

Intraductal papillary mucinous neoplasm (IPMN) of the pancreas encompasses a wide spectrum of epithelial changes from benign adenoma to invasive adenocarcinoma. IPMN is a premalignant lesion where approximately one-third of the tumors undergo malignant transformation. This disease is prevalent in the elderly population and is rare in youth. In this case we report a 12-year-old boy with symptoms of pancreatitis with cystic lesions consistent with branch duct type-IPMN. This is the third reported case of IPMN in a pediatric patient. Our patient underwent pylorus-preserving pancreaticoduodenectomy, and through this case report we suggest when worrisome features or high-risk stigmata features are observed even in pediatric patients, surgical resection should be considered due to the potential for malignant transformation in the future.
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas encompasses a wide spectrum of epithelial changes from benign adenoma to invasive adenocarcinoma. IPMN is a premalignant lesion where approximately one-third of the tumors undergo malignant transformation. This disease is prevalent in the elderly population and is rare in youth. In this case we report a 12-year-old boy with symptoms of pancreatitis with cystic lesions consistent with branch duct type-IPMN. This is the third reported case of IPMN in a pediatric patient. Our patient underwent pylorus-preserving pancreaticoduodenectomy, and through this case report we suggest when worrisome features or high-risk stigmata features are observed even in pediatric patients, surgical resection should be considered due to the potential for malignant transformation in the future.
Intraductal papillary mucinous neoplasm (IPMN) of the pancreas encompasses a wide spectrum of epithelial changes from benign adenoma to invasive adenocarcinoma, mainly involving the sixth to seventh decade of life. IPMNs are further grouped into main duct type IPMNs (MD-IPMNs), branch duct type IPMNs (BD-IPMNs), and mixed-type IPMNs according to the extent of pancreatic duct involvement. Neoplasia that involves the main pancreatic duct is classified as an MD-IPMN, whereas the involvement of the side branches is classified as a BD-IPMN. A BD-IPMN that involves the main pancreatic duct is termed a mixed-type IPMN [1].
This is a case report of a 12-year-old boy with symptoms of pancreatitis with cystic lesions consistent with BD-IPMN. This is the third reported case of IPMN in a pediatric patient [2, 3] and is the second-youngest case. The youngest was a 3-day-old neonate with a germline SKIL gene mutation [3].
A 12-year-old boy was admitted to the emergency department with a 1-month history of abdominal pain, which was aggravated on the day of his initial visit. The colicky abdominal pain was localized to the right and left upper quadrants with symptoms aggravated by a high-fat diet. He also experienced other symptoms including nausea and vomiting, but without weight loss or jaundice. The patient was previously healthy except for a known thyroid cyst with normal thyroid function. Risk factors for pancreatitis, including a history of obstructive diseases such as a biliary stone or choledochal cyst, medications such as valproic acid and steroids, or systemic illnesses such as hemolytic uremic syndrome [4], were denied. However, acute pancreatitis was suspected according to the International Study Group of Pediatric Pancreatitis: In Search for a Cure criteria [5] after evaluation for abdominal pain and imaging studies.
The initial preoperative laboratory data revealed an elevated amylase of 153 U/L and a lipase level of 71 U/L. The liver function tests were otherwise normal except for an elevated alkaline phosphatase of 429 IU/L. Abdominal ultrasonography was performed, which showed a lobulated cystic mass in the pancreas (Fig. 1), and subsequent computerized tomography (CT) showed a mildly inflamed pancreas with a 1.2×0.9×1.3 cm-sized low-attenuating cystic lesion with a pleomorphic appearance at the pancreatic uncinate process (Fig. 2). A magnetic resonance imaging (MRI) scan performed later for cystic evaluation showed pancreatic ductal communication with the cystic lesion along with downstream ductal dilatation. Furthermore, mild dilatation of the main pancreatic duct was observed (Fig. 3). The cystic lesion revealed communication with the dorsal duct and congenital anomaly of the pancreatic duct, and pancreas divisum was suspected due to a lack of fusion of the ventral and dorsal ducts and the common bile duct, which joins with the dorsal duct. Therefore, given the suspicion of IPMN and symptoms of pancreatitis, the patient underwent a pylorus-preserving pancreaticoduodenectomy. The histopathology report revealed BD-IPMN with intermediate-grade dysplasia. The depth was limited to the pancreas without invasion of the surrounding adjacent organs. Pancreatic intraepithelial neoplasia was not applicable, and the mucinous glands were of the intestinal type (Fig. 4).
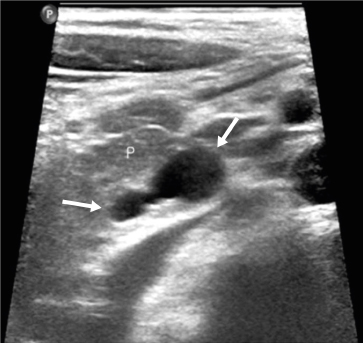
Fig. 1
Abdominal ultrasonography reveals a lobulated cystic mass (arrows) without discernable solid components.

Fig. 2
Abdominal computerized tomography reveals a small cystic mass (arrow) in the pancreatic uncinate process. The adjacent pancreatic duct (arrowhead) is mildly dilated.
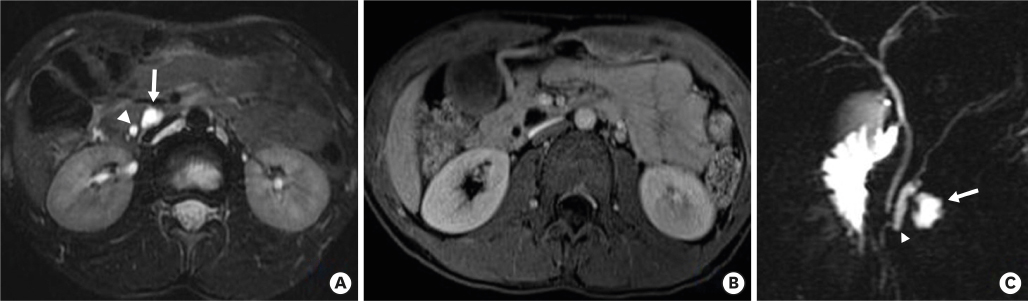
Fig. 3
(A) T2-weighted MRI reveals a small, lobulated cystic mass (arrow) in the pancreatic uncinate process. The adjacent pancreatic duct (arrowhead) is mildly dilated. (B) No solid enhancing components were revealed on T1-weighted MRI obtained after contrast administration. (C) Oblique-coronal, thick-slice magnetic resonance cholangiopancreatography reveals a lobulated cystic mass (arrow) and associated pancreatic duct dilatation (arrowhead).
MRI, magnetic resonance imaging.
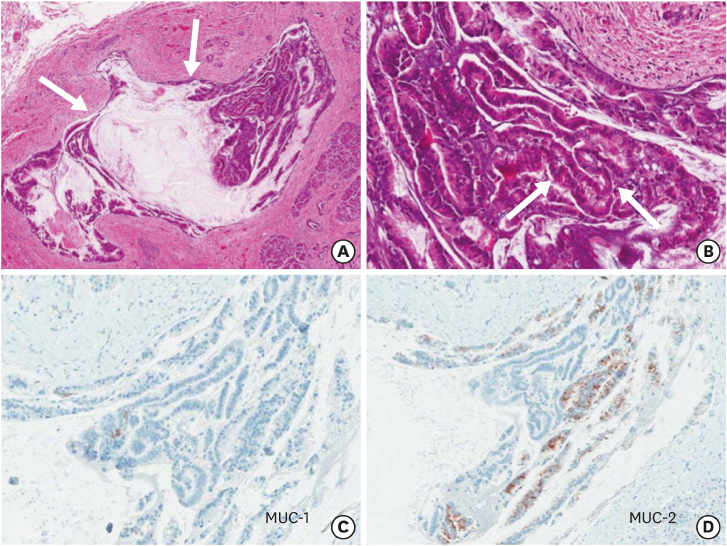
Fig. 4
(A) Low magnification of H&E staining of the IPMN shows a dilated duct with an intraductal epithelial papillary proliferation pattern and mucin production. (B) High magnification of H&E staining of the IPMN shows papillary structures lined by pseudostratified columnar epithelial cells with moderate dysplasia. (C) No immune labeling for MUC-1 in the IPMN was found. (D) IPMN showed intracytoplasmic immunoreactivity for MUC-2.
H&E, hematoxylin and eosin; IPMN, intraductal papillary mucinous neoplasm; MUC, mucin.
On postoperative day 5, the patient vomited several times with increased drainage through the nasogastric tube. A CT scan and upper gastrointestinal study (UGIS) were performed to evaluate the cause of the obstructive symptoms and signs. There was no passage of contrast through the duodenojejunostomy in the UGIS and luminal narrowing at the duodenojejunostomy site was suspected on the CT scan. Therefore, on postoperative day 12, a reoperation was performed. During the exploration, there was no definite obstructive lesion, but the afferent loop was severely dilated and compressed by the efferent loop, thereby obstructing the passage. The duodenojejunostomy was converted to a Roux-en-Y anastomosis, and after the reoperation, the patient made a good recovery with dietary progression and was discharged from the hospital. A follow-up MRI taken 9 months postoperatively revealed a 1.2 cm-sized cystic lesion at the dorsal aspect of the pancreaticojejunostomy. A pseudocyst secondary to recurrent pancreatitis and recurrent IPMN was suspected. However, because approaching a cystic lesion by endoscopic retrograde cholangiopancreatography is difficult, the lesion is being closely observed on an outpatient basis.
Since the first description of IPMN in 1982, the diagnosis and definition of IPMN have evolved dramatically over time, and the incidence of pancreatic cystic tumors has increased rapidly over the last two decades [6]. IPMN can be further categorized into MD-IPMN, BD-IPMN, and mixed-type IPMN according to the extent of pancreatic duct involvement [7]. IPMN is more prevalent during the sixth and seventh decade of life [8], but the incidence of pancreatic neoplasm in children is unknown due to the rare occurrence in this population. There are only a few institutional studies describing malignant pancreatic neoplasms [9, 10, 11]. Our patient was initially diagnosed at age 12 and is one of the youngest known patients with BD-IPMN. The patient's worrisome features are described.
IPMN is a premalignant lesion where approximately one-third of the tumors undergo malignant transformation [7], and its worrisome features and high-risk stigmata are used to identify high-risk patients diagnosed with IPMN [12]. The worrisome features include main duct sizes of 5–9 mm, enhancing mural nodules of <5 mm, thickened and enhancing cyst walls, BD-IPMN sizes >3 cm, abrupt caliber changes in the main duct with upstream atrophy, lymphadenopathy, increased serum CA19-9 levels, and cyst growth rates of >5 mm in 2 years. Also, the symptoms of pancreatitis are seen as worrisome features of IPMN [12]. The high-risk stigmata features include main duct sizes larger than 1 cm, enhancing mural nodules of >5 mm, and symptoms of obstructive jaundice [12].
Treatment plans vary according to the subtypes of IPMN. Surgical resection is recommended for MD-IPMN, especially those with main duct sizes >12 mm due to the high risk of malignant transformation [13]. However, treatment plans for BD-IPMN patients can vary according to risk stratifications in the international consensus guidelines [12]. Patients diagnosed with BD-IPMN exhibiting worrisome or high-risk stigmata features should be considered for surgical resection [14, 15] since the risk of malignancy in BD-IPMN with these features is 2%–3% [16]. Also, surgical resection should be considered for pediatric patients with long life expectancies as the long-term prognosis has not yet been reported. In our case, although close observation could have been applied, as the cystic lesion was small in size, we believe surgical resection was appropriate as the patient showed symptoms of pancreatitis, a known clinical worrisome feature of BD-IPMN, with other associated imaging findings such thickened cyst wall. After surgical resection, the final pathology report indicated BD-IPMN with intermediate-grade dysplasia, and such a degree of dysplasia is known for more malignant transformation than low-grade dysplasia [17]. Furthermore, there are 4 subtypes according to histopathology: gastric, intestinal, pancreatobiliary, and oncocytic. These 4 subtypes are known to affect the degree of dysplasia [18]. According to the current literature, most BD-IPMNs are of the gastric type, which has low proliferative activity and low malignant transformation potential. In contrast, the intestinal subtypes are prone to become invasive carcinomas. This histologic type tends to be larger and more complex [18, 19]. The patient described in this case report revealed the intestinal type in his final pathology report. Therefore, careful and close observation is warranted.
In conclusion, although a pediatric pancreatic cystic lesion is a rare presentation, IPMN should always be considered in pediatric patients with symptoms and laboratory data clinically associated with pancreatitis with cystic lesions on imaging studies. Also, when worrisome or high-risk stigmata features are observed, surgical resection should be considered due to the potential for malignant transformation. Furthermore, considering the long-life expectancy of pediatric patients, aggressive but careful treatment plans are needed.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.M.K., K.H.Y.
Data curation: K.M.K., Y.J.K.
Formal analysis: K.M.K., Y.J.K., K.H.Y.
Methodology: K.H.Y.
Supervision: K.H.Y.
Writing - original draft: K.M.K.
Writing - review & editing: K.M.K., Y.J.K., K.H.Y.
