
 , Shailesh Solanki
, Shivani Dogra
, Jai K Mahajan
, Shailesh Solanki
, Shivani Dogra
, Jai K Mahajan

Morgagni hernia (MH) is a type of congenital diaphragmatic hernia that is rare and without any distinctive presentation. Chest radiographs can miss the diagnosis when solid organs instead of bowel loops are herniated. Echocardiography can perplex the diagnosis instead of aiding if MH is not suspected. We are here discussing the presentation and management of a neonate with MH, which was referred to our institute as a congenital heart disease.
Morgagni hernia (MH) is a type of congenital diaphragmatic hernia that is rare and without any distinctive presentation. Chest radiographs can miss the diagnosis when solid organs instead of bowel loops are herniated. Echocardiography can perplex the diagnosis instead of aiding if MH is not suspected. We are here discussing the presentation and management of a neonate with MH, which was referred to our institute as a congenital heart disease.
Congenital diaphragmatic hernia (CDH) occurs due to abnormal diaphragmatic development during the embryonic period, leading to herniation of abdominal contents into the chest. Morgagni hernia (MH) is a rare type, encompassing around 1%–5% cases of CDH; it involves the protrusion of abdominal contents into the thoracic cavity through a diaphragmatic defect situated behind the sternum, known as the foramen of Morgagni [1]. The diaphragmatic defect is typically found on the right side (90%) or bilaterally (7%) [2]. The presence of the heart and the pericardium is a barrier against herniation; in most instances, patients do not exhibit symptoms until adulthood. However, there are rare cases where the condition becomes evident during the neonatal period, leading to significant respiratory distress. In these scenarios, there might also be concurrent anomalies in other organs, including the heart [2]. Plain radiographs can show herniating bowel loops into the thoracic cavity and assist in the diagnosis. There may be a dilemma in diagnosis, especially with herniation of solid organs like the liver, which is not easily detectable on chest radiographs. Diagnosing these conditions can be challenging and may resemble other medical conditions, as exemplified in the primary case. Due to the similarity of symptoms with congenital heart diseases (CHDs), diagnosis may remain obscure, and another diagnostic tool like computerized tomography (CT) scan may help for a diagnosis.
The five-week-old male child was referred to our institute for CHD with respiratory distress for one week. The child was preterm and born by cesarian section because of placenta previa and, had a smooth perinatal period, and had no complaints till four weeks of age. He suddenly developed respiratory distress and attended a local hospital where the child was intubated and kept on a ventilator. On further investigations, the X-ray chest showed an enlarged heart shadow, and echocardiography (2D echo) was reported as a hypoplastic right ventricle inlet. Afterward, he was referred to our institute for further management. After primary resuscitation, a chest radiograph was done, which depicted a slightly enlarged heart shadow and clear lung fields (Fig. 1A). A 2D echo was done, suggesting an external mass compressing on the right ventricle and possibly causing inflow tract obstruction. No other structural anomaly was detected; the right ventricular outflow tract and pulmonary pressures were normal. A CT scan was done to delineate the anatomy more clearly, which showed herniated liver tissue anterior to the pericardium and compressing it, suggesting MH (Fig. 1B).
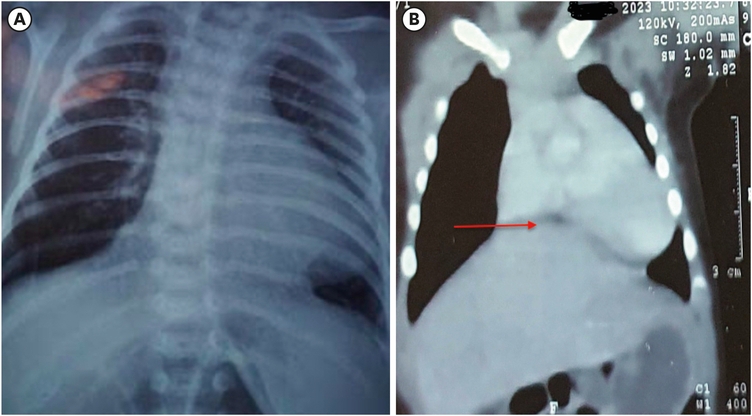
Fig. 1
Radiological investigations. (A) An X-ray of the chest showing a slightly enlarged heart shadow and mediastinal shift to the left side. (B) Computerized tomography reconstructed coronal image showing herniation of the liver (red arrow) into the thoracic cavity and compression on the pericardium.
The child was shifted to the surgical neonatal intensive care unit, and after resuscitation, he was taken for surgery. On exploration via substernal midline transverse incision, the hernial sac (size 3 × 3 cm) was found just posterior and right side to the sternum, part of the left lobe of the liver was seen herniating through the sac, and it was compressing upon the pericardium (Fig. 2A). Hernial content was reduced, and the sac was excised. The pericardium was visible through the sac. The anterior and posterior lip of the diaphragm were delineated and repaired using silk 2-0 suture (Fig. 2B).
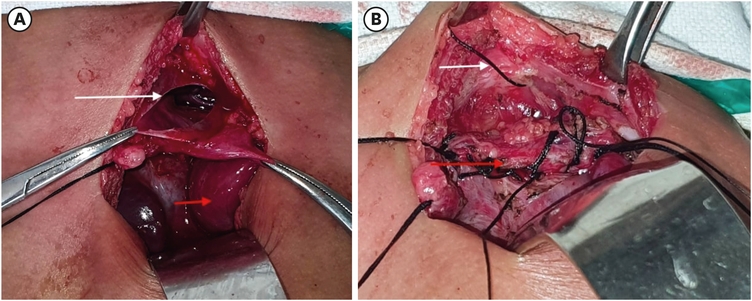
Fig. 2
Intraoperative image. (A) An opened hernial sac (white arrow) and reduced liver content (red arrow). (B) Complete closure (red arrow) and relation with sternum (white arrow).
The child had a smooth postoperative recovery and could be successfully extubated two days after the surgery. Repeat 2D echo showed no right ventricular inflow obstruction. The patient was discharged after seven days of surgery and was doing well at 6-month follow-up.
Written and informed consent was obtained from parents to publish the report and associated images with assurance to keep their identity confidential.
MH is an infrequent anterior opening in the diaphragm, initially documented by Morgagni in 1761, often remains without symptoms and is typically discovered incidentally during investigations for other conditions [2]. When symptoms arise, they primarily result from the compression of thoracic organs. Furthermore, individuals with previously undetected MH have presented with recurrent chest infections and gastrointestinal issues like vomiting, abdominal pain, retrosternal/epigastric pain, bleeding, or symptoms of intestinal obstruction [3].
An MH is thought to arise from the inadequate fusion or abnormal muscular development of the pars sternalis and pars costalis during the diaphragm formation. This creates a triangular gap adjacent to the sternum, known as the Morgagni gap on the right and the Larrey gap on the left [4].
MH is commonly associated with other congenital malformations, including CHD. Deng et al. [5] described a case of MH associated with Cor-triatriatum; an 18-month-old child was diagnosed with CHD and incidentally detected to have MH during the investigation. They managed the child with MH repair followed by intra-cardiac repair [5]. Similarly, Khaleel [6] reported a case of a large atrial septal defect in a child, delaying the diagnosis of MH, which was eventually detected in a CT scan.
Herniating liver tissue, as in the index case, compresses the heart, leading to a diagnosis of inflow obstruction of the right ventricle on 2D echo. There was a suspicion that some lesion was compressing the heart from outside, and so a CT scan was done to delineate the anatomy clearly. The herniated liver was applying external pressure to the right ventricle from the anterior aspect closely resembled the echocardiographic observations, indicating the possibility of right ventricular hypoplasia, an uncommon yet severe CHD. Termed 'hypoplastic right heart syndrome,' signifies an incomplete development of the components on the right side of the heart, leading to insufficient blood circulation to the lungs and consequent cyanosis. Typically, atresia of the pulmonary valve and a hypoplastic pulmonary artery are concurrent features in this condition, which were absent in the index case.
Only one case of MH masquerading as CHD has been described by Bassareo et al. [2]; a newborn presented with cyanosis and respiratory distress was being managed as CHD. They detected herniating bowel loops in the chest radiograph and arrived at the diagnosis of MH [2]. Our case had a similar presentation and recovery after surgery, but a chest X-ray was not helpful because of a herniating solid organ instead of a bowel. Aké et al. [7] reported a case of an antenatally detected pericardial tumor, which turned out to be a case of an MH with protrusion of hepatic tissue into the pericardium. Symptoms of MH during neonatal presentation may mimic CHD, especially in cases with solid organ herniation, as characteristic findings of hernia in chest radiographs may be missing. 2D echo may help to diagnose associated heart anomalies. On the contrary, when heart defects are detected on 2D echo, associated MH may sometimes be overlooked, making diagnosis difficult. In the case of herniation of the liver as content, an X-ray may not aid in arriving at a diagnosis as was in our case; a CT scan in such a scenario proves to be beneficial.
In conclusion, MH is a rare diagnosis; furthermore, herniation of solid organs (like the liver) only without the bowel makes the presentation more complicated. This case report highlights the varied presentation of diaphragmatic hernia and the difficulties faced in diagnosing. A high degree of suspicion at the earliest gives an excellent outcome, and additional studies like CT scans and 2D-Echo may aid in the diagnosis.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: S.S., U.S.
Formal analysis: S.S., M.J.K.
Supervision: M.J.K., D.S.
Validation: S.S., M.J.K.
Writing - original draft: U.S., S.S.
Writing - review & editing: D.S., M.J.K.
