
 , Ju Yeon Lee2
, Ju Yeon Lee2

Duodenal web (DW) is a rare congenital anomaly of the intestinal tract that can lead to severe dehydration and electrolyte imbalance. A 14-day-old boy presented with recurrent vomiting and weight loss and was diagnosed with DW. Duodenoscopy identified a pinhole structure in the second portion of the duodenum, prompting a subsequent endoscopic balloon dilatation procedure. Following the procedure, vomiting and abdominal distension resolved, and the patient was discharged on a regular diet. No symptoms recurred during follow-up.
Duodenal web (DW) is a rare congenital anomaly of the intestinal tract that can lead to severe dehydration and electrolyte imbalance. A 14-day-old boy presented with recurrent vomiting and weight loss and was diagnosed with DW. Duodenoscopy identified a pinhole structure in the second portion of the duodenum, prompting a subsequent endoscopic balloon dilatation procedure. Following the procedure, vomiting and abdominal distension resolved, and the patient was discharged on a regular diet. No symptoms recurred during follow-up.
Duodenal web (DW), also referred to as duodenal membrane/diaphragm or intraluminal duodenal diverticulum, is a rare congenital anomaly in which a membrane-like structure, partially or completely, obstructs the duodenum. Although duodenal obstruction is a common congenital gastrointestinal anomaly in newborns, it accounts for approximately 10% of all congenital duodenal obstructions [1]. Children with DW commonly present with symptoms such as vomiting, dehydration, or failure to thrive. However, disease severity depends on the degree of fenestration, which can contribute to a delayed diagnosis.
The primary treatment for DW is surgical intervention; however, reports on endoscopic procedures have accumulated since the 1990s. In Korea, Lee et al. reported an endoscopic DW resection using an insulated knife in a 3-year-old child with Down syndrome in 2011 [2]. However, further reports in this field are scarce, especially in young children. Here, we present the first case of endoscopic ballooning in a neonate with DW in Korea.
A 14-day-old male child with a history of frequent non-bilious vomiting since birth visited the emergency department. Vomiting persisted despite supportive treatments, such as positional changes and formula adjustments. The infant showed abdominal distension and had lost 5% of his birth weight. Physical examination revealed decreased skin turgor, and the patient produced only two wet diapers daily. Abdominal radiography revealed a distended stomach with some small bowel gas, while ultrasonography revealed duodenal dilatation. The upper gastrointestinal series revealed a windsock sign and a distended contrast-filled duodenum surrounded by a narrow lucent line with a small connection to the distal intestine (Fig. 1). No abnormalities were observed.
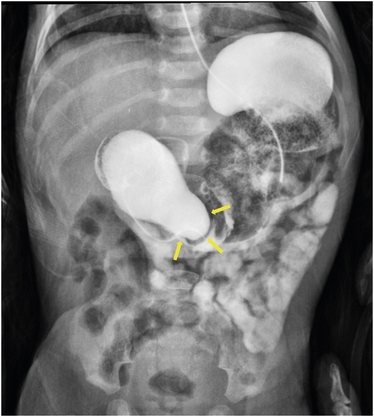
Fig. 1
An upper gastrointestinal series reveals a contrast-filled sac (arrow) with a surrounding rim of lucency. This configuration is referred to as the windsock sign, a typical imaging finding associated with a duodenal web.
The patient was referred to the Department of Pediatric Surgery. After consultation with a pediatric gastroenterologist, endoscopic intervention was attempted as the initial approach. The pediatric surgeon was on standby for emergent complications. Endoscopy was performed with the patient under general anesthesia using a flexible endoscope. A dilated duodenum and membranous stenosis with small openings were also observed (Fig. 2A). A guidewire was carefully introduced into the opening (Fig. 2B), followed by a multi-diameter dilation balloon (CRE™ PRO wire-guided balloon dilatation catheter, Boston Scientific, Product Code M00558640). The balloon was incrementally expanded from 10 to 18 mm, with each inflation lasting 1 minute (Fig. 2C). A mucosal tear was confirmed after repeated expansions with no evidence of perforation or bleeding. The ampulla of Vater was found immediately below the web, and no additional strictures were observed in the distal intestine (Fig. 2D).
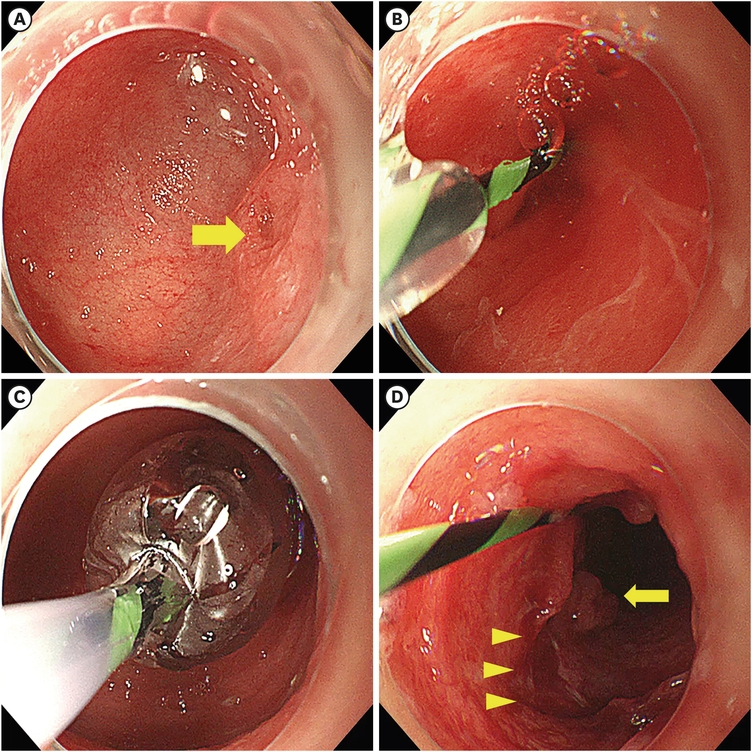
Fig. 2
Balloon dilatation of the duodenal web. (A) Endoscopy reveals a dilated duodenal bulb with a tiny lumen (arrow). (B, C) A guiding catheter is passed through the opening, and balloon dilatation is performed, increasing from 10 mm to 18 mm. The diameter of inflation did not exceed the caliber of the duodenum. (D) Stenosis markedly improves after ballooning. A post-dilatation mucosal tear (arrowhead) and the ampulla of Vater (arrow) are observed.
Abdominal bloating and vomiting resolved immediately after the procedure, and a regular diet was initiated the day after the intervention. Subsequent upper gastrointestinal imaging revealed no signs of intestinal obstruction or passage disturbance (Fig. 3). During the 3-month follow-up period, the patient exhibited no recurrence of symptoms and displayed normal growth.
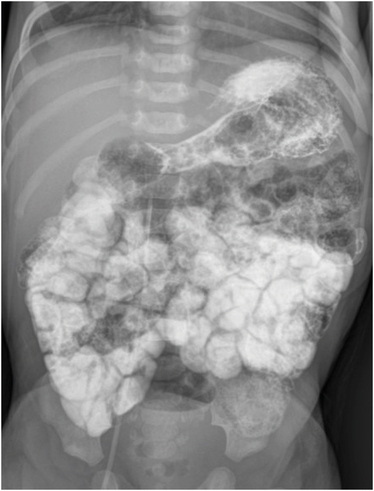
Fig. 3
Following upper gastrointestinal series no longer reveals a dilated duodenum and passage disturbance.
DW occurs in 1:10,000–1:40,000 live births and results from incomplete recanalization of duodenal epithelial cells during gestation. The lesion is typically located in the second part of the duodenum near the ampulla in 85%–90% of cases, followed by the third and fourth portions of the duodenum. DW may also be associated with Down syndrome or malformations in other organs, including the heart, gastrointestinal tract, spine, and kidneys. No other associated diseases were identified in this patient [3].
Traditionally, surgery, including gastrojejunostomy, duodenojejunostomy, and duodenotomy with web excision, has been considered the primary treatment for DW. Among them, established primary surgical methods for DW were longitudinal anterolateral duodenotomy, web resection, and transverse closure of the duodenotomy [4].
Laparoscopic surgery has been successfully performed in children with duodenal obstructions. Muensterer and Hansen [5] also reported a case of a 9-month-old girl with DW who underwent single-incision endoscopic surgery with good functional and cosmetic results. Although the laparoscopic approach is safe and effective, it does not decrease the time to full feeding or the length of stay [6]. The overall morbidity and length of hospital stay were approximately 22% and 14 days, respectively [7]. Concomitant Down syndrome or congenital heart defects may increase the mortality risk [8].
With the growing interest in nonsurgical treatments, the number of trials of endoscopic interventions for various gastrointestinal diseases has been increasing. There have been case reports of endoscopic interventions for DW, and various endoscopic intervention methods have been explored, including simple balloon dilatation, endoscopic knife incision, and balloon traction. Although specific indications for endoscopic intervention are still under development, this minimally invasive approach is safe and effective in neonates or those with underlying medical conditions such as Down syndrome. Sundin et al. reported successful endoscopic dilatation in a 6-month-old female patient with a double DW without surgery or the need for repeat endoscopy [9, 10, 11, 12].
The first endoscopic intervention for a 35-month-old girl with DW in Korea was endoscopic resection using an insulated tip knife in 2011 [2]. However, endoscopic resection is associated with a higher risk of perforation, bleeding, and potential damage to the ampulla of Vater, leading to preference for the ballooning method. Endoscopic ballooning involves tearing the membranous web without affecting the submucosa or muscle layer, thereby significantly reducing the perforation risk. Furthermore, ballooning equipment and procedures are much simpler than resection methods. Therefore, we recommend endoscopic balloon dilation as a minimally invasive treatment option after a thorough discussion with patients who want a non-surgical approach.
Poddar et al. [11] performed multiple balloon expansions over several weeks, starting with smaller balloons. However, while carefully observing the complications, we progressed from smaller to larger balloons during a single procedure. If bleeding or perforation does not occur during intervention, increasing the maximum diameter in a single session may be worth considering.
In conclusion, this is the first report of the endoscopic treatment of DW in a neonate in Korea. Endoscopic balloon dilation is a simple and efficacious procedure, and physicians managing children with DW should consider the endoscopic method as a valuable treatment option.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: L.J.Y.
Data curation: K.S.H.
Writing - original draft: K.S.H., L.J.Y.
Writing - review & editing: K.S.H., L.J.Y.
