

Intussusception recurs in 10% to 20% of childhood intussusception after successful nonoperative reduction. Multiple recurrences of intussusception are associated with the presence of a pathologic lead point. We describe a case of a 9-month-old boy with 4 times recurrent intussusception after nonoperative reduction caused by diffuse large B cell lymphoma lesion of the ileum. Clinical suspicion and surgical approach is needed to find rare cause of recurrent intussusception.
Intussusception recurs in 10% to 20% of childhood intussusception after successful nonoperative reduction. Multiple recurrences of intussusception are associated with the presence of a pathologic lead point. We describe a case of a 9-month-old boy with 4 times recurrent intussusception after nonoperative reduction caused by diffuse large B cell lymphoma lesion of the ileum. Clinical suspicion and surgical approach is needed to find rare cause of recurrent intussusception.
Intussusception is the most common abdominal emergency in early childhood, particularly in children younger than 2 years of age. In approximately 25% cases of childhood intussusception, an underlying disease causes a pathologic lead point for the intussusception [1]. A lead point is a lesion in the intestine that is trapped by peristalsis and dragged into a distal part of the intestine, causing intussusception. Recurrence is not necessarily an indication for surgery. But imaging studies should be reviewed carefully for the possibility of a pathologic lead point. The suspicion of an intestinal intussusception with a pathological lesion at the lead point necessitates a surgery. In this case report, we present a case of a 9-month-old boy who had recurrent ileocolic intussusception on diffuse large B cell lymphoma lesion of the ileum.
A 9-month-old male who was previous healthy came to the emergency room with complaints of bloody stools occurring in the evening of the previous day and the next morning, followed by vomiting. Abdominal ultrasonography was performed at another hospital. It showed suspicious findings for intussusception. The patient appeared more irritable than usual. He had bloody stools resembling red currant jelly. The patient was hemodynamically stable. On physical examination, his abdomen was not distended and the tenderness was not evident. Bowel sounds were slightly decreased on auscultation. Laboratory test results are shown in Table 1. Abdominal ultrasonography revealed ileocolic type intussusception with a size of about 1.8 cm in the right abdomen. There were mesenteric fat and enlarged lymph nodes inside. However, no mass or lead point was seen inside the intussusception. Doppler examination confirmed adequate blood flow inside the intestine. Fluoro-guided pneumatic reduction was successfully performed and the patient was hospitalized to monitor the progress.
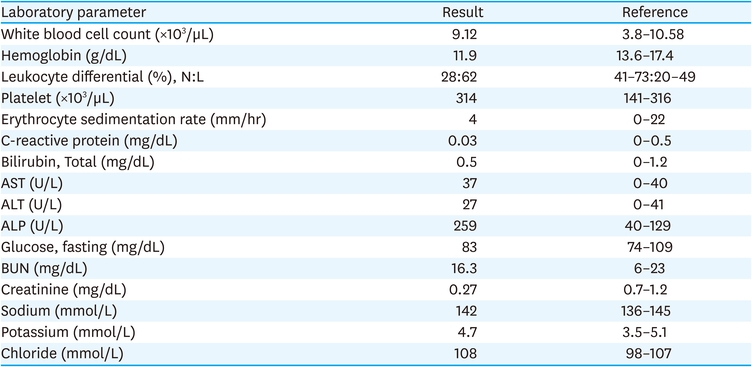
Table 1
Laboratory findings at presentation
On the first day of hospitalization, formula feeding was started. There were no symptoms after the diet progressed. On the second day of admission, the patient became irritable and bloody stools recurred. Ultrasonography showed recurrence of intussusception and a second air reduction was performed. After successful decompression, the patient had a follow-up ultrasound the next day. On ultrasonography, ileocolic intussusception was re-developed in the right abdomen and 1.4 cm long low echoic focal eccentric wall thickening was observed in the distal part of intussuscipiens (Fig. 1A). This was the lesion thought to be the lead point. A third air reduction was performed for recurrent intussusception. After the patient was stabilized, abdominal computed tomography (CT) was performed to evaluate the lesion suspected as a lead point on ultrasound. On CT scan, the lesion appeared to be in the form of focal enhancing wall thickening with recurred ileocolic intussusception (Fig. 1B). There were no findings suggestive of Meckel's diverticulum or duplication cyst. The patient was diagnosed with intussusception with a lead point. The patient underwent exploratory laparoscopy. Laparoscopic reduction of intestine was performed for findings of intussusception. We used 3 mm laparoscopic instruments during surgical reduction of intussusception. Two graspers were mainly utilized during the procedure. We grasped the proximal ileum and cecum with laparoscopic graspers and gently pulled both ends apart. Care was taken not to injure the bowel during the procedure, both at the point where the bowels were grasped and around the intussusceptum. The serosal surface of the terminal ileum showed a dimpling spot and vague surrounding irregularity after successful reduction. Also, firmness of the bowel surrounding the dimpling spot was felt through the laparoscopic instruments. It was fairly obvious that there was a mass lesion within (Fig. 2A). In the intra-lumen of ileum, there was a solid, immobile mass-like lesion of 1 cm in size with central ulceration (Fig. 2B). The umbilical incision was extended craniocaudally and a wound protector was applied. The cecum and terminal ileum were mobilized and externalized through the umbilical incision. A firm, fixed mass was felt on the ileum wall 5 cm proximal to the ileoceceal valve and 4 cm segment of the surrounding ileum was resected. The ileal ends were anastomosed in end-to-end fashion with interrupted running sutures. The patient recovered without complications. He was discharged on the sixth day after surgery. Histopathological examination of the lesion revealed features of diffuse large B-cell lymphoma (Fig. 2C and D). We referred the patient to the Department of Pediatric Oncology for evaluation and initiation of chemotherapy treatment. This disease was classified as stage II germinal center B-cell like diffuse large B cell lymphoma. Patients and parents showed good adherence to treatment and followed recommendations of the oncologist.
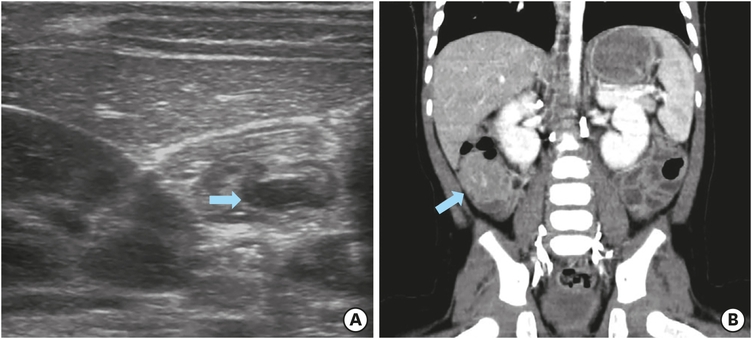
Fig. 1
Ultrasonography and abdominal computed tomography findings for a 9-month-old boy, who was demonstrated to have recurrent intussusception: (A) Ultrasonography revealing recurred ileocolic intussusception with a lead point, an eccentric low echoic thickening (arrow) in the distal part of intussuscipiens. (B) Coronal abdominal computed tomography showing a focal enhancing wall thickening with recurred ileocolic intussusception (arrow). This focal enhancing lesion was thought to be the lead point.
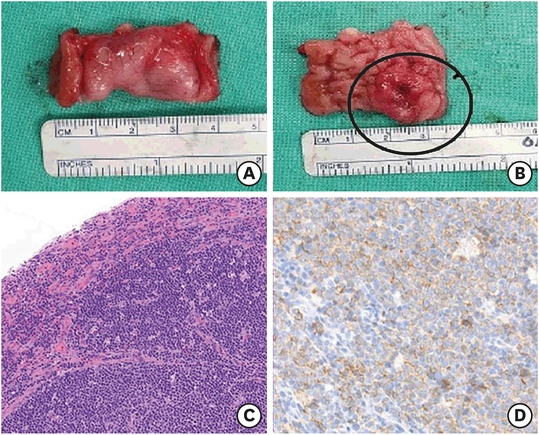
Fig. 2
Gross and histopathological examination of the surgical specimen: (A) The serosal surface of the resected terminal ileum showed a dimpling spot and vague surrounding irregularity. The bowel surrounding the dimpling spot was firm. (B) A solid, immobile mass-like lesion (circle) of 1 cm in size with central ulceration in the intra-lumen of ileum was found. This lesion was thought to be the lead point trapped by peristalsis and dragged into a distal part of the intestine, causing intussusception. (C) The mass showed diffuse cellular infiltrates in mucosa and submucosa of small intestine. Atypical tumor cells were singly dispersed an, bearing large round nuclei with prominent nucleoli. (×40 hematoxylin and eosin stain). (D) Large atypical cells were identified as CD20+ mature B cells (×100 CD20). Results of other immunohistochemical staining were as follows: CD3−, Bcl-2−, MUM1+, CD10+, Bcl-6+, c-myc−, and high proliferation index (Ki-67: 90%). Based on these histological features and immunophenotypes, a diagnosis of diffuse large B-cell lymphoma was made.
This study was approved by the Institutional Review Board (IRB) of the Samsung Medical Center (IRB file No. SMC 2021-07-184).
The clinical triad described for intussusception consists of abdominal pain, red currant jelly stools, and a palpable abdominal mass. A typical symptom of intussusception is a sudden onset of intermittent, crampy, and progressive abdominal pain accompanied by inconsolable crying with legs pulling toward the abdomen [2]. Such episodes usually occur at 15- to 20-minute intervals. Shortly after the first episode of abdominal pain, nonbilious vomiting often starts. However, emesis often becomes bilious as the obstruction progresses. Bloody stool occurs grossly in up to 50% of cases. An additional 25% of cases have occult blood [3]. The bloody stool might be a mixture of blood and mucous that looks like currant jelly. Sometimes, a sausage-shaped abdominal mass may be felt in the right side of the abdomen. However, the typically described triad of pain, currant jelly stool, and a palpable abdominal mass is seen in less than 15% of cases at the time of presentation [4]. Up to 20% of young infants have no apparent pain and about one-third of patients do not pass blood or mucus, nor do they develop an abdominal mass. Occasionally, the initial presenting symptom is lethargy or altered consciousness alone [5]. This clinical presentation is often confused with sepsis in infants. Thus, intussusception should be considered as a differential diagnosis even in the absence of typical symptoms.
Ultrasonography is the method of choice to diagnose intussusception. Reported sensitivity and specificity of this technique approach are 100% in the hands of an experienced ultrasonographer [6]. The classic manifestation of intussusception on ultrasound is a "target sign", representing layers of the intestine within the intestine. Color doppler imaging may reveal insufficient perfusion in the intussusceptum indicating ischemia. Ultrasonography can diagnose a rare ileo-ileal intussusception and identify the lead point of intussusception in approximately two-thirds of cases with underlying pathology [7]. An intussusception can be recognized on CT. CT generally is reserved for patients when other imaging modalities are unrevealing, or to evaluate pathologic lead points for intussusceptions detected by ultrasound [8].
Intussusception recurs in 10% to 20% of children after successful nonoperative reduction [9, 10]. About half of recurrences occur within the first 72 hours after reduction. Residual bowel edema and inflammation might act as lead points [9]. Recurrence is not necessarily an indication for surgery. In general, each recurrence should be managed as if it were the first episode, provided that each attempt at nonoperative reduction is successful and the patient remains stable [10]. However, imaging studies should be reviewed carefully to evaluate the possibility of a pathologic lead point. Multiple recurrences of intussusception are associated with the presence of a pathologic lead point. In one series, 19% of children with 2 or more episodes of intussusception had a pathologic lead point, whereas 4% of children without a recurrence had a pathologic lead point [8].
In approximately 25% cases of childhood intussusception, an underlying disease causes a pathologic lead point for the intussusception [1]. A lead point is a lesion in the intestine that is trapped by peristalsis and dragged into a distal part of the intestine, causing intussusception. Meckel diverticulum, polyps, duplication cysts, lymphomas, areas of reactive lymphoid hyperplasia, and other focal abnormalities of the intestine can act as lead points. Meckel diverticulum is the most common pathologic lead point in most case series in children, followed by polyps, and then either duplication cysts or immunoglobulin A vasculitis [8].
The suspicion of intussusception with a pathological lesion at the lead point necessitates surgery. Laparotomy is the gold standard in both diagnosis and treatment. Pathologic lead point accounts for a greater proportion of cases of intussusception in children younger than 3 months or older than 5 years [8]. Nonetheless, it is important to be vigilant for pathologic lead points in children of any age.
In conclusion, physician should review imaging study carefully for the possibility of a pathologic lead point in case of recurrent intussusception. The suspicion of an intestinal intussusception with a pathological lesion at the lead point necessitates a surgery. Clinical suspicion and surgical approach are warranted to find rare causes of recurrent intussusception.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.M.J.
Data curation: J.T.J., K.E.S., A.S., K.Y.
Supervision: K.M.J., L.S., C.Y.H.
Writing - original draft: J.T.J.
Writing - review & editing: K.M.J., K.E.S.
