

In patients with Langerhans cell histiocytosis (LCH), it is possible for other malignancies to develop. In the majority of cases, these are lymphomas and leukemia; however, in some cases solid tumors such as lung carcinomas may exist concurrently or can develop after chemotherapy. We want to introduce a rare solid tumor that can be found during LCH treatment. A 4-year old boy who was treated for 15 months with chemotherapy for LCH. The mass was noted on a follow-up abdominal ultrasonography. He underwent an abdominal mass excision and it was confirmed as a ganglioneuroblastoma. Coexistence of malignant neoplasms with LCH is currently being studied but is not yet well understood. In this case report, ganglioneuroblastoma appeared after chemotherapy for LCH. Whether this solid tumor developed as a result of chemotherapy or was formed due to the inflammatory response of LCH is still controversial.
In patients with Langerhans cell histiocytosis (LCH), it is possible for other malignancies to develop. In the majority of cases, these are lymphomas and leukemia; however, in some cases solid tumors such as lung carcinomas may exist concurrently or can develop after chemotherapy. We want to introduce a rare solid tumor that can be found during LCH treatment. A 4-year old boy who was treated for 15 months with chemotherapy for LCH. The mass was noted on a follow-up abdominal ultrasonography. He underwent an abdominal mass excision and it was confirmed as a ganglioneuroblastoma. Coexistence of malignant neoplasms with LCH is currently being studied but is not yet well understood. In this case report, ganglioneuroblastoma appeared after chemotherapy for LCH. Whether this solid tumor developed as a result of chemotherapy or was formed due to the inflammatory response of LCH is still controversial.
The pathogenesis of Langerhans cell histiocytosis (LCH) is not well established. Research is ongoing to determine whether this disorder is neoplastic or is caused by an inflammatory response [1]. In addition, the association of LCH with other malignancies is not fully understood. Egeler et al. [2] reported that a large number of LCH patients had associated malignant lymphoma, leukemia, lung carcinoma, and other solid tumors. Until now, there have been few reports on the coexistence of neuroblastoma detected when patients are diagnosed with LCH or the appearance of neuroblastoma following chemotherapy for LCH [3, 4, 5]. Here, we introduce a case study of a child with LCH who was diagnosed with ganglioneuroblastoma after several months of chemotherapy.
A 4-year-old boy was referred to the department of pediatric surgery at Seoul National University Children's Hospital due to an abdominal mass found on an abdominal ultrasound. He was previously diagnosed with LCH on his right humerus (Fig. 1). At the first diagnosis, the child reported arm pain and fever which had persisted for a month. He was treated at another hospital with chemotherapy, comprising vinblastine and prednisone, from March 2018 to June 2019. The child underwent follow-up, which involved monthly radiography of his humerus and bone scans every 3 months. After staring of 15 months chemotherapy, a routine abdominal ultrasound was performed to potentially identify any new lesions in the abdomen. On the imaging taken on May 31, 2019, an abdominal mass was detected, and ultrasound-guided biopsy was performed. Pathology results initially suggested that the mass was ganglioneuroma. The child showed no specific symptoms, such as abdominal discomfort, at the time of the ultrasound. The patients' neuron-specific enolase level was 21.38 ng/mL (normal range: 0–16.3 ng/mL) and ferritin level was 9 ng/mL (normal range: 16–400 ng/mL).
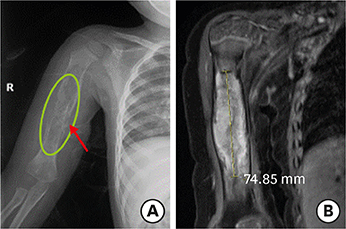
Fig. 1
Right humerus X-ray (A) and upper arm MRI (B). The X-ray shows an osteolytic lesion on the right humerus with a lamellated periosteal reaction (A). MRI of the right upper arm shows a 7.5×1.4×1.5 cm enhancing osteolytic mass replacing right humerus diaphysis with extensive soft tissue edema (B). This lesion was diagnosed with Langerhans cell histiocytosis by ultrasound-guided biopsy.
MRI, magnetic resonance imaging.
For more detailed examination, magnetic resonance imaging (MRI) was taken. An arterial T1-weighted MRI showed a lobulated mass measuring 3.6×3.8 cm, with high signal intensity, in the right suprarenal area (Fig. 2). Positron emission tomography (PET)-computed tomography (CT) showed hypermetabolism in the right adrenal gland and suggested the need to clarify whether this is a metastatic lesion at the anterior aspect of right psoas muscle (Fig. 3).
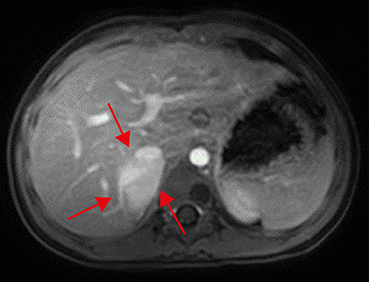
Fig. 2
Abdominal magnetic resonance imaging. An arterial-phase imaging shows enhancing lobulated mass (multiple red arrows) in the right suprarenal area, displacing intrahepatic inferior vena cava anteriorly and suspicious of the invasion of right hepatic lobe.
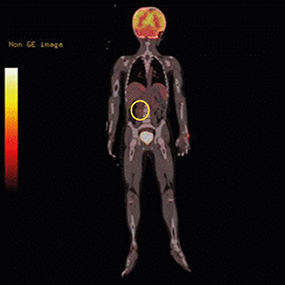
Fig. 3
Positron emission tomography-computed tomography. The round circle indicates a hypermetabolic lesion on the right psoas muscle. This lesion was suspicious of metastasis of ganglioneuroblastoma. Multi-disciplinary teams discussed the lesion and concluded that metastasis was not definite.
Abdominal-pelvic CT was performed on July 18, 2019, and it showed a low attenuated, ill-defined mass on the right adrenal gland, indicating a probable neurogenic tumor (Fig. 4). In addition, a metastatic lymph node (LN) along the anterior part of the right psoas muscle appeared suspicious. Multi-disciplinary teams discussed whether the anterior aspect of right the psoas muscle was a true metastatic lesion and made the decision to undergo an operation.
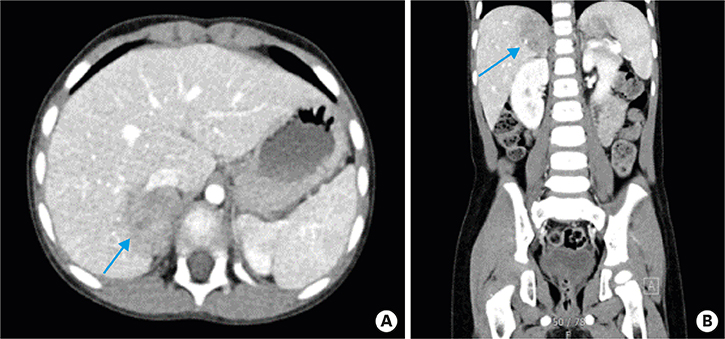
Fig. 4
Abdominal-pelvis computed tomography. An arterial phased axial view (A) and coronal view (B). The blue arrows show a low attenuated lobulated mass and tiny calcification at the medial portion.
The patient underwent surgery for excision of the lesion. We had initially planned a laparoscopic right adrenalectomy (Fig. 5); however, the tumor was located at the rear of the liver. Thus, poor accessibility was anticipated, and the surgical team decide to change into open method. The abdominal tumor was fully excised, including a small part of the posterior section of the liver. The gray-whitish solid tumor measured 4.0×3.8×2.2 cm. No signs of necrosis or hemorrhage were observed. The pathology results revealed ganglioneuroblastoma, both nodular and intermixed. N-myc gene amplification study was additionally performed.
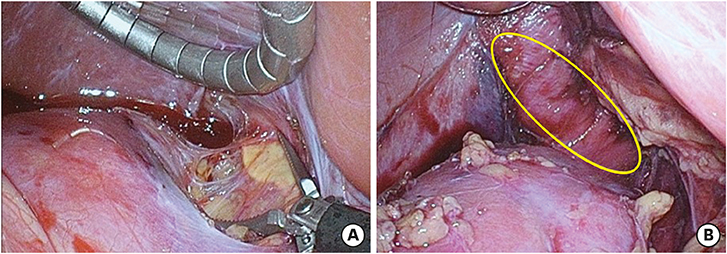
Fig. 5
Laparoscopic view during operation. Laparoscopic dissection of mass surrounding tissues on the right kidney (A). Laparoscopic view of the right adrenal mass (B).
The patient was discharged on postoperative 6 day after surgery without any complications. Due to the N-myc result being negative, ganglioneuroblastoma was defined as stage I. Thereafter, continuation of chemotherapy for LCH was planned at the outside hospital where he had previously received treatment. Whether the LN along the anterior aspect of the psoas muscle was metastatic was not determined, therefore a follow-up PET-CT and abdominal MRI were planned.
The association of LCH with malignant neoplasms is not clearly understood. Egeler et al. [2] reviewed several cases of LCH with leukemia or other solid tumors. The types of solid tumor reported vary; however, most of them (12 cases of 30) are lung carcinomas and one case of each of the following has been reported: osteosarcoma, astrocytoma, glioblastoma, medulloblastoma, and meningioma. In that report, the time of diagnosis of the solid tumors differed in each case. In cases of lung carcinoma (12 cases), 75% (9 cases) were diagnosed simultaneously with LCH. However, in cases of the other solid tumors (18 cases), 78% (14 cases) were diagnosed after treatment of LCH. Conversely, Rayburg et al. [6], reported a case of a neuroblastoma patient in phase I of treatment being diagnosed with an LCH related bone lesion.
In this case report, LCH preceded the diagnosis of ganglioneuroblastoma. The LCH was initially confined to a bone lesion and was not disseminated. After 15 months of chemotherapy, new lesion development was confirmed. The lesion was located in the right adrenal gland and was adherent to the posterior section of the liver. The fully excised mass was confirmed as a ganglioneuroblastoma. Ganglioneuroblastoma is a rare malignancy, which occurred in this patient during the treatment of LCH. Considering that this neoplasm was diagnosed after 15 months of starting chemotherapy and routine imaging, the newly developed tumor may be a result of the chemotherapy.
The child suffered from a single bone lesion (localized on the humerus); however, due to its large size, the lesion was unsuitable for curettage or radiation therapy. In addition, for the functional preservation of the upper arm, we deemed it better to administer 12 months of systemic chemotherapy. The regimen consisted of vinblastine and prednisone. Other regimens such as cladribine or a combination of vincristine and cytosine arabinoside can also be used for multisystem LCH treatment. We prescribed vinblastine for the treatment of LCH in our case and this is renowned for neuroblastoma treatment along with rapamycin [7]. It is therefore interesting whether this ganglioneuroblastoma was a chemotherapy related malignancy or part of the inflammatory response of LCH [1]. As observed in our case, follow-up imaging at least every 1 year is necessary to determine recurrence or development of other malignancies in the treatment of LCH. Also, according to the staging of newly developed neoplasms, chemotherapy may be an additional or omitted treatment strategy. Further understanding of the pathogenesis is necessary, and the natural history of LCH should be studied to ensure proper treatment to help improve outcomes.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H.Y.
Data curation: H.I.
Formal analysis: H.I.
Funding acquisition: H.J.W.
Investigation: B.J.
Methodology: B.J.
Project administration: K.H.Y.
Resources: K.H.Y.
Supervision: H.J.W.
Validation: H.J.W.
Visualization: B.J.
Writing - original draft: H.I.
Writing - review & editing: H.I.
