anomalies, which are defined as diffuse lesions that cannot be removed by simple resection surgery or lesions encasing vital organs such as the trachea or major blood vessels [2].
Under such circumstances, there has been several studies conducted to figure ideal therapies for this diverse patients, targeting cellular pathways crucial in abnormal vascular proliferation and growth.
The phosphatidylinositol 3-kinase (PI3K)/AKT signaling pathway plays a major role in cell growth and survival and has been shown to govern normal vascular development and angiogenesis [3]. Mutation in this pathway can lead to overactivation, causing dysregulation of cellular function and resulting in various tumorous conditions, including vascular anomalies. In efforts to treat vascular anomalies, several drugs targeting the PI3K pathway have been explored. Among them, mammalian target of rapamycin (mTOR) inhibitors have emerged as a commonly used drug in transplant patients, with established safety in pediatric populations. By reducing cell proliferation, angiogenesis, and vascular endothelial growth factor (VEGF) expression, mTOR inhibitors have been applied to patients with vascular anomalies, offering a promising therapeutic approach.
In this study, we aimed to present the clinical experience of sirolimus treatment in a single center over a period of 2 years, focusing on efficacy and safety.
A retrospective review was performed on patients of complicated vascular anomalies treated with sirolimus between January 2018 and December 2021 at Asan Medical Center. Sirolimus was administered to a patient population encompassing all age groups, including pediatric patients (aged 19 years and under), with vascular anomalies deemed unresectable due to involvement of vital organs or extensive effects shown on imaging or histopathology, and those whose symptoms did not improve or worsened following treatment based on the type of vascular anomaly. Patients with localized vascular anomaly, those showing improvement with conventional treatment, those with resectable lesions and those with less than 2 years of follow-up observation were excluded from the study population. The Institutional Review Board of Asan Medical Center approved this study (IRB No. 2020-0190).
Sirolimus was administered orally at a loading dose of 1.6 mg/m2 per dose once followed by 0.8 mg/m2 per dose, twice daily at 12-hour intervals. Using pharmacokinetically-guided dosing, sirolimus levels were measured at appropriate times, and trough levels were maintained between 8 and 12 ng/mL. Dose reductions or interruptions were implemented for clinically significant toxicities.
Patients have been assessed during regular outpatient follow-up. For the outcome measure, they have taken radiologic tests such as magnetic resonance imaging (MRI) were conducted every years and the adverse events were assessed according to the Common Terminology Criteria for Adverse Events. Laboratory testing to assess safety included hematologic, serum metabolic tests.
There is no optimal measurement of disease response in patients with complicated vascular anomaly, because of its various characteristics. In this study, treatment efficacy was measured by volume change before and after 2 years of sirolimus treatment, measured by volumetry in MRI. We used in-house computer aided volumetry software obtained from patient’s MRI. Despite a reduction in the size of the lesion clinically or as perceived by the caregiver, there are instances where the absolute size of the lesion measured on MRI appears to increase as patients grow. Therefore, we measured volumetry on MRI divided by the patient’s body surface area (BSA) to assess relative size changes. Also, we reviewed all patients’ MRI scans in collaboration with 2 pediatric radiologists, reassessing the patients’ diagnoses according to the ISSVA classification.
In total, 32 patients had sirolimus treatment over 2 years between January 2018 and December 2021 at Asan Medical Center. Patient and tumor characteristics are summarized in Tables 1 and 2. There is one patient, classified as having “none” symptoms, who had microcystic venolymphatic malformation in the mesentery which causing no discomfort for the patient. When divided by age at the initiation of medication, there were 5 patients aged less than a-year-old, 18 patients aged less than 10-year-old, 8 in their teens and 1 aged 20 or older. Median start age of sirolimus was 65 (29–124) months and median period of usage was 38 (32–44) months. We tried to maintain trough level of sirolimus between 8 and 12 ng/mL, but the median therapeutic drug monitoring (TDM) level was 6.95 (5.98–7.73) ng/mL. In cases where patients exhibited infection symptoms or severe side effects such as stomatitis, sirolimus was temporarily discontinued, during which time some of the TDM was measured. Since these inaccurate TDM values were included, the median value is lower than the target range we aimed for.
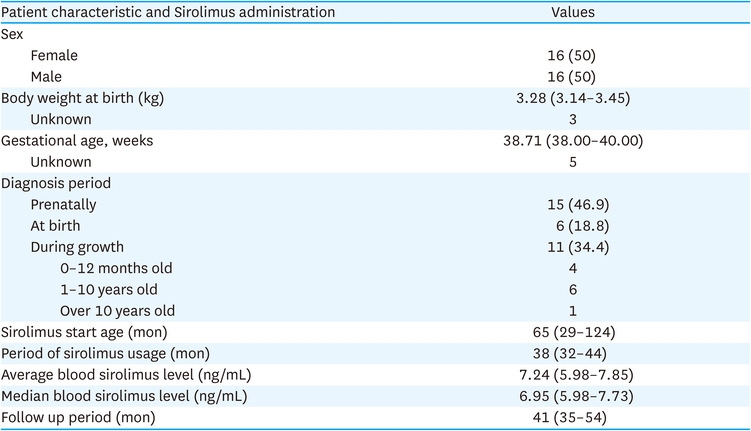
Table 1
Patient characteristics and Sirolimus administration (n=32)
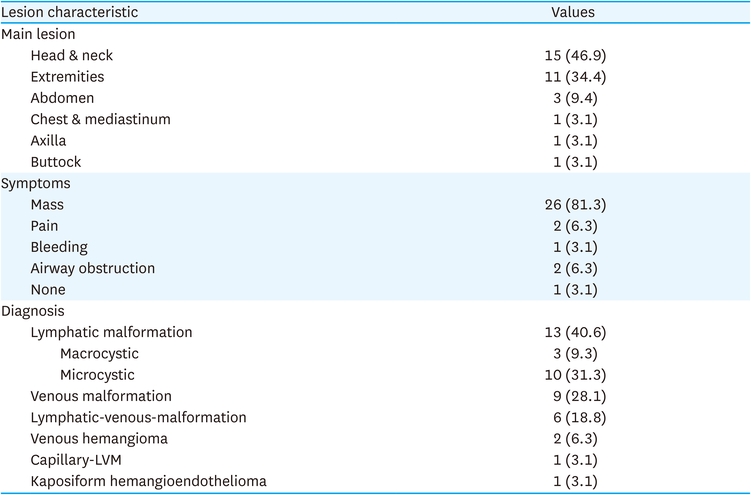
Table 2
Lesion characteristic (n=32)
Sirolimus was initiated median 47 months after diagnosis. Among them, only 3 patients began sirolimus immediately after diagnosis without prior therapy, with the shortest interval between diagnosis and sirolimus initiation being 2.6 months. The longest gap between diagnosis and initiation of sirolimus therapy was 312 months. Among the patients who received prior therapy, the distribution is as follows; 5 patients were treated with beta blockers, 2 underwent surgery, and 8 received interventions such as sclerotherapy. Furthermore, 2 patients underwent both beta blocker and sclerotherapy, 11 underwent surgery and sclerotherapy, and 1 patient underwent all of three treatments; beta blocker, surgery, and sclerotherapy.
Among 32 patients, 24 patients are currently under medication, 4 discontinued treatments due to significant improvement in lesions as per clinical judgement, while 4 were lost to follow-up. One patient who initiated sirolimus therapy was excluded from relative tumor volume measurement due to absence of BSA data.
Two patients stopped and resumed sirolimus treatment during the study period. One patient discontinued medication due to lesion improvement; however, after about 5 months of discontinuation, he experienced lesion aggravation prompting a decision to resume sirolimus. Following re-application, the lesion was improved. The other patient had voluntarily stopped medication due to parental concerns about upper respiratory tract infection related to her tracheostomy status. During the sirolimus treatment, lesion improvement was observed; however, approximately 14 months after discontinuation of sirolimus, the patient presented to the outpatient clinic with a new lesion observed beneath the left jaw. Subsequently, medication treatment was resumed, and currently, the lesion shows improvement with ongoing medication administration.
Absolute reduction in lesion size on MRI was observed in 17 patients (53.1%), lesion stability in 7 (21.9%), and lesion increase in 8 (25%). Relative reduction in lesion size based on BSA was noted in 22 patients (71%), lesion stability in 7 (22.6%), and lesion increase in 2 (6.5%). Patients classified as ‘markedly decreased’ numbered 9 (28.1%) when categorized by absolute volume and 12 (38.7%) based on volume relative to BSA. Efficacy presented according to tumor characteristics and previous treatment is described in Table 3.
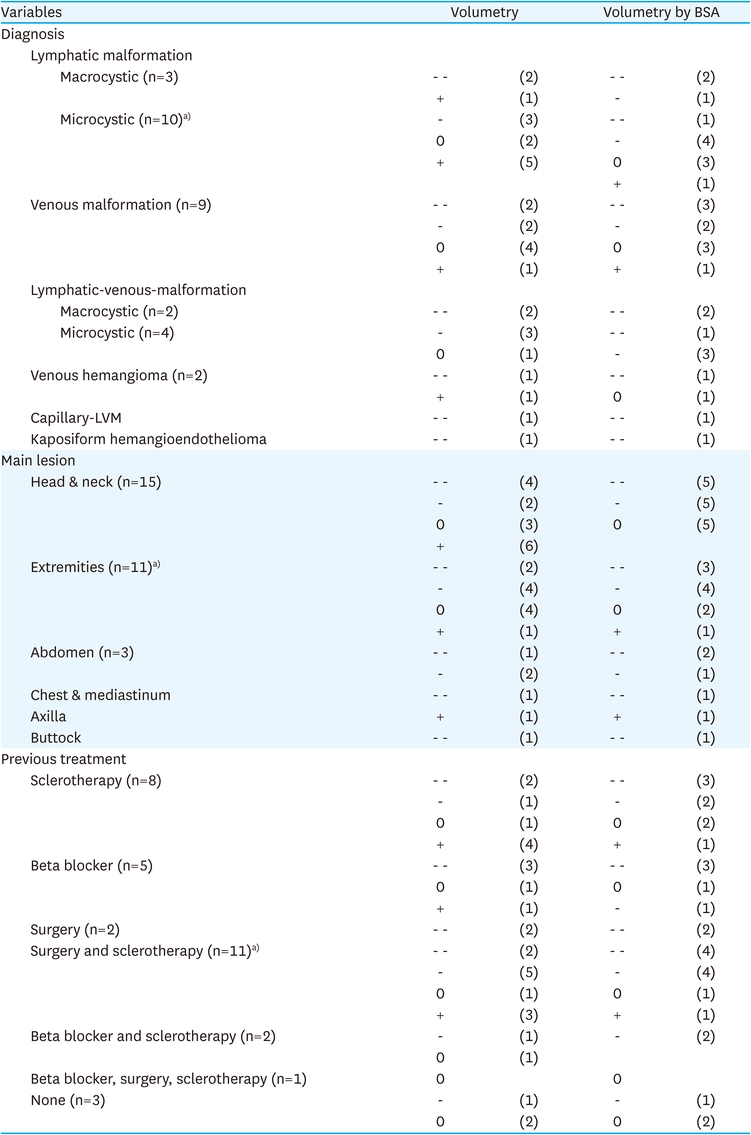
Table 3
Efficacy presented according to tumor characteristics and previous treatment
None of the patients experienced adverse events of Common Terminology Criteria for Adverse Events (CTCAE) grade 3 or higher; however, in some patients, medication was temporarily discontinued or maintained at lower doses due to adverse effects. Sirolimus intake was suspended in cases presenting signs of infection, including fever, with resumption of intake one week after symptom resolution. A total of 19 patients discontinued medication at least once, with an average discontinuation period of 64.5 days. Adverse drug reactions included stomatitis in 6 patients (18.8%), diarrhea in 2 patients (6.3%), and skin rash, abnormal liver function tests, elevated serum triglycerides, and hyperglycemia each in 1 patient (3.1%).
Sirolimus functions as a specific inhibitor of the mTOR, an enzyme crucial for controlling processes like angiogenesis, cellular growth, and proliferation. Sirolimus was approved by Food and Drug Administration (FDA) in 1999 for oral administration as an immunosuppressive agent in kidney transplantation. And in 2015, the FDA approved it as first drug to treat lymphangioleiomyomatosis, a rare, progressive lung disease that primarily affects women of childbearing age. The potential of sirolimus to treat vascular malformations is supported by its ability to decrease VEGF, which is a known key regulator in lymphangiogenesis and angiogenesis [4]. Blatt et al. [5], the first report on the successful use of sirolimus as an antiangiogenetic agent was published in 2010. In this study, they reported the effective response to sirolimus treatment in a patient with Kaposiform hemangioendothelioma who was unresponsive to conventional therapy. This patient had complicated vascular anomaly, encasing the airway, at the time of initial diagnosis. Despite undergoing treatment with beta blockers and steroids for 6 months, the patient showed resistance to treatment, with an increase in mass size and worsening respiratory symptoms. However, after the initiation of sirolimus therapy, as confirmed by a follow-up MRI at 10 months, there was a reduction in mass size and improvement in the patient’s symptoms. Subsequently, a large-scale patient study by Adams et al. [2] reported that sirolimus was effective in 83% and 85% of patients after 6 and 12 months of treatment, respectively.
Although numerous articles reported the efficacy of sirolimus in treating vascular anomalies, comparing treatment effectiveness is limited due to the heterogeneous nature of these anomalies and the absence of a standardized measurement. While some studies have reported the percentage of volume reduction [6, 7, 8, 9], due to the concurrent growth of pediatric patients and their vascular anomaly lesions, we aimed to assess proportional volume by dividing the volume by patients’ BSA.
In this study, 53.1% of patients exhibited a decrease in volume on MRI as measured by volumetry, and 71% of patients showed volume decrease when assessed using relative volumetry divided by BSA. Notably, 28.1% of patients had markedly decreased volume reduction based on absolute volume, and 38.7% based on volume compared to BSA.
In many trials, the volume reduction was not quantified to compare with our result. In some studies, the percentage of volume reduction was reported, and the reductions were between 49 and 90% in lymphatic malformation in neck [4]. Adams et al. [2] analyzed the efficacy by quality of life, functional impairment score, and radiologic evaluation. It reported that after 12 course of treatment, 52% of patients showed volume reduction over 20% in radiologic evaluation, which correlated with our result.
To our knowledge, this study represents the first analysis of therapeutic effects of sirolimus by evaluating the volume of lesions compared to patients’ growth. Interestingly, there were often discrepancies between the perceived improvement of lesions by patients or caregivers and the radiological interpretations. We believe that relative volume analysis is appropriate in assessing treatment outcome of sirolimus.
The safety of long-term use of sirolimus in organ transplant recipients has been demonstrated. And most side effects are dose dependent [10]. However, since FDA approved sirolimus in pediatric kidney transplantation in patients aged 13 years and older, its potential side effects remain unclear particularly in newborns and younger patients.
Adams et al., a multicenter study with 61 patients, from newborns to 31 years of age, reported drug-induced adverse effect over grade 3 included blood/bone marrow (27%), metabolic/laboratory (3%), infection (2%), lymphatic (2%), and pulmonary/upper respiratory (2%). And there was no toxicity-related death [2].
Wiegand et al., analyzed 28 studies including 105 patients with lymphatic malformations of the head and neck, and it reported that various adverse effects like hyperlipidemia, neutropenia, and infections. And in 5 studies included in this study reported no patients experienced side effects [4].
In another review article, Freixo et al., including 73 articles with 373 patients of vascular anomaly, demonstrated that the side effects most frequently reported were oral mucositis (31.9%), dyslipidemia (16.5%), leukopenia (12.3%), gastrointestinal symptoms (10.2%), and rash/eczema (8.2%) [11].
In this study, we experienced no patients with adverse effects over CTCAE grade 3. The observed difference could possibly be due to maintaining drug concentration level lower than those in Adams et al. [2]. And most frequently reported adverse event was stomatitis (18.8%), which correlates with Freixo et al. [11].
One of the severe side effect is Pneumocystis jirovecii pneumonia, which was reported in two patients with vascular anomalies treated with sirolimus [12, 13], and some studies recommended prophylaxis with sulfamethoxazole-trimethoprime [10, 14]. We did not encounter any case of Pneumocystis infection, even all of the patients did not systematically receive Pneumocystis prophylaxis. But special caution is warranted, in patients who develop neutropenia, in very young children, or with underlying diseased causing lung dysfunction, a poor general condition, or other co-morbidities.
This study has several limitations. All patients underwent a modified quality of life survey developed by the institution prior to the initiation of sirolimus. However, due to incomplete follow-up surveys in all patients, the insufficient data precluded its inclusion in this paper. Attempts were made to correlate outpatient records with radiologic imaging; however, the retrospective nature of the study limited the assessment of symptomatology or lesion improvement from outpatient records alone.
Furthermore, in some patients with the lesion size reduced resulting in skin laxity, clinicians perceived improvement, yet radiologic interpretation did not consistently align with these size change. Consequently, current practice involves not only relying on imaging studies but also considering patient satisfaction to determine the continuation and tapering of sirolimus.
The duration of sirolimus treatment is still controversy and different between the studies. Also, the time to reach the optimum treatment effect remains unclear. In the review article, Wiegand et al. [4], analyzed the time to clinical response between 10 days and 13 months. It was also our concern that how long to continue medication and how to manage discontinuation. In one patient, we experienced the lesion progression 5 months after sirolimus discontinuation, so resuming medication was necessary. Currently, we are implementing tapering methods such as reducing the dosage from twice daily to once daily. Additionally, we are considering long-term administration at low doses. Also, we are planning further studies to investigate the potential long-term toxicity and assess the risk of relapse following discontinuation.
In our study, there was 2 patients experienced an increase in lesion size relative to BSA. One patient is diagnosed as microcystic lymphatic malformation, and initiated sirolimus treatment at the age of 10. This patient presented with diffuse lesions spreading across the axilla and trunk. After undergoing 6 sessions of sclerotherapy and 4 excision surgeries, sirolimus treatment was commenced and continued for 46 months, with ongoing treatment. The other patient is diagnosed with slow-flow venous malformation, with infiltrative lesions affecting the left leg, abdominal wall, and even in the iliac bone. Sirolimus treatment was applied at the age of 13 after 2 sessions of sclerotherapy and has been ongoing for 46 months. Both patients had average sirolimus level of 7.0 and 7.2, respectively, with cessation periods of 7 days and 5 days each. Biopsy of the lesion and evaluation of molecular pathway mutations are planned for these patients.
The sample size in this study was insufficient for phenotype/genotype correlation. However, such correlation may be feasible in future studies and may guide treatment decisions, especially with the introduction of novel drugs for molecularly targeted therapy.
In conclusion, based on treatment and follow-up results of over 2 years, sirolimus appears to be effective and safe for most vascular anomaly patients when appropriately dosed according to individual patient circumstances. A multidisciplinary approach is necessary for the evaluation of vascular anomaly patients’ treatment, and further research is needed for long-term drug efficacy and adverse effect monitoring. Additionally, in patients who exhibit resistant to treatment, further research on phenotype/genotype correlation through tissue examination and molecular targeted therapy is warranted.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.Y.
Data curation: P.J., H.S., Y.H.M., K.P.H.
Formal analysis: P.J.
Supervision: K.D.Y.
Visualization: P.J., K.D.Y.
Writing - original draft: P.J.
Writing - review & editing: K.H., N.J.M., K.D.Y.
