

Purpose
Temporary stoma formation is a common procedure in pediatric surgery. Surgical site infection after stoma reversal surgery is a common complication, and the cosmetic effect after skin suturing is reduced. Purse-string closure has been suggested for stoma reversal, preventing surgical site infections and providing better cosmesis. Positive results have been reported abroad for the purse-string closure technique for stoma reversal in pediatric patients; however, no cases have been reported in Korea. Therefore, we aimed to investigate the outcomes of purse-string closure for stoma reversal in pediatric patients.
Methods
From October 2018 to September 2022, all pediatric patients who underwent stoma reversal at the Department of Pediatric Surgery were included. The electronic medical records of the patients were retrospectively reviewed. The following variables were analyzed: perinatal data including gestational age, sex, birth weight, Apgar score, and types of delivery; preoperative conditions including total parental nutrition, steroid use, and tracheal intubation; operational data such as diagnosis, types of stoma, age, body weight, skin closure methods and operation time; and postoperative data such as surgical site infection, transfusion, days until extubation, and start of enteral feeding. The serial wound healing process after purse-string closure was documented using photographs.
Results
Thirty-seven patients underwent stoma reversal surgery, 14 underwent purse-string closure, and 23 underwent conventional lineal closure. No surgical site infection occurred in the purse-string group and four cases of surgical site infection occurred in the conventional liner group. However, there were no statistically significant differences between both groups (p=0.276).
Conclusion
No surgical wound infection was found in pediatric patients who underwent purse-string closure for stoma reversal, and the cosmetic effect was promising. However, no statistically significant difference was found between the purse-string closure and conventional linear closure groups. Further multicenter studies involving a larger sample size are needed to determine statistical significance.
Temporary stoma formation is a common procedure in pediatric surgery. Surgical site infection after stoma reversal surgery is a common complication, and the cosmetic effect after skin suturing is reduced. Purse-string closure has been suggested for stoma reversal, preventing surgical site infections and providing better cosmesis. Positive results have been reported abroad for the purse-string closure technique for stoma reversal in pediatric patients; however, no cases have been reported in Korea. Therefore, we aimed to investigate the outcomes of purse-string closure for stoma reversal in pediatric patients.
From October 2018 to September 2022, all pediatric patients who underwent stoma reversal at the Department of Pediatric Surgery were included. The electronic medical records of the patients were retrospectively reviewed. The following variables were analyzed: perinatal data including gestational age, sex, birth weight, Apgar score, and types of delivery; preoperative conditions including total parental nutrition, steroid use, and tracheal intubation; operational data such as diagnosis, types of stoma, age, body weight, skin closure methods and operation time; and postoperative data such as surgical site infection, transfusion, days until extubation, and start of enteral feeding. The serial wound healing process after purse-string closure was documented using photographs.
Thirty-seven patients underwent stoma reversal surgery, 14 underwent purse-string closure, and 23 underwent conventional lineal closure. No surgical site infection occurred in the purse-string group and four cases of surgical site infection occurred in the conventional liner group. However, there were no statistically significant differences between both groups (p=0.276).
No surgical wound infection was found in pediatric patients who underwent purse-string closure for stoma reversal, and the cosmetic effect was promising. However, no statistically significant difference was found between the purse-string closure and conventional linear closure groups. Further multicenter studies involving a larger sample size are needed to determine statistical significance.
Temporary stoma creation is widely performed to save the lives of pediatric patients by diverting stool passage through the stoma. Several conditions such as anorectal malformation, necrotizing enterocolitis, spontaneous intestinal perforation, meconium-related ileus, Hirschsprung’s disease, and trauma are common indications for stoma creation in pediatric patients. The stoma is reversed several months after placement, with surgical site infection (SSI) being the most common complication following the procedure [1]. There have been many efforts to reduce SSI after stoma reversal, including application of antibiotics, stoma implantation into the subcutaneous tissue, modification of suturing time, and different skin closing methods [1, 2, 3]. Purse-string closure (PSC) for stoma reversal was first mentioned in the literature in 1997 [4]. Several comparative and contrasting articles have investigated the postoperative complications and cosmetic effects of both PSC and conventional linear closure (CLC) methods in adult patients [1, 5, 6, 7]. Studies using PSC for stoma reversal in pediatric patients have been published overseas [8, 9]; however, PSC for stoma reversal in pediatric patients in Korea has not yet been reported. Our study aimed to compare the outcomes of CLC and PSC for stoma reversal in pediatric patients, focusing on SSI, and also to examine the wound healing process with the PSC method.
All pediatric patients who underwent a stoma reversal operation at the Pediatric Surgery Department of Keimyung University Dongsan Medical Center between October 2018 and September 2022 (36 months) were included. The patients’ electronic medical records were retrospectively analyzed. The following variables were examined: patient age, sex, gestational age, birth weight, Apgar score, disease for stoma creation, types of stoma, age at the time of stoma reversal surgery, preoperative total parenteral nutrition (TPN), preoperative steroid use, preoperative tracheal intubation, interval between stoma creation and stoma reversal, operative time, postoperative wound infection, postoperative transfusion, time required to heal the wound, and the appearance of postoperative wounds over time. All surgeries were performed by two pediatric surgeons, with the exception of one case, which was performed by an expert colorectal surgeon.
SSI was evaluated by surgeons who performed stoma reversal operations according to the surveillance definition of the Centers for Disease Control and Prevention (CDC)/National Healthcare Safety Network (NHSN) [10]. There are two types of SSI: superficial incisional SSI and deep incisional SSI. SSI is defined as an infection that occurs within 30 days of surgery. The symptoms and signs of SSI include purulent drainage from the superficial incision, pain or tenderness, localized swelling, redness, or heat. In addition to these signs and symptoms, deep incisional SSI also includes spontaneous deep incision dehiscence or fever (>38°C) [10].
The surgical processes of stoma reversal before skin closure were the same in both groups. Bowel preparation was performed differently depending on the patient’s condition and enterostomy type. Mechanical bowel cleansing through an enema was not performed in any patient. Antibiotics were administered by an intravenous injection of 3rd generation cephalosporin 30 minutes to one hour prior to surgery. Under general anesthesia, a circular or oval incision was made in the skin along the stoma with a Bovie using the cutting mode. After separating the stoma from the subcutaneous and fascia layers, the intestine was exposed and minimally resected, and an end-to-end anastomosis was performed with a hand-sewn interrupted suture. The restored intestine with an anastomosis was placed into the abdominal cavity, and the abdominal wall muscle and fascia layer were sutured with an interrupted linear suture using absorbable sutures. In the next step, the CLC and PSC differed, with the PSC method performed as follows: the subcutaneous tissue was sutured using the purse-string method with absorbable 3-0 suture (Fig. 1A), and the skin edges were tightened by pulling the thread, leaving a 2–3 mm gap (Fig. 1B). The sutures were then tied together.
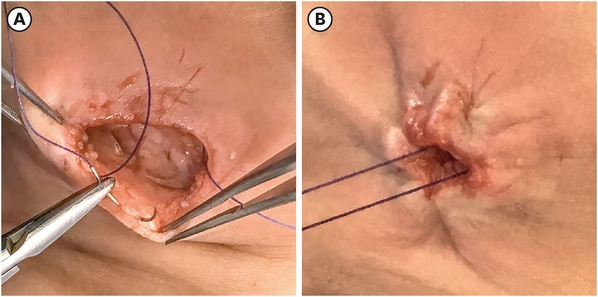
Fig. 1
CHow to perform purse-string closure method. (A) Suturing the subcutaneous tissue using purse-string closure method. (B) Ligation by pulling the thread with a free space of 2–3 mm.
Statistical analysis was performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). An independent t-test was performed to compare the means of the quantitative variables. The chi-square test or Fisher’s exact test was used for the qualitative variables. Statistical significance was set at p<0.05.
This study was approved by the Medical Research Ethics Review Committee of Keimyung University Dongsan Medical Center (IRB 2022-06-013) and informed consent was waived due to the retrospective nature of the study. No personally identifiable information is included.
This study included 37 pediatric patients (23 males and 14 females) who underwent stoma reversal surgeries. The mean gestational age was 30.1±5.2 weeks and the mean birth weight was 1,491±1,008 g. The mean Apgar score was 5.4±2.1 at 1 minute and 7.4±1.5 at 5 minutes. The most common cause of stoma formation was necrotizing enterocolitis (nine patients [24.3%]), followed by meconium related ileus (eight patients [21.6%]), imperforate anus (six patients [16.2%]) and other diseases including ileal atresia, colon stricture, colon atresia, gastric perforation, ileus, intussusception, and traumatic perforation. When looking at the types of stoma, eight cases of colostomy and 29 cases of ileostomy or jejunostomy were found. The mean body weight during the stoma reversal operation was 4.2±4.5 kg. The mean duration from stoma formation to stoma reversal surgery was 83.3±82.3 days.
PSC was performed in 14 patients and CLC in 23 patients. There were no statistical differences in perinatal characteristics, including gestational age, birth weight, Apgar score, and type of delivery between the PSC and CLC groups. Statistically significant differences were found between the sexes (p=0.035) (Table 1). Perioperative data between the PSC and CLC groups were also analyzed: causative disease for stoma creation, types of stoma, preoperative TPN, preoperative steroid use, preoperative intubation, body weight, time interval between stoma creation and reversal, operation time, age, and SSI. There were no statistically significant differences between these variable (Table 2). There were no cases of SSI in the PSC group (0%) while there were four cases of SSI (17.4%) in the CLC group. However, no statistical difference was found between both groups. Variables thought to have an impact on SSI were analyzed between the SSI (n=4) and non-SSI groups (n=33). All variables believed to affect SSI—birth weight, type of stoma, body weight and age at stoma reversal operation, preoperative TPN, steroid and intubation, time interval between stoma creation and reversal, operation time, skin closure method, postoperative transfusion, duration of extubation, and days to enteral feeding—showed no statistical difference between the SSI and non-SSI group (Table3).
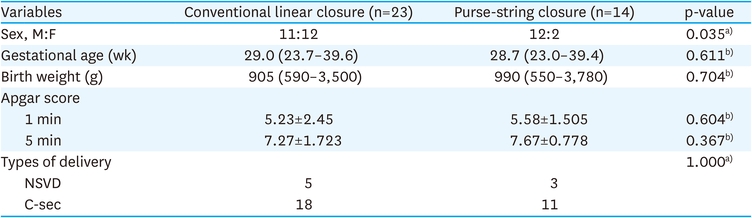
Table 1
Demographic characteristics of the patients
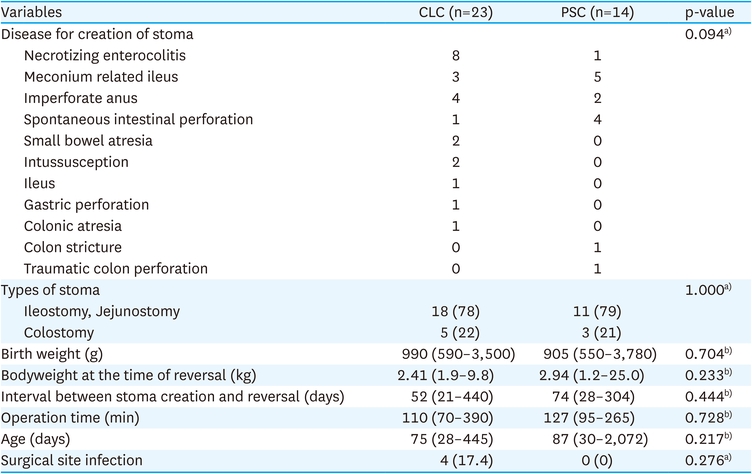
Table 2
Perioperative data of the two groups; CLC vs. PSC
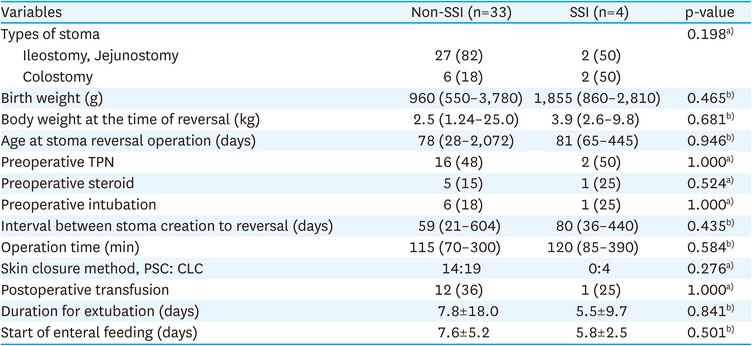
Table 3
Variables associated with surgical site infection
Fig. 2A-D show the consecutive recovery process of the surgical wound over time. In general, the epidermis was restored 4–7 days post-operation and any wrinkles were smoothed out. The sutures were not removed, as absorbable sutures were used. The wound was restored to a visually inconspicuous state six months postoperatively (Fig. 3).
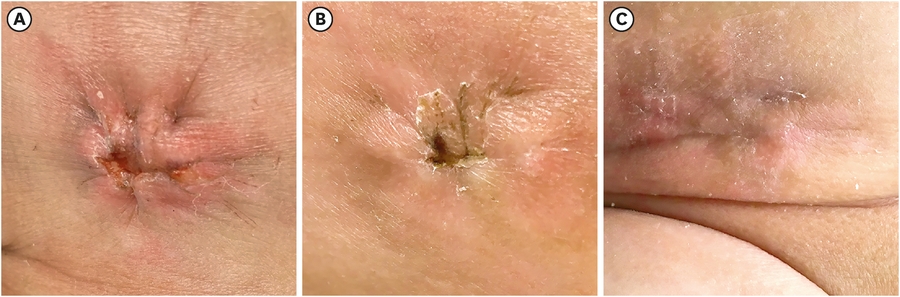
Fig. 2
Serial photographs of wound healing after ileostomy reversal with purse-string skin closure. (A) POD 1, (B) POD 7, (C) POD 13.
POD, post-operative day.

Fig. 3
Long-term follow-up of the closed wound with purse-string method; six months after ileostomy reversal.
The most common complication related to stoma reversal is SSI, with a high reported rate of 40%, with no significant difference in its occurrence noted among adult and pediatric patients [1, 7, 11]. According to the Hospital Infection Control Practices Advisory Committee (HICPAC) of the CDC, SSI can be diagnosed based on symptoms or evidence of infection, such as pain, tenderness, local swelling, or redness [12, 13]. Various studies have found that long operation time, age, Hirschsprung’s disease, and heart risk factors increase the risk of SSI, and the use of bowel cleansing, warming, antibiotics, and skin cleansers reduces the incidence of SSI [14, 15]. There was also a difference in the incidence of SSI according to the closure method after stoma reversal [16, 17, 18], and the incidence of SSI was 0% in 51 patients for 6 weeks after using the purse-string closure method [19]. A remarkably low incidence of SSI, shortened hospital stay, and cosmetic superiority were reported in pediatric patients after purse-string closure [8, 9]. There was no SSI after PSC in 14 patients with stoma reversals, whereas 17% of SSI after CLC (four out of 23) occurred in our study. There was no statistically significant difference between the two groups, which may have occurred due to the small sample size of this study.
Although our study results did not demonstrate a statistically significant difference in the incidence of SSI, the advantages of PSC should not be ignored. In the CLC group, 3 of four patients who developed SSI needed reoperation to close the fascia due to wound dehiscence of deep SSI. One patient in the PSC group had an exiguous seroma under the closed wound on the fifth postoperative day of ileostomy reversal. However, the seroma was easily drained through the gap in the center of the wound, and the wound did not develop SSI. In the case of purse-string sutures, an empty space is created for ligation with a gap of 2–3 mm, through which a seroma or hematoma can be drained. For this reason, it is believed that the frequency of SSI occurrence is low [9].
Milanchi et al. developed a patient wound healing satisfaction scale to evaluate patient satisfaction after stoma reversal of circumferential subcuticular wound approximation and primary closure; patients who received circumferential subcuticular approximation tended to have a higher scores, although the difference was not statistically significant [7]. Other reports analyzed the cosmetic and functional outcomes of PSC using the patient and observer scar assessment scale: pain, itchiness, discoloration, stiffness, and thickness [20]. In this study, however, we could not investigate the satisfaction of pediatric patients with surgical wounds through their caregivers. As a follow-up study, it is necessary to develop questions to evaluate the satisfaction with the healing of the surgical wound, including cosmetic outcomes and functional aspects. The cosmetic outcomes of PSC were satisfactory in the surgeons’ eye. The pulling of the thread after penetrating through the subcutaneous tissue created wrinkles, which generally improved 4–7 days postoperatively. Around two weeks after the operation, the wrinkles improved remarkably and the wound recovered to a relatively flat state. The wound was difficult to visualize, even after a longer follow-up period.
The purse-string closure technique is easier to perform than the conventional linear skin closure from the surgeon’s subjective point of view. When round or oval wounds are linearly closed, the edges often protrude; in many cases, it is difficult to correct the protruded edges surgically. Additionally, infants younger than a few months—especially those born prematurely—have very delicate skin. The skin around the stoma is irritated by stool and becomes inflamed; the skin is easily torn by sutures when the CLC method is used. As a result, the cosmetic effect is reduced. In contrast, the damage to the skin edge is less with the PSC method, because the suture passes through the subcutaneous tissue without penetrating the epidermis. PSC is relatively easy to perform, even on inflamed tissue or in premature infants with delicate tissue.
There were no SSI in pediatric patients who had undergone purse-string closure for stoma reversal, although there were no statistical differences between the PSC and PLC groups. Good cosmetic results were obtained when the wounds were healed. Additionally, this surgical technique is easy to perform and can shorten the skin closure operation time. Therefore, PSC is recommended as the skin closure method for stoma reversal in pediatric patients. However, the number of patients who underwent this procedure in this study was small; therefore, the results were not conclusive. A multicenter prospective study with a large sample size is needed to determine the statistical significance, and survey of patients or caregivers will be needed to evaluate cosmetic results.
Funding:This research was supported by a Bisa Research Grant from Keimyung University in 2020 (20200192).
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Scientific Meetings:Presented at the 38th annual meeting of the Korean Association of Pediatric Surgeons, 10th June 2022, Yeosu.
Author Contributions:
Conceptualization: K.E.J.
Data curation: K.E.J.
Formal analysis: K.E.J.
Funding acquisition: K.E.J.
Investigation: K.E.J.
Resources: J.E.
Supervision: J.E.
Validation: J.E.
Visualization: K.E.J.
Writing - original draft: K.E.J.
Writing - review & editing: J.E.
The authors thank the registered nurses Yun Ji Hee, Lee Seul Gi, and Lee Su Bin for their assistance in caring for patients in the pediatric surgery department.
