

Infantile hemangiomas are the most common vascular tumors of infants and are characterized by abnormal proliferation of endothelial cells and aberrant blood vessel architecture. The drug Sirolimus has been explored as a new therapeutic option in the management of vascular anomalies that do not respond to conventional treatments. This report presents a case of refractory multiple infantile hemangiomatosis with brain involvement that was successfully treated with sirolimus.
Infantile hemangiomas are the most common vascular tumors of infants and are characterized by abnormal proliferation of endothelial cells and aberrant blood vessel architecture. The drug Sirolimus has been explored as a new therapeutic option in the management of vascular anomalies that do not respond to conventional treatments. This report presents a case of refractory multiple infantile hemangiomatosis with brain involvement that was successfully treated with sirolimus.
Infantile hemangiomas (IHs) are the most common vascular tumors of infants and are characterized by abnormal proliferation of endothelial cells and aberrant blood vessel architecture [1, 2, 3, 4, 5, 6]. These tumors are present at birth and undergo a proliferative growth phase for up to a year, followed by stabilization and spontaneous involution over several years [4, 7]. Typically, these tumors do not pose functional or cosmetic threats, although, medical intervention is required in approximately 10%–20% of cases because of complications such as ulceration, bleeding, infection, disfigurement, functional impairment, airway obstruction, or cardiac compromise [7, 8, 9].
Mammalian target of rapamycin (mTOR) inhibitors have been explored as a new therapeutic option in the management of refractory vascular anomalies that do not respond to conventional treatments such as resection, sclerotherapy, propranolol, and steroids [10, 11, 12, 13]. Sirolimus, also known as rapamycin, is an allosteric inhibitor of mTOR. We present an infant case of refractory hemangiomatosis with brain involvement that was successfully treated with sirolimus.
A 2-day-old male infant visited our pediatric emergency center with bleeding from perianal cutaneous lesions. He was born at a gestational age of 38 weeks and 5 days by normal full-term spontaneous delivery, and had a birth weight of 4,080 g. He has no family history of vascular malformation, but his father had a history of being treated for a subarachnoid hemorrhage due to an unknown ruptured cerebral aneurysm at the age of 35. Vital signs including body temperature, heart rate, respiration, and blood pressure were within normal ranges. The skin lesions were purpuric to cherry-red in color, and multiple cutaneous lesions were present on the scalp, neck, trunk, extremities, and perianal area. The lesions were present at birth and had diameters ranging from 1 to 10 mm (Fig. 1). There was fine anal bleeding, but there were not any symptoms related to involvement of anal sphincter.
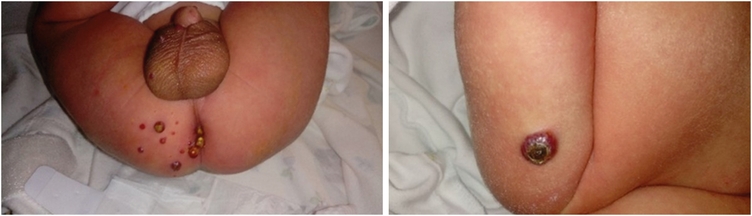
Fig. 1
Multiple cutaneous skin lesions on scalp, neck, trunk, extremities, and perianal area before treatment.
Laboratory evaluations, including a complete blood count with platelet, hemoglobin, coagulation battery, and D-dimer assessment, and liver function, renal function, serum electrolytes, and thyroid function tests, were within normal limits or negative. Abdominal ultrasonography showed mild left pelviectasis (7 mm). Soft tissue mass ultrasonography showed multiple hypoechoic solid masses with markedly increased vascularity, suggesting hemangiomas (Fig. 2). Whole body magnetic resonance imaging (MRI) showed a numerous enhancing skin, subcutaneous, and muscular lesions throughout the body, and a multiple lobulated enhancing mass with a central non-enhancing portion along the anus and buttock areas and involving the right sided of the anal sphincter. Brain MRI demonstrated multiple variably-sized enhancing lesions in the right cerebellum, right medial temporal lobe, left thalamus, and right parietal lobe, with marked perilesional edema; the largest in the right parietal lobe measured up to 6.5 mm (Fig. 3). Echocardiography showed unremarkable findings. Neurologic and eye examinations revealed no abnormalities. To confirm whether multiple hemangiomas are related to genetic abnormality, we additionally performed chromosomal analysis. The test showed no chromosomal structural abnormalities and was 46, XY, which is normal karyotype.
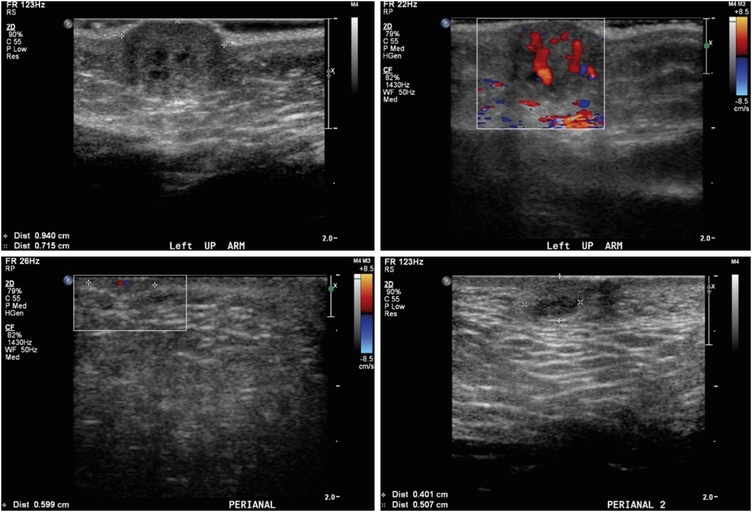
Fig. 2
Soft tissue mass ultrasonography before treatment.
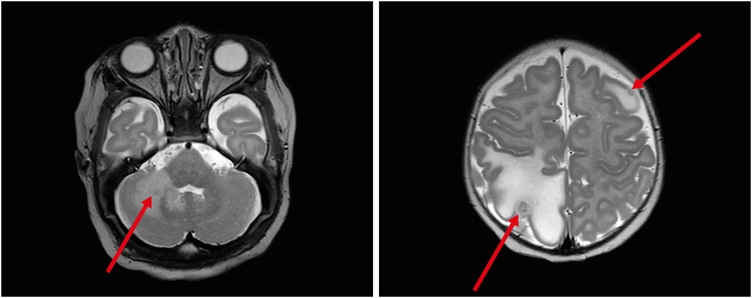
Fig. 3
Brain magnetic resonance imaging before treatment.
We decided to try medical intervention because there were fine anal bleeding and anal discharge during defecation due to hemangioma, and the number was increasing. We initiated treatment with oral propranolol (2 mg/kg/day) and local triamcinolone injection from the 14th postnatal day for a total duration of 1 month. There were no significant adverse effects such as hypoglycemia, bradycardia, and hypotension, and so forth. However, the size and number of the hemangiomas had increased over the treatment period (Fig. 4A). Oral prednisolone (1 mg/kg/day) was added as a second-line treatment for 2 weeks, but no clinical response of treatment was observed.
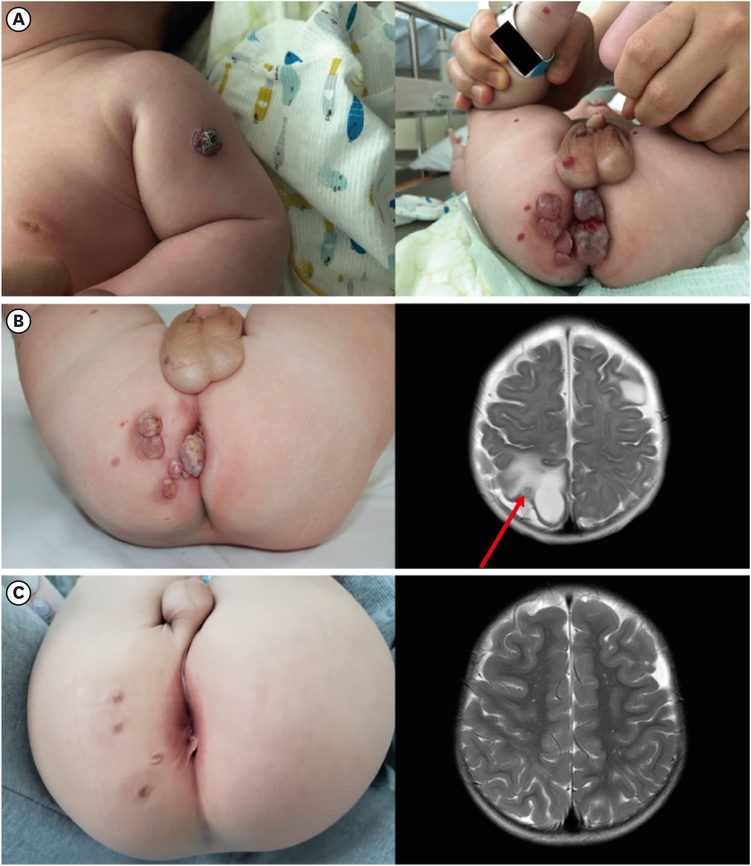
Fig. 4
(A) After 1 month of propranolol treatment. (B) After 1 month of sirolimus and propranolol treatment. (C) After 18 months of sirolimus and propranolol treatment.
Following discussions between a multidisciplinary team consisting of a pediatric surgeon, dermatologist, radiologist, pediatric oncologist, neurosurgeon, and neurologist, we finally decided to try treatment with both oral sirolimus and propranolol (3 mg/kg/day). The patient was administered oral doses of sirolimus 0.8 mg/m2 every 12 hours as the initial dose. The therapeutic drug monitoring (TDM) range was 8 to 10 ng/mL. No adverse effects from sirolimus were noted in the baby. After 1 months, the patient responded to sirolimus treatment with a reduction in the size and number of lesions (Fig. 4B). After 9 months, brain MRI showed complete involution of the cranial hemangiomas. We tried to wean off sirolimus every 2 to 3 months. Treatment for the hemangiomas was stopped 18 months after sirolimus treatment was began (Fig. 4C). The lesions were scheduled for follow-up with a repeated MRI and clinical measurements every 6 to 12 months after treatment cessation (Fig. 5). No additional lesions were identified during follow-up period. The patient is currently 4 years old and maintains normal growth and neurodevelopment without recurrence.
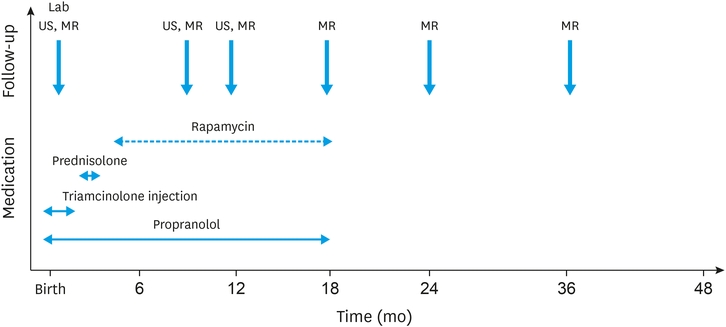
Fig. 5
Timeline of patient’s medications and follow-up.
US, ultrasonography; MR, magnetic resonance imaging.
The efficacy of sirolimus in the treatment of vascular anomalies was previously described [10, 11]. This report describes a case of refractory multiple infantile hemangiomatosis with brain involvement that was treated with sirolimus. Our experience supports prior studies indicating that sirolimus is effective for vascular anomalies including IH refractory to conventional therapy.
The PI3K/Akt/mTOR pathway plays a key role in cell growth and proliferation. Activation of the PI3K/Akt/mTOR pathway can also increase expression of the vascular endothelial growth factor, that regulate angiogenesis and lymphangiogenesis [10, 11]. mTOR inhibitors directly inhibit mTOR, blocking downstream protein synthesis and thereby presenting antitumoral and antiangiogenic effects. Sirolimus recently showed efficacy in the treatment of vascular anomalies, but as a treatment for hemangioma, it has only been presented in a limited number of cases. Warren et al. [14] and Lekwuttikarn et al. [15] reported that diffuse hepatic hemangiomas were successfully treated using sirolimus and propranolol, and Hutchins et al. [16] and Dávila-Osorio et al. [17] also reported treatment of refractory IHs with sirolimus. From the limited experience available, it can be inferred that the treatment of refractory hemangioma is helped by the combined use of sirolimus and propranolol. Randomized controlled trials of sirolimus treatment of refractory hemangioma are required, including additional comparative studies of the differences between sirolimus alone and in combination with propranolol.
The safety of sirolimus is a major concern in the treatment of vascular anomalies, as most patients require long-term treatment and are most often of pediatric age [18]. Important questions about the most appropriate dosage and duration of treatment for the patient remain unanswered [10]. The effects of sirolimus on human vascular endothelial cell anomalies are concentration dependent, [19] and its use requires a risk-benefit evaluation and follow-up with possible adverse effects [18]. The most common side effects are oral mucositis, dyslipidemia, leukopenia, infection, gastrointestinal symptoms, and cutaneous reactions [18]. Hence, the target blood sirolimus through level should be monitored. In this case, the TDM level of sirolimus was maintained at 8 to 10 ng/dL, and performed at intervals of 2 days until stabilization. The interval of TDM gradually increased to one week, 2 weeks, and one month. Monitoring was performed through imaging and clinical measurements at 3, 6, and 12 months. More research is needed to determine whether the onset, duration, intervals, and cessation of sirolimus are suitable for the management of multiple infantile hemangiomatosis.
In conclusion, sirolimus may be worth considering in the case of complex and life-threatening hemangiomas that do not respond to first-line therapies.
Funding:This study was approved by the Institutional Review Board of Asan Medical Center (approval number: 2022-0457).
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.Y.
Data curation: K.D.Y.
Formal analysis: P.S.J., K.D.Y.
Supervision: K.D.Y.
Validation: P.S.J., K.D.Y.
Writing - original draft: P.S.J.
Writing - review & editing: P.S.J., K.D.Y.
The authors thank Bioedit (https://www.bioedit.kr) for English language editing.
