
Division of Pediatric Surgery, Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Copyright © 2016 Korean Association of Pediatric Surgeons
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

| Patient No. | Age at diagnosis (mo) | Age at operation (mo) | Chief complaint | Diagnostic modality | Treatment | Recurrence |
|---|---|---|---|---|---|---|
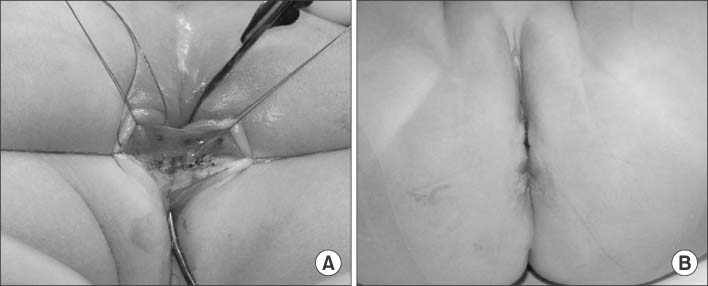
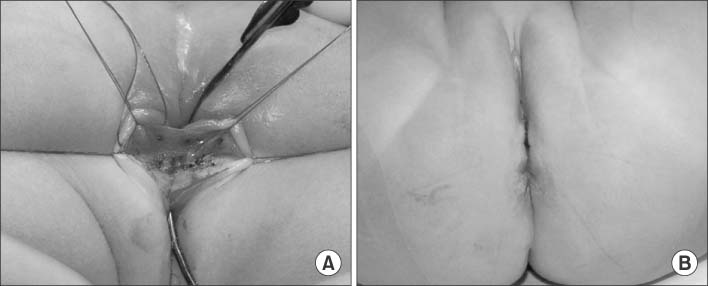
| 1 | 2 | 6 | Vestibular defecation | Gross physical examination | Fistulectomy & repair of perineal body | No |
| 2 | 0 | 5 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 3 | 2 | 6 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 4 | 1 | 1 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 5 | 3 | 3 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 6 | 0 | 7 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 7 | 0 | 2 | Vestibular defecation | Fistulography | Fistulectomy & repair of perineal body | No |
| 8 | 2 | 3 | Vestibular defecation | Gross physical examination | Fistulectomy & repair of perineal body | No |
| 9 | 1 | 2 | Major labial abscess | Fistulography | Fistulectomy & repair of perineal body | Yes |
| 10 | 1 | 2 | Vestibular defecation & major labial abscess | Fistulography | Fistulectomy & repair of perineal body | Yes |
| 11 | 2 | 5 | Vestibular defecation & major labial abscess | Gross physical examination | Abscess drainage → fistulectomy & repair of perineal body | No |

