

Purpose
Acute appendicitis is the most common surgical condition of abdomen in children and the diagnosis is still challenging. The aim of this study was to evaluate the diagnostic value of the Alvarado score and computed tomography (CT) scan and to provide guidance for CT scan to reduce the number of CT examinations for clinically suspected acute appendicitis in children.
Methods
We retrospectively analyzed pediatric patients aged below 18 years and screened via abdominal CT for suspected appendicitis at Yeungnam University Hospital between January 1, 2013 and October 31, 2018. The Alvarado scores of all patients were calculated and correlated with pathology and CT findings.
Results
A total of 198 patients aged between 5 and 18 years were reviewed, and 87 patients underwent surgery whereas 81 patients (40.9%, 81/198) were diagnosed with acute appendicitis pathologically. Six patients underwent negative appendectomy (6.9%, 6/87).
The mean Alvarado score was 7.3±1.6 in the appendicitis group and 3.9±1.7 in the nonappendicitis group (p<0.01). A total of 79 positive CT cases were detected in the group with clinically suspected appendicitis. The CT scan yielded 8 false-negative and 6 false-positive results. The sensitivity and specificity of CT scan were 90.1% and 94.8%, respectively, and the sensitivity and specificity of Alvarado score were 75.6% and 89.1%, respectively (p<0.01). The proportion of cases with appendicitis carrying an Alvarado score less than 3 was 4.2% (3/71), and that of patients with Alvarado score greater than 8 was 95.8% (46/48).
Conclusion
The Alvarado score facilitates risk stratification of patients and is expected to guide the reasonable use of CT scan especially in patients with low (less than 3) and high (more than 8) scores.
Acute appendicitis is the most common surgical condition of abdomen in children and the diagnosis is still challenging. The aim of this study was to evaluate the diagnostic value of the Alvarado score and computed tomography (CT) scan and to provide guidance for CT scan to reduce the number of CT examinations for clinically suspected acute appendicitis in children.
We retrospectively analyzed pediatric patients aged below 18 years and screened via abdominal CT for suspected appendicitis at Yeungnam University Hospital between January 1, 2013 and October 31, 2018. The Alvarado scores of all patients were calculated and correlated with pathology and CT findings.
A total of 198 patients aged between 5 and 18 years were reviewed, and 87 patients underwent surgery whereas 81 patients (40.9%, 81/198) were diagnosed with acute appendicitis pathologically. Six patients underwent negative appendectomy (6.9%, 6/87). The mean Alvarado score was 7.3±1.6 in the appendicitis group and 3.9±1.7 in the non-appendicitis group (p<0.01). A total of 79 positive CT cases were detected in the group with clinically suspected appendicitis. The CT scan yielded 8 false-negative and 6 false-positive results. The sensitivity and specificity of CT scan were 90.1% and 94.8%, respectively, and the sensitivity and specificity of Alvarado score were 75.6% and 89.1%, respectively (p<0.01). The proportion of cases with appendicitis carrying an Alvarado score less than 3 was 4.2% (3/71), and that of patients with Alvarado score greater than 8 was 95.8% (46/48).
The Alvarado score facilitates risk stratification of patients and is expected to guide the reasonable use of CT scan especially in patients with low (less than 3) and high (more than 8) scores.
Acute appendicitis is the most common acute abdominal condition in children warranting surgical intervention, and accounts for 5%–10% of emergency department visits by children [1, 2]. Recently, non-operative treatment has been advocated but prompt appendectomy is still the mainstay of treatment. Delayed intervention may increase complications such as perforation and abscesses while rushing to surgery is associated with a high negative appendectomy [3, 4].
A prompt and accurate diagnosis of appendicitis is essential to avoid morbidity and adverse outcome. Despite being a common disease, the diagnosis of appendicitis in children is frequently challenging because of several other conditions that mimic the clinical presentation of the disease in children in addition to difficulties in communication and examination. Therefore, abdominal imaging has become a common tool for the evaluation of suspected appendicitis in children [5]. Abdominal computed tomography (CT) has high diagnostic accuracy, and has been used routinely; however, the risk of radiation-induced malignancy in children is a significant concern [1, 5]. A number of clinical scoring systems have been developed as tools for risk stratification in an attempt to quantify and improve the accuracy of clinical assessment in diagnosing acute appendicitis [6].
The aim of this study was to evaluate and compare the diagnostic value of the Alvarado score and abdominal CT and develop a guidelines for CT scanning based on Alvarado scores to reduce the number of CT examination in the diagnostic workup of suspected appendicitis in children.
We retrospectively reviewed the medical records of patients aged below 18 years who underwent abdominal CT for suspected appendicitis between January 1, 2013 and October 31, 2018 at the Yeungnam University Hospital.
Patient demographic and clinical characteristics including age, sex, body mass index (BMI), duration of symptoms, body temperature, presence of anorexia, nausea/vomiting, tenderness and rebound tenderness on right lower quadrant (RLQ), migration of pain to the RLQ, white blood cell and neutrophil count, and C-reactive protein (CRP), and abdominal CT findings were reviewed. The criteria for diagnosis of acute appendicitis using abdominal CT include: swollen appendix (outer diameter exceeding 6 mm), wall thickening of appendix (>3 mm) and periappendiceal inflammatory strands. Patients who underwent surgery, the surgical records, and pathologic results were collected. The sensitivity and sensitivity of CT scans were calculated based on the pathology results of appendectomy.
Patients were divided into 2 groups: pathologically confirmed cases of acute appendicitis (A group) and non-confirmed cases (non-A group).
The Alvarado scores were calculated for each patient and correlated with final pathology reports and CT results (Table 1) [7]. Based on the Alvarado scores and pathology results, the incidence of patients with appendicitis was defined. The sensitivity and specificity of Alvarado score were calculated. According to the probability of appendicitis, patients were stratified into low, intermediate, and high-risk group.
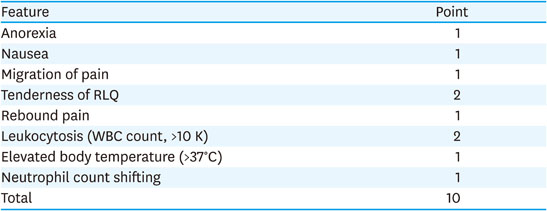
Table 1
Alvarado score system
The R software package was used to analyze data. Categorical variables were summarized as frequency and cross-tables, and the relationship between them was assessed using χ2 test. The diagnostic performance was assessed based on calculated values of sensitivity, specificity, positive and negative predictive values as well as area under the receiver operating characteristic (ROC) curves. Statistical significance was determined by a p-value of less than 0.05 for all tests.
This study was approved by the Institutional Review Board of Yeungnam University medical center (IRB No. 2020-08-034).
A total of 198 patients, aged between 5 and 18 years, were included in this study: 87 patients (43.9%) underwent surgery and 6 patients (6.9%) had normal histology. Pathologically confirmed patients (n=81) were included in the appendicitis group (A group) and patients with negative appendectomy results (n=6) and the remaining 111 patients were included in the non-appendicitis group (non-A group). Nine patients were excluded from the study owing to incomplete medical records.
The 198 patients in this study included 114 males and 84 females. There was no significant difference between both groups regarding age, sex, weight, and BMI. The A group exhibited a significant higher Alvarado score than the non-A group (p<0.01). Positive findings of abdominal CT were more frequent in the A group (p<0.01) (Table 2).
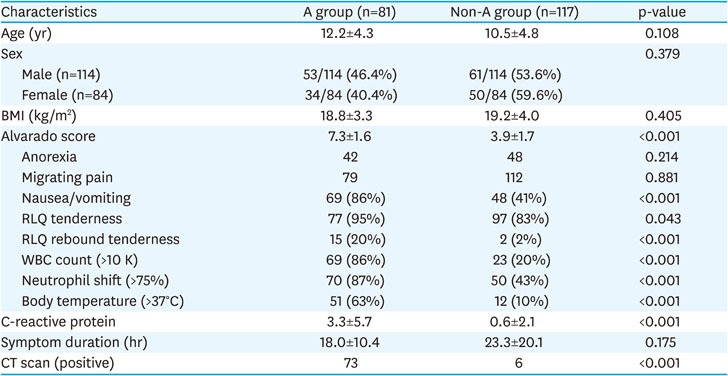
Table 2
Demographic and clinical characteristics of patients
A total of 118 negative and 80 positive CT scans for appendicitis were performed during the study period. Eight false-negative and 7 false-positive CT scans were identified. The sensitivity and specificity rates of abdominal CT were 90.1% and 94.0%, respectively. The 7 false positive CT scans led to 6 negative appendectomies for a negative appendectomy rate of 6.9% (6/87) (Table 3, Fig. 1).

Table 3
The Alvarado scores versus CT findings in appendicitis and non-appendicitis groups
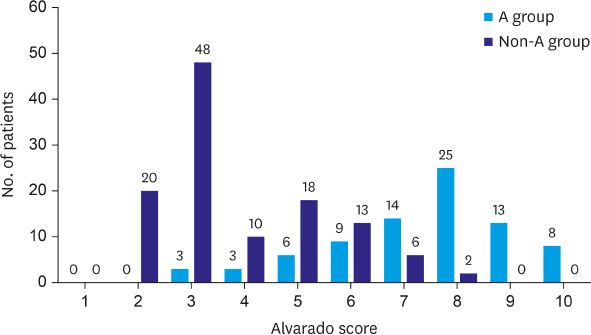
Fig. 1
The Alvarado scores of patients with and without appendicitis.
A group, appendicitis group; non-A group, non-appendicitis group.
The average Alvarado score for A group was 7.3±1.6 and non-A group was 3.9±1.7 and the sensitivity and specificity values of the Alvarado score were 75.6% and 89.1%, respectively. The areas under the ROC curve (AUC) for abdominal CT and the Alvarado score were 0.893 and 0.875, respectively (Fig. 2). The results of Alvarado scores of patients with and without appendicitis are shown in Fig. 1. They include 71 patients with Alvarado scores 3 or below and 3 of them had appendicitis (4.2%, 3/71). The diagnostic accuracy of Alvarado score 3 or lower in diagnosing healthy appendix was 95.8%. There were 48 patients with Alvarado scores 8 or higher and the incidence of appendicitis was 95.8% in 46 of them.
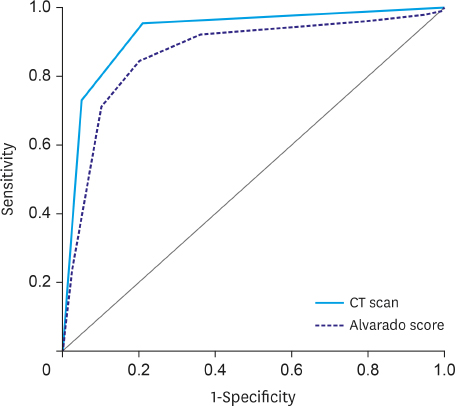
Fig. 2
Sensitivity and specificity of Alvarado score and CT scan. The AUC for abdominal CT scan and the Alvarado score were 0.893 and 0.875, respectively.
CT, computed tomography; AUC, areas under the receiver operating characteristic curve.
Abdominal imaging studies are usually employed as a diagnostic adjunct for children with suspected appendicitis because of the relatively poor diagnostic accuracy associated with clinical and laboratory data [1].
Abdominal ultrasound (US) is noninvasive, relatively inexpensive compared with CT and magnetic resonance imaging (MRI), and does not require sedation, contrast agent, or ionizing radiation [8]. However, its accuracy is highly affected by the examiner’s experience and the reported diagnostic accuracy of US varies widely with sensitivities ranging from 44% to 94% and specificities ranging from 47% to 95% [9]. Additionally, US is frequently unavailable during nights, weekends and holidays in many institutes including our hospital [9, 10].
Because of the high sensitivity (87%–100%) and specificity (89%–99%) [11, 12], abdominal CT has been the most frequently used imaging test to diagnose appendicitis. In addition to the accuracy, abdominal CT has several advantages over other imaging modalities including ready availability at most institutes, rapid acquisition time, lack of operator dependency [9, 10]. A few patients and parents are more confident when CT imaging is included as part of their evaluation [5, 13]. Kotagal et al. [1] reported that more than 50% of children underwent CT scan as their first imaging study. Anderson et al. [5] reported that the rate of CT use may be higher than 70% in community hospital.
Despite its diagnostic accuracy, concerns regarding ionizing radiation and risk of subsequent malignancy have prompted efforts to minimize the use of CT as the initial diagnostic imaging test in suspected pediatric cases of appendicitis. Two main strategies have been proposed. The first strategy entails decrease in the amount of radiation by reduction of the dosage or decreasing the size of exposed area (focused scan) below the lower pole of right kidney. The second approach involves decreased utilization by using a clinical scoring system and US examination either alone or prior to CT.
The Alvarado score is composed of 8 components with a total score of 10 (migration of pain, anorexia, nausea/vomiting, RLQ tenderness, rebound tenderness, increased temperature >37°C, leukocytosis >10,000/mL, and polymorphonuclear neutrophilia >75%) [7]. It was developed with the idea that the combined predictive value of clinical symptoms, physical examination, and laboratory data was greater than any of these sources of diagnostic elements considered individually [1, 14]. The calculated scores were divided into low, intermediate, and high range to suggest the likelihood of appendicitis and aid in management. In his original study, Alvarado recommended that patients with a score of 4 or lower should be discharged and patients with a score of 5 to 6 should be observed, and those with a score of 7 or higher undergo surgery for appendicitis [7]. In a prospective study of 588 patients, Schneider et al. [15] reported a sensitivity of 72% and specificity of 81%. In another prospective analysis, Mandeville et al. [16] reported a sensitivity of 76% and a specificity of 72%.
Results of these studies suggested that Alvarado score is not adequate as an independent diagnostic tool, particularly for intermediate range scores, but better as a tool for risk stratification in diagnosing appendicitis. Several studies reported the use of Alvarado score to reduce the role of CT in the evaluation of suspected appendicitis in children [17, 18]. Rezak et al. [18] suggested that patients with an Alvarado score 1 to 4 could be discharged without further imaging examination or another diagnostic evaluation. CT should be performed for patients with a score of 5 to 7, whereas patients with a score of 8 to 10 do not need further imaging. Such patients should undergo appendectomy. Blitman et al. [19] reported that only 1 case of appendicitis was found in 241 patients with an Alvarado score of 4 or below and a score of 9 or 10 was 100% predictive of appendicitis.
In our study, we found that using Alvarado score of 3 or below to exclude appendicitis would have missed 3 cases in 71 patients, whereas using a score of 8 or higher as an indication for surgery would have led to 2 cases of negative appendectomy in 48 patients with a negative appendectomy rate of 4.1%. The results of this study showed that in children with suspected appendicitis, patients with an Alvarado score of 3 or below and 8 or higher routinely should be excluded and only those with an Alvarado score of 4–7 should be diagnosed with CT, thereby nearly 60% of CT examination could be eliminated with acceptable missed rates and negative exploration rate.
The limitations of this study related to the small sample size and the single institute setting. The nature of this study was retrospective and calculation of Alvarado score might be less reliable due to physical examination by several physicians. All findings should be validated in larger, prospective study.
In conclusion, the Alvarado score is a useful and relatively accurate tool for risk stratification of patients with suspected appendicitis. Abdominal CT usage could be avoided in low- and high-risk patients based on the score.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: L.N.H., J.H.M.
Data curation: J.H.M.
Formal analysis: J.H.M.
Methodology: J.H.M., L.N.H.
Supervision: L.N.H.
Validation: J.H.M., L.N.H.
Writing - original draft: J.H.M.
Writing - review & editing: L.N.H., J.H.M.
