

Purpose
Anorectal malformations (ARMs) represent a wide spectrum of anomalies with various presentations and associated anomalies. The management of ARMs is still controversial and various managements for ARMs have been proposed. The aim of this study was to identify the status of ARMs in Korea and to analyze the data regarding classification, treatment and functional outcomes of ARMs among the Korean Association of Pediatric Surgeons (KAPS) members.
Methods
The KAPS has conducted a national survey for ARMs in 1999 and 2015 to analyze the differences and changes in the classification, treatment, and functional outcomes of ARMs.
Results
A total of 295 and 619 ARMs patients were enrolled in the second and third national survey, respectively. The most common type among male and female was the low type in the second national survey and low defects (cutaneous fistula, anal stenosis, membrane) in the third national survey. Most common associated anomalies were genitourinary system in the second national survey and cardiovascular system in the third national survey. Various surgical options including anoplasty, posterior sagittal anorectoplasty (PSARP) and laparoscopic surgery with or without colostomy were performed. Unfortunately, comparison regarding functional outcomes between 2 national surveys was not possible due to the use of different classification and functional assessment criteria.
Conclusion
We suggest making an ARMs registry at a national level so that multicenter functional outcome data can be collected for a better understanding and management of this rare anomaly.
Anorectal malformations (ARMs) represent a wide spectrum of anomalies with various presentations and associated anomalies. The management of ARMs is still controversial and various managements for ARMs have been proposed. The aim of this study was to identify the status of ARMs in Korea and to analyze the data regarding classification, treatment and functional outcomes of ARMs among the Korean Association of Pediatric Surgeons (KAPS) members.
The KAPS has conducted a national survey for ARMs in 1999 and 2015 to analyze the differences and changes in the classification, treatment, and functional outcomes of ARMs.
A total of 295 and 619 ARMs patients were enrolled in the second and third national survey, respectively. The most common type among male and female was the low type in the second national survey and low defects (cutaneous fistula, anal stenosis, membrane) in the third national survey. Most common associated anomalies were genitourinary system in the second national survey and cardiovascular system in the third national survey. Various surgical options including anoplasty, posterior sagittal anorectoplasty (PSARP) and laparoscopic surgery with or without colostomy were performed. Unfortunately, comparison regarding functional outcomes between 2 national surveys was not possible due to the use of different classification and functional assessment criteria.
We suggest making an ARMs registry at a national level so that multicenter functional outcome data can be collected for a better understanding and management of this rare anomaly.
Anorectal malformations (ARMs) represent a wide spectrum of anomalies with various presentations and associated anomalies. The classification and operative management of ARMs have been influenced by the extensive work of Alberto Peña [1, 2]. In other western countries, surgical methods have undergone numerous trials and errors over a long period of time for improvement. Since the first description of posterior sagittal anorectoplasty (PSARP) in 1982, this Peña operation has evolved as the standard technique for numerous surgeons worldwide and this operation was also immediately introduced to Korea. Most Korean pediatric surgeons began corrective surgery for ARMs using Peña operation from the beginning. However, there are still controversies in the management of ARMs and various managements for ARMs have been proposed [3, 4]. Constipation and incontinence are major concerns that affect the quality of life of patients. Therefore, many multicenter studies have been conducted to improve the treatment outcome of ARMs [5, 6, 7]. The Korean Association of Pediatric Surgeons (KAPS) also conducted a national survey to members of the KAPS in order to identify the status of ARMs in Korea and to analyze the data regarding classification, treatment and functional outcomes of ARMs among KAPS members.
The KAPS has conducted three national surveys for ARMs so far. Unfortunately, data from the first national survey in 1994 were not available. Therefore, we analyzed the differences and changes in the classification, treatment, and functional outcomes of ARMs based on the national survey data conducted in 1999 and 2015. The second national survey in 1999 was conducted for two years from 1996 to 1997 on 24 members of KAPS working in 22 pediatric surgical centers in Korea [8]. We made the case registration form before the survey which included data regarding gender, gestational age, birth weight, any associated anomalies, type of defect, type of surgery, and functional outcomes. Case registration form was sent to the 24 members of the KAPS. In order to classify the type of ARMs, Wingspread classification was used at the second national survey. The third national survey included patients who had been treated for ARMs from January 2010 to December 2013. We also created the medical questionnaire before the survey to include data regarding gender, gestational age, birth weight, any associated anomalies, type of defect, type of surgery, and functional outcomes. The third national survey using the medical questionnaire was sent to the members of the KAPS and were completed in 17 pediatric surgical centers, including total of 619 patients. Patients who received colostomy at an initial hospital and then transferred to another hospital, or had incomplete or inaccurate data during follow-up were excluded. In the third national survey, Peña classification was used. To evaluate the functional outcomes, the Krickenbeck classification which includes voluntary bowel movements, soiling and constipation was used.
A total of 295 patients were enrolled in the second national survey, comprising of 187 male and 108 female patients. The male to female ratio was 1.7:1. Premature infants under 36 weeks accounted for 1.9%, and low birth weight infants weighing less than 2.6 kg accounted for 12.1%. When considering the frequency of associated anomalies by organ system, there were a total of 54 cases (18.3%) involving the genitourinary system which was the most common anomaly, followed by 42 cases (14.2%) of cardiovascular system, 15 cases (5.1%) of musculoskeletal systems, 13 cases (4.4%) of gastrointestinal system, 12 cases (4.1%) of vertebral anomalies, 11 cases (3.7%) of chromosomal anomalies, and 19 cases (6.4%) of others.
Regarding the type of ARMs in male, the most common type was low type including anocutaneous fistula and anal stenosis, with 88 cases (47.1%). The second most common type was high type including anorectal agenesis and rectal atresia, with 62 cases (33.2%). In female, low type was present in 66 (61.1%) out of 108 cases, being the most common type of defect in female. Intermediate type, such as rectovestibular fistula, rectovaginal fistula, and anal agenesis without fistula was second most common type (27.8%) (Table 1).
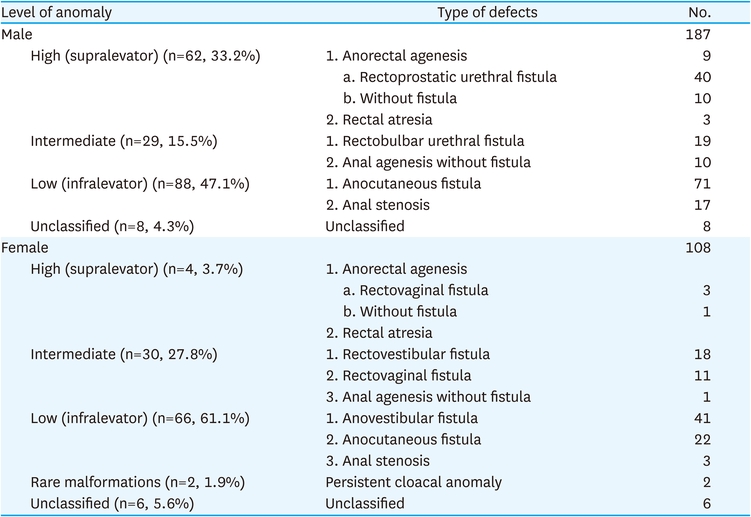
Table 1
Type of defects of ARMs patients in the second national survey
Regarding the operative treatment according to the type of defect in male patients, 58 cases (93.5%) out of 62 high type patients were treated with Peña operation. Twenty-four cases (82.8%) out of 29 intermediate type patients were treated with Peña operation. Sixty-six cases (75.0%) out of 88 low type patients were treated with cutback anoplasty. Regarding the operative treatment according to the type of defect in female patients, 6 cases (100.0%) of cloaca and high type patients were treated with Peña operation. Twenty-six (86.7%) out of 30 cases of intermediate type patients were treated with Peña operation. Sixty-six cases of low type patients were treated with 27 (40.9%) Peña operation, 14 (21.2%) cutback anoplasty, 18 (27.3%) anal transposition and 2 (3.0%) others (Table 2).
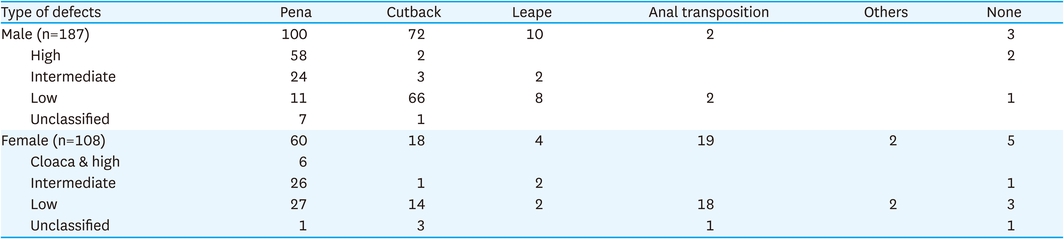
Table 2
Operative treatment according to the type of defects in ARMs patients in the second national survey
The second national survey included three criteria to evaluate the functional outcomes after surgery: anal appearance, constipation, and continence (Table 3). In male patients, as for the shape of the anus, the low type group had the best result with 79 patients (96.3%) having normal appearances. Regarding presence of constipation, 78 patients (94.0%) in the low type group did not have constipation. Defecation control was also normal in 77 patients (98.7%) in the low type group. In female patients, similar to the results in male patients, low type group had the best outcome regarding shape of anus with 58 of the patients (95.1%) having normal appearances. Regarding presence of constipation, 43 patients (76.8%) in the low type group did not have constipation. Defecation control was also normal in 49 patients (87.5%) in the low type group (Table 4).
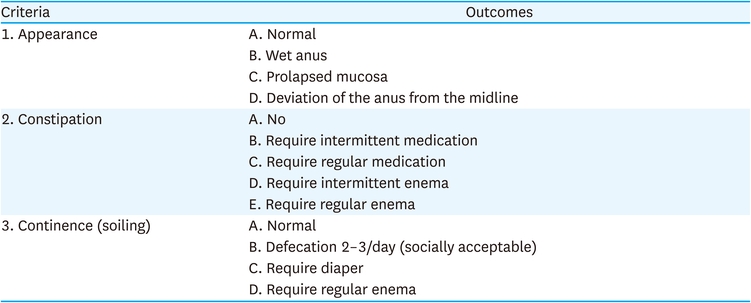
Table 3
Evaluation of functional outcomes after surgery in the second national survey
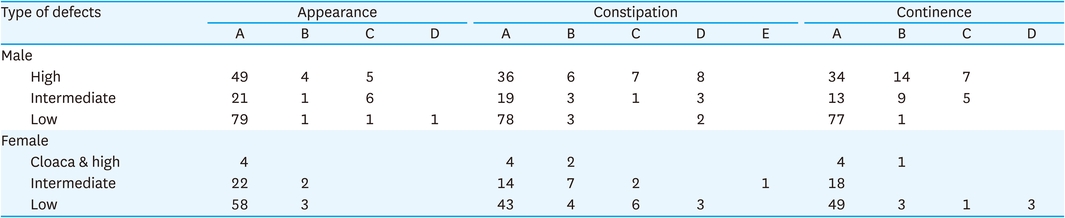
Table 4
Postoperative functional outcomes of ARMs patients in the second national survey
A total of 619 patients were enrolled in the third national survey, with 354 males and 265 females. Male to female ratio was 1.3:1. Mean gestational age was 38 weeks and 1 day. Mean birth weight was 2,933 g. The most frequent organ associated anomaly was cardiovascular system with 261 cases (42.2%), followed by 126 cases (20.4%) of neurologic problems, 125 cases (20.2%) of genitourinary systems, 59 cases (9.5%) of gastrointestinal system, 43 cases (6.9%) of vertebral anomalies, 39 cases (6.3%) of musculoskeletal systems, 17 cases (2.7%) of chromosomal anomalies, and 58 cases (9.4%) of others. In particular, there were 36 cases (5.8%) of esophageal atresia with or without tracheoesophageal fistula, 9 cases (1.5%) of duodenal atresia or web, 4 cases (0.6%) of congenital megacolon, 4 cases (0.6%) of malrotation, and 2 cases (0.3%) of omphalocele.
Regarding the type of ARMs in male, the most common type was low defects with 162 cases, accounting for 45.8%. The second most common type was rectourethral bulbar fistula with 82 cases (23.2%), followed by rectourethral prostatic fistula with 48 cases (13.5%) and rectobladder neck fistula with 30 cases (8.5%). In female, low defects was present in 113 cases (42.6%), which was the most common type of defect in female. Vestibular fistula was present in 103 cases (38.9%), and vaginal fistula was present in 13 patients (4.9%). Persistent cloacas was present in 20 cases (7.6%) (Table 5).
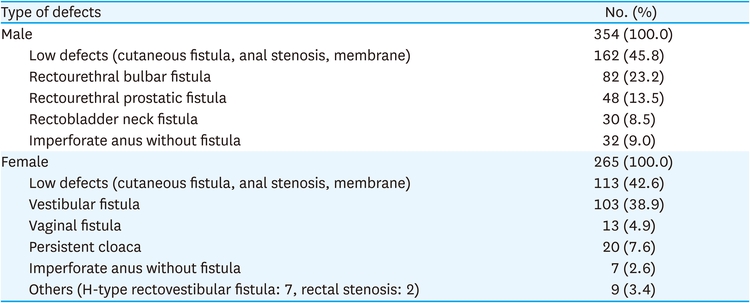
Table 5
Type of defects in the ARMs patients in the third national survey
For the low defects in male patients, 115 cases (71.0%) were treated by Y-V or cutback anoplasty and minimal PSARP was performed in 30 cases (18.5%) (Table 6). In rectourethral bulbar fistula, 65 cases (79.3%) were treated with PSARP with colostomy. Laparoscopic surgery with colostomy was performed in 14 cases (17.1%). In rectourethral prostatic fistula, 37 cases (77.1%) were treated with PSARP with colostomy and PSARP and laparotomy with colostomy was performed in 5 cases (10.4%). In rectobladder neck fistula, 12 cases (40%) were treated with PSARP with colostomy and laparoscopic surgery with colostomy was performed in 10 cases (33.3%) (Table 7).
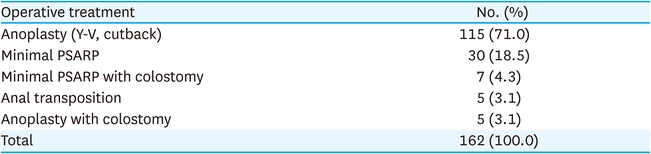
Table 6
Operative treatment for the low defects in male patients in the third national survey
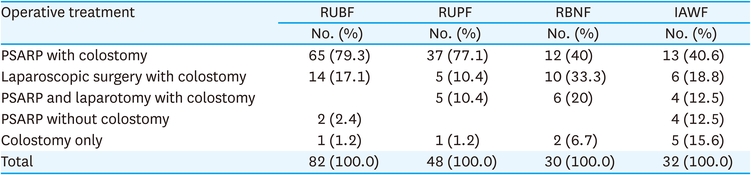
Table 7
Operative treatment for the rectourethral bulbar, rectourethral prostatic, rectobladder neck fistula and imperforate anus without fistula in male patients in the third national survey
For the low defects in female patient, 89 cases (78.8%) were treated with anoplasty and minimal PSARP were performed in 18 cases (15.9%) (Table 8). For vestibular fistula, various surgical options were performed: 41 cases (39.8%) were minimal PSARP with colostomy, 22 cases (21.3%) were minimal PSARP without colostomy, 19 cases (18.4%) were anoplasty, and 12 cases (11.7%) were anoplasty or fistula widening and then minimal PSARP (Table 9). For vaginal fistula, PSARP with colostomy were performed in 6 cases (46.1%) and laparoscopic surgery with colostomy were performed in 5 cases (38.5%). For persistent cloacas, 15 cases (75.0%) were treated with total repair of cloacas with colostomy or ileostomy and 2 cases (10.0%) were performed with colostomy or ileostomy only. Two cases (10.0%) were performed with colostomy or ileostomy with cystostomy (Table 10). Other cases included 7 cases of H-type rectovestibular fistula which were treated with mucosal advancement flap and 2 cases of rectal stenosis which were treated with PSARP with colostomy or pull-through operation with ileostomy.
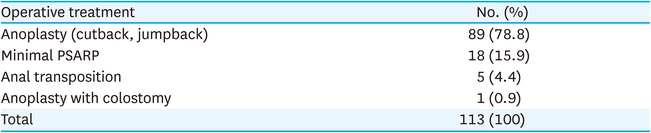
Table 8
Operative treatment for the low defects in female patients in the third national survey
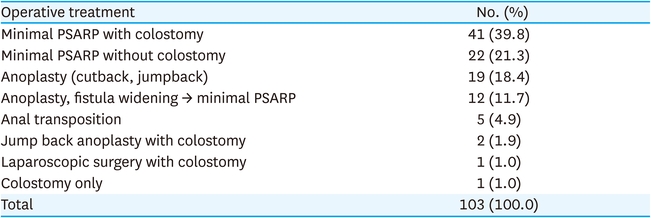
Table 9
Operative treatment for vestibular fistula in female patients in the third national survey
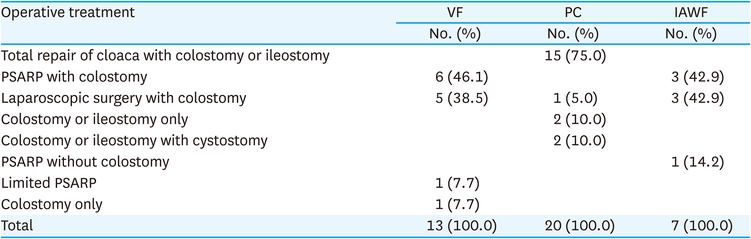
Table 10
Operative treatment for vaginal fistula, persistent cloaca and imperforate anus without fistula in female patients in the third national survey
Regarding the postoperative functional outcomes in male patients, low defects resulted in 94.3% having voluntary bowel movements, 3.8% had soiling, and 27.4% had constipation. However, in rectourethral prostatic fistula, as we could expect, the outcome was poor compared to the low type. 59.6% had voluntary bowel movements, 25.5% had soiling, and 48.9% had constipation. Regarding the postoperative functional outcomes according to the type of defects in female patients, low defects resulted in 95.4% having voluntary bowel movements, 7.3% had soiling, and 21.1% had constipation. For vestibular fistula, 10.3% had soiling, and 43.3% had constipation. For vaginal fistula, 16.7% had soiling, and 66.7% had constipation. For cloacas, 35.7% had soiling, and 42.9% had constipation (Table 11).
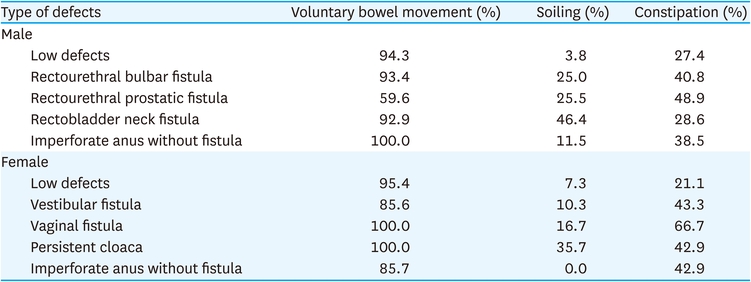
Table 11
Postoperative functional outcomes of ARMs patients in the third national survey
ARMs are relatively common congenital anomaly. However, a clear classification system has not yet been established due to various anatomical and morphological variations. Therefore, comparison of treatment outcomes has been hindered because of confusion relating to classification and assessment systems. In a conference held in Wingspread, USA in 1984, new classification and assessment systems was suggested to facilitate intercommunication and comparison between pediatric surgeons working in the reconstruction of ARMs. The Wingspread classification categorized ARMs into high, intermediate, and low lesions based on the relationship of the terminal rectum with levator ani [3]. However, Wingspread classification also has several problems. Currently, many pediatric surgeons are using the Peña classification system described by Alberto Peña in 1995. Peña classification system is based on the presence and position of the fistula present such as perineal, bulbar, prostatic, bladder neck fistula, vestibular, vaginal fistulas, and cloacal fistulas [2]. An International Conference for the Development of Standards for the Treatment of Anorectal Malformations was held in Krickenbeck Castle, Germany to develop a new international classification for ARMs and a new grouping for follow-up assessment and standard surgical procedures. The Krickenbeck classification system encompasses three categories including diagnostic, surgical procedure, and functional outcome [4].
In our two national surveys of KAPS, the second national survey using Wingspread classification enrolled 295 patients over 2 years. Six hundred nineteen patients were enrolled in the third national survey with Peña classification over 4 years. Although the number of patients per year was similar in the two national surveys, it was difficult to directly compare the demographics and type of defects between two national surveys due to the difference in classifications used. Nevertheless, in the 2 national surveys, the most common type among male and female was the low type in the second national survey, and low defects (cutaneous fistula, anal stenosis, membrane) in the third national survey.
The most common associated anomaly was the genitourinary system in the second national survey and cardiovascular system in the third national survey. A hypothesis why there were many cardiovascular system anomalies in the third national survey is that the medical questionnaire used in the second and third surveys were different, and a significant number of minor heart problems such as small atrial septal defect or patent ductus arteriosus were included in the third national survey. Another explanation is that from 2010 to 2015, when the third national survey was conducted, more aggressive diagnostic work-up for congenital heart disease may have been performed.
Various surgical options such as sacroperineal anorectoplasty, abdominoperineal anorectoplasty have been implemented in repairing the ARMs. Since the first introduction of PSARP in 1982, this operation has evolved as the standard technique for numerous surgeons worldwide. Georgeson et al. reported laparoscopically assisted anorectal pull-through (LAARP) for high imperforate anus in 2000 [9]. Since then, many pediatric surgeons have performed laparoscopic surgery for ARMs and reported the outcomes [10, 11, 12, 13, 14, 15, 16, 17]. In PSARP, the levator ani muscle and external anal sphincter are incised and then the muscle is sutured and wrapped around the pull-through rectum. However, LAARP in children with ARMs may allow direct visualization of the pelvic structure and accurate dissection. In addition, it facilitates identification of the levator ani muscles and the pull-through sites with the use of bipolar myostimulator and then creates a new anus without cutting the levator ani muscle and external anal sphincter. In general, laparoscopic surgery has advantages such as less pain, better cosmetic results, faster return of bowel function, and shorter hospital stay [12]. There is still controversy regarding the clear indication of laparoscopic surgery for various type of ARMs. In the case of rectobladder neck fistula, which occurs in 10% of male patients with ARMs, abdominal approach is required, and therefore, it is an ideal indication for laparoscopic surgery. However, rectourethral prostatic fistula can be repaired either by laparoscopically or PSARP. The choice of surgical method must be made based on the experience of the pediatric surgeon. In all other type of ARMs such as rectoperineal fistula, rectourethral bulbar fistula, ARMs without fistula, and rectovestibular fistula, no clear justification for laparoscopic surgery could be found [12]. Recently, many studies have been published comparing the functional outcomes and complications of conventional PSARP and LAARP in patients with ARMs [11, 12, 13, 14, 15, 16]. Minaev et al. reported that laparoscopic-assisted anorectal pull-through enabled complete correction of ARM without damage to the rectum and anus [11]. Bischoff et al. [12] reported in a review article that standardization and improvement in the quality of reporting is necessary and there was no evidence of better functional results in cases of ARMs operated laparoscopically. Tainaka et al. [13] reported that LAARP was at high risk for mucosal prolapse and posterior urethral diverticulum. Although LAARP did not improve fecal continence in high and intermediate anus, the results of LAARP was comparable to those of PSARP [13]. In our national survey, there was no laparoscopic surgery performed in the second national survey in 1999. However, in the third national survey, laparoscopic surgery was performed in 45 (7.3%) out of 619 ARMs patients in KAPS during the 4 years. Among them, laparoscopic surgery with colostomy was performed in 33.3% of patients with rectobladder neck fistula. There were various surgical options for vestibular fistula in female at the third national survey; 1) 3 stages operation including colostomy, PSARP, and colostomy repair, 2) 1-stage PSARP without colostomy, 3) perineal operation with anoplasty or fistula transposition. Our suggestion is to choose the surgical option depending on the surgeon’s preference and patient’s general condition.
In addition to the functional outcomes, the psychosocial aspect and quality of life (QOL) are very important issues in the long-term management of patients with ARMs. Recently, long-term studies have been published to analyze the QOL of patients with ARMs [15, 18]. Wong et al. [15] reported that the QOL scores based on the Hirschsprung disease/Anorectal Malformation Quality of Life (HAQL) questionnaire were comparable between the LAARP and PSARP in all areas except social functioning. Unfortunately, it was not possible to directly compare the two national survey groups regarding functional outcomes because the assessment criteria were different in our two national surveys. There is also limitation of these national survey that the follow-up period is too short to fully evaluate the postoperative functional outcomes of ARM patients. This needs to be considered in the future for a more reliable results. In order to collect accurate patient data, it is important to decide in advance which classification method and functional outcome assessment to use through a KAPS meeting.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
