

Hydatid disease and tuberculosis are both endemic in India. The involvement of the kidney in any of these diseases is rare and co-occurrence of both pathologies at the same time is extremely rare. The common characteristics of both conditions i.e., remain asymptomatic for a long duration and present with non-specific symptoms make the diagnosis challenging. Moreover, the treatment of both pathologies at the same time requires multifaceted medical management and surgical intervention at the optimal time. Here, we are describing a case of renal hydatid with tuberculosis in a child, its presentation and management along with the review of pertinent literature.
Hydatid disease and tuberculosis are both endemic in India. The involvement of the kidney in any of these diseases is rare and co-occurrence of both pathologies at the same time is extremely rare. The common characteristics of both conditions i.e., remain asymptomatic for a long duration and present with non-specific symptoms make the diagnosis challenging. Moreover, the treatment of both pathologies at the same time requires multifaceted medical management and surgical intervention at the optimal time. Here, we are describing a case of renal hydatid with tuberculosis in a child, its presentation and management along with the review of pertinent literature.
Hydatid disease (HD) and tuberculosis (TB) are both endemic in India with a prevalence of 5%–11% and 27% respectively. HD commonly involves the liver (50%–70%) and lungs (20%–30%) while TB commonly affects the lungs. Rarely, HD and TB can affect other organs like the heart, liver, soft tissue, and kidney [1]. The incidence of renal HD and renal TB is 2% and 3-4% respectively in all the cases of HD and TB [2, 3]. In Korea, both the diseases are not endemic, but they are on a rise due to travelers and immigrants. The incidence of TB is 77 per 100,000 population while HD is very rare and only 38 echinococcosis cases have been reported in Korea [3, 4].
Low socioeconomic status and poor hygiene habits are the risk factors for both diseases. As such, it is very rare to have both the pathology at the same time and in the same organ. Here, we are discussing the presentation and management of renal HD with TB in a child.
A 6-year-old male child (126 cm height, 26 kg weight, body mass index of 16.88 kg/m2) resident of Himachal Pradesh, India, presented with vague abdominal pain for the past 2 years. There was no history of abdomen distension, hematuria, dyspnea, chest pain, loss of weight, or contact with a pet animal or TB patient. There was no similar history among the family members. The child was hemodynamically stable and on examination, a firm lump was palpable in the right lumbar region. Ultrasonography (USG) showed a cystic mass (7.3×7.2 cm) with internal echoes at the right suprarenal location. Chest X-ray was normal and there were no specific changes (Fig. 1A) The contrast-enhanced computed tomography (CECT) abdomen (Fig. 1B) showed an 8.7×6.6 cm cystic lesion arising from the upper pole of the right kidney, with fine internal septations. No enhancing solid component, fat, calcifications, or air was seen in the lesion. The lesion has a large exophytic component which was scalloping the posteroinferior surface of the right lobe of the liver. The renal vessels were normal. The blood investigations including complete blood count (haemoglobin 11.7 g/dL, white cell count 13,700 cells per mm3, platelets 373,000 per mm3, eosinophils 4%), renal function test (urea 23 mg/dL, creatinine 0.7 mg/dl), and liver function test (total bilirubin 0.39 mg/dL) were normal, serological test (indirect hemagglutination) for HD was negative. On clinical presentation and radiological images, the possibility of a cystic variant of Wilms tumor (WT) was kept and the child was taken up for exploration with the consent of right partial nephrectomy. On laparotomy, a tense cystic lesion was noted arising from the upper pole of the kidney (Fig. 2A), abutting the lower surface of the liver. On aspiration, 70 mL of clear fluid (hydatid fluid) was aspirated from the cyst, 10% betadine was instilled into the cyst and kept for 20 minutes, re-aspiration was done followed by deroofing of the cyst (Fig. 2B), a single hydatid cyst (size 10×8 cm) was removed without any spillage. A drain was placed in the cyst and the abdomen was closed. The post-operative period was uneventful. The histopathology report (Fig. 2C) of hydatid fluid and excised cyst wall turned out to be hydatid cyst with tuberculosis i.e., presence of AFB bacilli along with hydatid. The pediatric pulmonologist’s opinion was taken, and the child was started on anti-tubercular treatment (ATT). In ATT regimen, child had received isoniazid (H), rifampicin (R), ethambutol, and pyrazinamide for 2 months followed by 4 months of H and R. At the same time, child had also received 3 cycles of albendazole and each cycle comprise of albendazole 10 mg/kg/day for 21 days followed by 3 weeks gap before next cycle. At 6-months follow-up, the child was doing well and on USG abdomen there was no residual cavity.
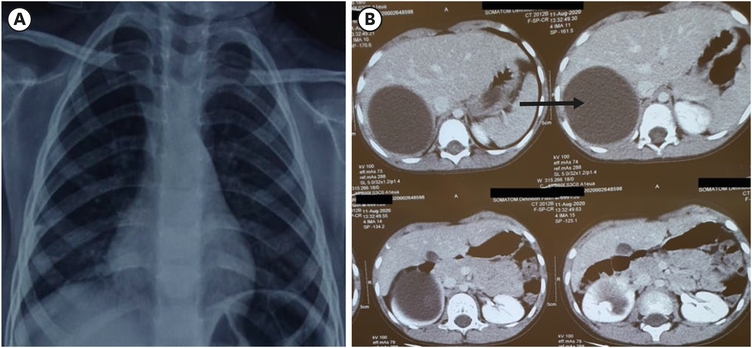
Fig. 1
Showing X-ray chest (A) with no specific changes and computed tomography scan abdomen (B) showing large cystic lesion at the upper pole of the right kidney.
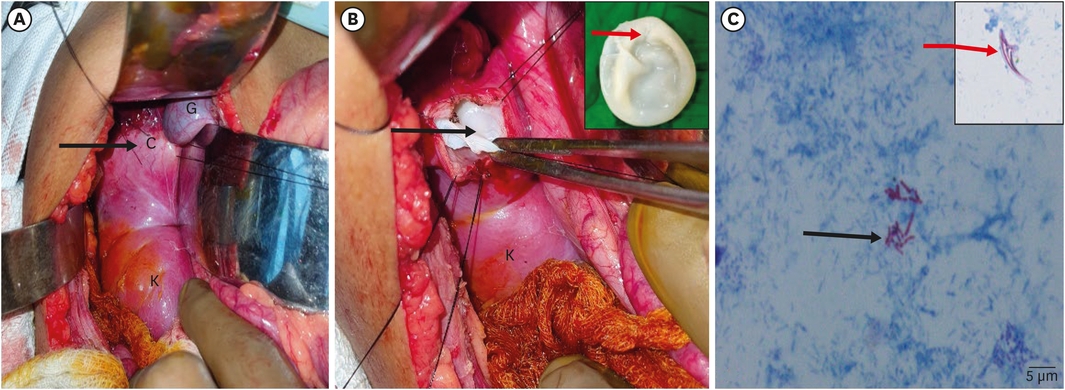
Fig. 2
Intraoperative image. (A) Tense whitish cystic lesion (black arrow) at the upper pole of the kidney near the gall bladder. (B) Open cyst cavity (black arrow) which showed hydatid cyst and it was removed completely (red arrow, inset). (C) Smear (Ziehl Neelsen stain, magnification ×1,000) showing numerous long slender, beaded acid-fast bacilli (black arrow) and hooklet of hydatid (red arrow, inset).
C, cyst; K, kidney; G, gall bladder.
HD can affect the pediatric age group because of the closeness with pets [5]. Most of the time, HD remains a silent disease and manifests only when grown to a significant size or complicated with infection or rupture that leads to the release of content into adjacent body cavities. Renal HD usually presents with symptoms of dull aching pain and sometimes as a palpable lump as presented in the index case. Rarely, few renal hydatid may present as hydatiduria with renal colic [6].
Children get HD infection through ingestion of contaminated food and water. The eggs transform into larvae in the intestine and migrate through the mesenteric circulation. The first filtration site is liver (most common involved organ) and the second site of filtration is the lung (second most common site). Any organ can be infected through hematogenous dissemination and renal involvement represents 4% of all cases in compare to the liver or lung [7].
Renal TB is usually secondary to pulmonary tuberculosis (PTB) and may present 1–10 years after PTB [8]. The symptoms most seen are increased frequency of micturition (44%), burning micturition (24%), haematuria (20%), fever, and constitutional symptoms (20%). Persistence of pyuria with sterile culture should lead to a strong suspicion of renal TB [8].
The nature and symptomatology of both the pathologies have common characteristics i.e., remain asymptomatic for a long time and present with non-specific symptoms. Although, the site i.e., the kidney is very rare for individual pathology, and co-occurrence of both diseases is exceptional. The usual site for both the disease is the lung and there are few reports of co-occurrence of TB and HD in the lung [9]. Verma et al. [10], reported a 17-year-old boy with TB and HD of the lung along with cardiac HD. The child presented with chronic cough and expulsion of whitish glistening material as sputum. CECT chest and bronchoalveolar lavage (BAL) fluid analysis had confirmed the diagnosis. The child was treated medically with ATT and albendazole followed by surgery [10]. Moscatelli reported a case of renal hydatid in a 5-year-old who presented with weight loss and palpable right upper quadrant lump [5]. The patient received albendazole, before surgical intervention. Renal hydatid can be misdiagnosed as a tumor, as reported by Uçar et al. [11]. A 15-years-old female presented with abdominal pain and was diagnosed to have a cystic swelling arising from the lower pole of the right kidney and mimicked as a tumor. The index case was also presented with similar complaints, the hydatid serology was negative and so the diagnosis of the renal tumor was kept as one of the differentials in the preoperative period.
The co-existence of both i.e., renal hydatid with tuberculosis has not been reported yet in the English literature. There have been theories regarding changes in the immune system in presence of both pathologies. The HD predisposes to the development of TB, the oncosphere activates the complement system, which leads to the death of the host cells surrounding the oncosphere decreasing the strong complement-mediated immune response. This leads to the generation of T-suppresser cells and pattern change of the immune system from T helper (Th) 1 to Th2 cells, leading to impair macrophage and lymphoproliferative response. The suppression of Th1 cells leads to the impaired host response to pathogens and may cause the host more susceptible to the development of tuberculosis [12].
The management of this entity is challenging, as the need for surgical intervention must be assessed thoroughly. The anti-tubercular treatment and albendazole are given simultaneously as per the standard protocols. The renal parenchymal or changes in the ureter due to TB may not be reversible even after chemotherapy. Surgical intervention in the form of excisions like nephrectomy or reconstructive surgery like ureteric reimplantation may be required [13, 14].
In renal hydatid, de-roofing of the cyst is usually done. The cases where the hydatid cavity does not reduce in size with time during postoperative follow-up or presents with pus collection in the residual cavity or does not follow the natural history, one should suspect associated TB, and the patient should be evaluated and investigated for the TB.
In conclusion, co-existence of renal HD and TB is rare, but the awareness of its association is important in managing patients, who are unresponsive to the standard treatment. In both diseases, the diagnosis can be usually delayed because of the non-specific symptoms. Multidrug chemotherapy combined with judicious surgery as and when indicated is the ideal treatment.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: S.S.
Data curation: V.S.
Formal analysis: M.P.
Investigation: S.R.
Methodology: S.S.
Project administration: S.R.
Resources: P.N.
Supervision: S.R.
Validation: M.P.
Visualization: P.N.
Writing - original draft: V.S.
Writing - review & editing: S.S.
1S.R., Ram Samujh; 2S.R., Radhika Srinivasan.
