

Jejunoileal atresia (JIA) is a rare congenital disorder in newborns leading to intestinal obstruction, necessitating urgent surgery. A delay in diagnosis can result in severe complications like sepsis, bowel perforation, and even death. Over the years, improvements in neonatal care, surgical techniques, and nutrition have led to a marked decrease in mortality rates for JIA patients. While the exact cause remains uncertain, it is thought to result from an ischemic insult during later in utero. JIA is categorized into 4 types, detailing the structure and implications of each type. Clinically, mothers may exhibit polyhydramnios, and infants usually present with symptoms like bilious vomiting and abdominal distension. A significant percentage of affected infants do not pass meconium within the first day of life. Diagnosis is commonly through abdominal radiographs, with some cases requiring contrast enemas. Once diagnosed, immediate surgery is advised, with the primary goal to restore intestinal function and length. Nowadays, the survival rate for JIA patients exceeds 90%. This improvement is attributed to a better understanding of the condition, advancements in surgical techniques, and the introduction of total parenteral nutrition. The prognosis varies, with short bowel syndrome being a significant factor determining the outcome. Short bowel syndrome’s prognosis depends on the remaining small bowel length, the ileocecal valve’s presence, and dependence on long-term nutrition. In conclusion, the treatment and prognosis for JIA have seen substantial improvements due to advances in medical care. Early diagnosis and intervention are crucial. While many patients lead a normal life, those with complications like short bowel syndrome may require long-term care. Future efforts should emphasize refining surgical techniques, gaining a deeper understanding of JIA, and enhancing postoperative care. There's also a need for more research into JIA’s genetics and etiology.
Jejunoileal atresia (JIA) is a rare congenital disorder in newborns leading to intestinal obstruction, necessitating urgent surgery. A delay in diagnosis can result in severe complications like sepsis, bowel perforation, and even death. Over the years, improvements in neonatal care, surgical techniques, and nutrition have led to a marked decrease in mortality rates for JIA patients. While the exact cause remains uncertain, it is thought to result from an ischemic insult during later in utero. JIA is categorized into 4 types, detailing the structure and implications of each type. Clinically, mothers may exhibit polyhydramnios, and infants usually present with symptoms like bilious vomiting and abdominal distension. A significant percentage of affected infants do not pass meconium within the first day of life. Diagnosis is commonly through abdominal radiographs, with some cases requiring contrast enemas. Once diagnosed, immediate surgery is advised, with the primary goal to restore intestinal function and length. Nowadays, the survival rate for JIA patients exceeds 90%. This improvement is attributed to a better understanding of the condition, advancements in surgical techniques, and the introduction of total parenteral nutrition. The prognosis varies, with short bowel syndrome being a significant factor determining the outcome. Short bowel syndrome’s prognosis depends on the remaining small bowel length, the ileocecal valve’s presence, and dependence on long-term nutrition. In conclusion, the treatment and prognosis for JIA have seen substantial improvements due to advances in medical care. Early diagnosis and intervention are crucial. While many patients lead a normal life, those with complications like short bowel syndrome may require long-term care. Future efforts should emphasize refining surgical techniques, gaining a deeper understanding of JIA, and enhancing postoperative care. There's also a need for more research into JIA’s genetics and etiology.
Jejunoileal atresia (JIA) is a rare congenital disorder causing intestinal obstruction in newborns, necessitating emergency surgery. Although JIA typically presents with characteristic symptoms and radiologic features, a delayed diagnosis can lead to complications, including bowel perforation, sepsis, and even death. Over recent decades, care for JIA patients has improved markedly, resulting in a significant decrease in mortality due to advancements in neonatal intensive care, surgical techniques, the use of total parenteral nutrition, and progress in neonatal anesthesia. This article offers a contemporary review of JIA.
JIA occurs in approximately 1–3 out of every 10,000 live births. The gender ratio between males and females is roughly equal, and about one-third of these patients are known to be premature [1]. The site of occurrence for JIA between the jejunum and ileum is similar [2]. In South Korea, based on data from the national healthcare insurance service database from 2013 to 2017 on JIA surgical cords and the number of births, the prevalence is estimated to be about 2.5 per 10,000 live births [3]. According to a survey conducted in 2010 by the Korean Association of Pediatric Surgeons (KAPS), 146 cases of JIA were reported in South Korea between 2007–2009. Of these, 65 cases (44.5%) were jejunal atresia and 81 (55.5%) were ileal atresia. The male to female ratio was approximately 1.3:1, with males being slightly more common, and the preterm rate was 44.8% [4].
The pathogenesis of JIA has been researched extensively, but the precise mechanisms remain elusive. Here is a brief overview of the prevailing theories on its pathogenesis.
This is the most widely accepted theory. It suggests that an intrauterine vascular accident causes ischemia (lack of blood flow) to a segment of the fetal intestine. This ischemia leads to the resorption of the affected segment, resulting in an atresia [5, 6]. Potential causes for this ischemic insult include intussusception, perforation, volvulus, intestinal strangulation, transmesenteric internal hernias, or thromboembolism.
While most cases of JIA are sporadic, some families have reported multiple affected members, suggesting a possible genetic predisposition. There is a well-documented autosomal recessive pattern of inheritance for multiple atresia, which is often found due to mutations in the tetratricopeptide repeat domain-7A (TTC7A) gene, predominantly among French Canadians [7].
There are studies that hint at maternal factors, such as certain infections or drug use during pregnancy, potentially increasing the risk of developing JIA in the fetus. Maternal smoking and cocaine use are known to be associated with neonatal intestinal atresia. Also, maternal use of pseudoephedrine, a common decongestant, has been linked to a higher risk of small bowel atresia in some research. However, the correlation is not definitively established of pseudoephedrine [8].
In JIA, associated extra-abdominal organ abnormalities are less than 10%. This is because JIA occurs in the later stages of fetal development and also because the nature of the vascular insult is localized [9]. Associated congenital anomalies are rarer with JIA than with duodenal atresia. Trisomy 21 is found in about 30% of duodenal atresia patients but is rare in JIA. The most common congenital co-morbidities are cystic fibrosis, malrotation, and gastroschisis, occurring in about 10% of cases [10]. According to the 2010 KAPS survey, the anomalies that accompanied were congenital heart disease at 8.6%, gastrointestinal anomalies at 7.5%, and genitourinary anomalies at 4.8% [4].
The most widely used classification for JIA was revised by Grosfeld. This classification emphasizes the importance of the loss of intestinal length, the abnormal collateral intestinal blood supply, and the concomitant atresia or stenosis, thus having significant prognostic and therapeutic value (Table 1) [11, 12].
• Type I: An internal membrane composed of mucosa and submucosa with continuity in the proximal and distal muscle layers, with no mesenteric defect (Fig. 1).
• Type II: The intestine is discontinuous but without a mesenteric defect.
• Type III: This has two subtypes.
• Type IIIa: The intestine is discontinuous with a V-shaped mesenteric defect (Fig. 2).
• Type IIIb: The intestine is discontinuous, with a broad mesenteric defect, making it look like it is wrapping around a single artery, resembling a Christmas tree or apple peel (Fig. 3).
• Type IV: Multiple-segment atresia, giving a string of sausage appearance (Fig. 4).
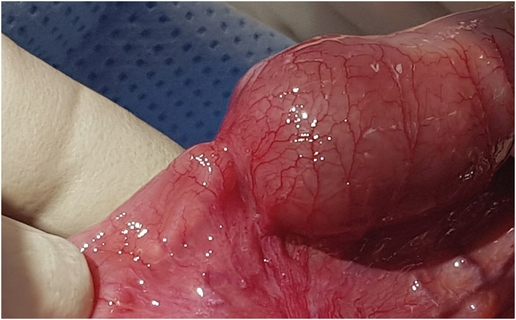
Fig. 1
Type I mucosal atresia. The bowel and its mesentery appear to be in continuity.
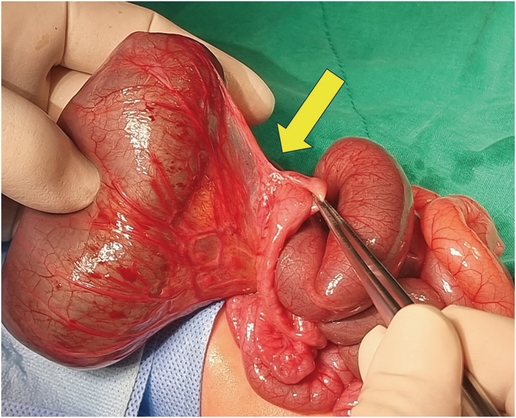
Fig. 2
Type IIIa atresia. Each blind end of the intestine is separated by a V-shaped mesenteric defect (yellow arrow).
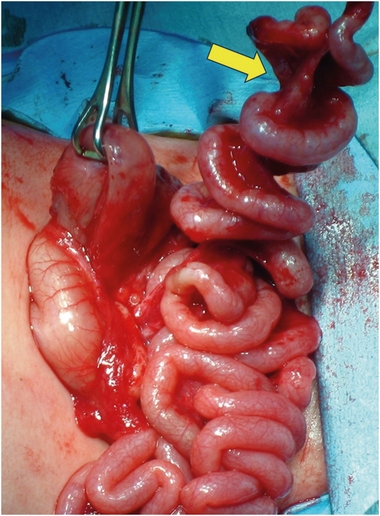
Fig. 3
Type IIIb Christmas tree or apple-peel atresia. Presents with a proximal jejunal atresia with a large mesenteric defect. The distal bowel (yellow arrow) has a single, insecure blood supply.
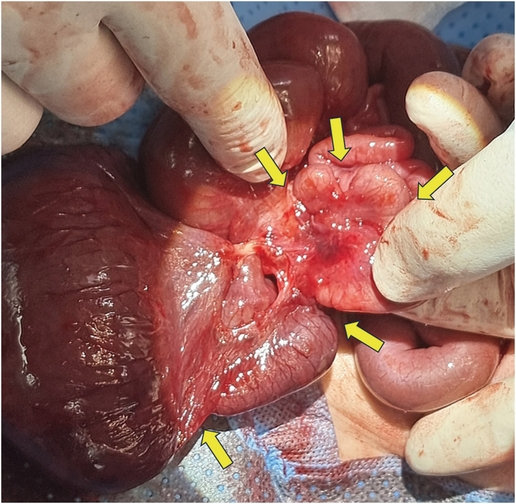
Fig. 4
Type IV multiple atresia (yellow arrows).

Table 1
Classification of jejunoileal atresia
The incidence of each type varies slightly over time and researcher. Applying the current classification to a study of 559 patients published in 1969 by DeLorimier et al. [13], type I was 19%, type II 31%, and type IIIa 46% (at the time, the concepts of type IIIb and IV were absent). In a study of 128 patients published by Dalla Vecchia et al. [10] in 1998, the incidences were type I 23%, type II 27%, type IIIa 18%, type IIIb 7%, and type IV 24%. A study from Japan in 1998 reported on 88 patients: type I 26%, type II or IIIa 56%, type IIIb 8%, and type IV 10% [14]. In the 2010 KAPS survey on 145 patients, the incidences were type I 23.4%, type II 17.9%, type IIIa 38%, type IIIb 6.9%, and type IV 10.3% [4].
JIA occurs similarly in the jejunum (51%) and the ileum (49%) [2]. In more detail, it is known to occur in the proximal jejunum 31%, distal jejunum 20%, proximal ileum 13%, and distal ileum 36% [13]. Most are single atresia (>90%), while multiple atresia occur in 6%–20% of all JIA cases [11, 15]. Type IIIb occurs in 11%–32.4% of JIA cases [16, 17].
Polyhydramnios in the mother is more commonly observed in cases of proximal jejunal atresia (38%) [13]. Typical symptoms in JIA patients are bilious vomiting and abdominal distension. Bilious vomiting is more common in jejunal atresia (84%), while abdominal distension appears more pronounced in ileal atresia (98%). Most patients do not pass meconium within 24 hours of birth, but either meconium or necrotic tissue is occasionally passed [18].
Prenatal ultrasound (US) diagnosis of JIA is limited and does not affect neonatal outcomes in patients with intestinal atresia [19]. This is primarily because US findings, including dilated, echogenic bowel loops and polyhydramnios, are visible mostly only in the later stages of pregnancy. According to one study, only 31% of patients were diagnosed with JIA through prenatal US [20]. However, the prenatal diagnosis rate according to the 2010 KAPS survey was 84.6% for jejunal atresia and 50.6% for ileal atresia [4].
In a normally active neonate, the swallowed air usually reaches the proximal bowel within an hour and the distal small bowel within three hours [21]. In most cases, plain abdominal radiographs (supine and lateral view) demonstrate the presence of intestinal obstruction in patients. Proximal jejunal atresia may present as only a small amount of air-fluid level in the proximal dilated bowel and a gasless abdomen beyond the atresia. The more distal the atresia, the more severe the abdominal distension, with more distended bowel loops and air-fluid levels. In ileal atresia, the bowel just proximal to the atresia is much more dilated and may show more air-fluid levels, which may require differential diagnosis with meconium ileus or total colonic aganglionosis. In these cases, a contrast enema can be helpful (Fig. 5) [22]. In 12% of JIA, plain radiographs show peritoneal calcification, indicating meconium peritonitis [23]. The giant cystic meconium peritonitis is associated with late intrauterine bowel perforation, where the perforated intestine and meconium form an encapsulated mass (pseudocyst) (Fig. 6) [24]. In a survey by KAPS in 2010, meconium peritonitis was reported in 22.1% of JIA (12.5% in jejunal atresia and 31.5% in ileal atresia) [4].
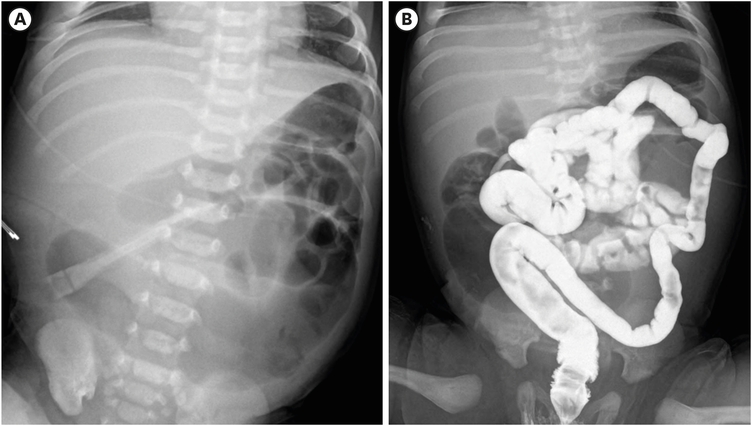
Fig. 5
Ileal atresia. (A) A plain abdominal radiograph taken 10 hours after birth shows a distal small bowel obstruction. (B) A contrast enema reveals a small colon that does not fill the dilated loops of the bowel.
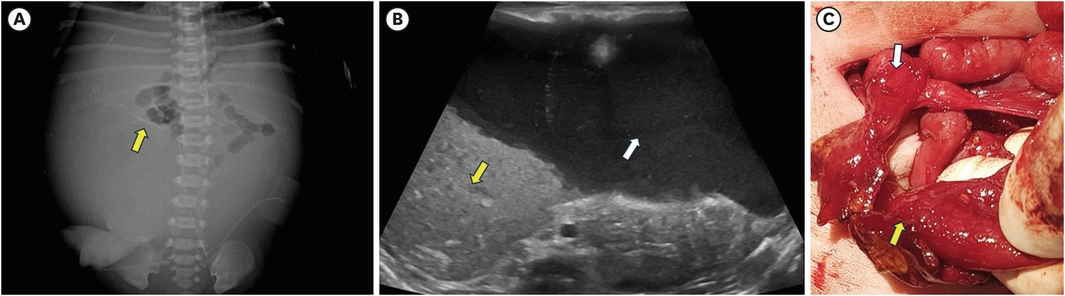
Fig. 6
Meconium peritonitis. (A) Peritoneal calcifications (yellow arrow) are present in the right abdomen. This plain radiograph, taken 4 hours after birth, shows the bowel being compressed by the pseudocyst; hence, bowel gas is only visible in the proximal bowel. (B) A large amount of fluid (white arrow) with echogenic debris (yellow arrow) occupies most of the peritoneal cavity in the ultrasound. (C) The patient had a massive meconium pseudocyst that took up most of the abdominal space. After the pseudocyst was removed, a type IIIa ileal atresia (with the yellow arrow indicating the proximal end and the white arrow indicating the distal end) was confirmed. The patient recovered well post-surgery.
Once diagnosed, gastric decompression should be performed through a nasogastric tube, along with fluid resuscitation to correct electrolyte abnormalities and hypovolemia. If there are suspicions of perforation or infection, broad-spectrum antibiotics should be administered. Surgery should be performed as soon as possible after diagnosis.
There are several methods for approaching the intraperitoneal. The traditional approach is to make a transverse incision about 2 cm above the umbilicus. Laparoscopic-assisted surgery using an inverted smile incision at the umbilicus has also been recently introduced [25]. Neonatal JIA surgery using a circumumbilical incision is as effective as traditional supraumbilical transverse incision, and showed less morbidity and better cosmetic results [26]. Regardless of the method of approach, the most important thing is to be able to observe and access the entire intestine and peritoneal cavity. The entire bowel should be carefully observed to confirm the type of JIA, the length of the entire small bowel, and any other abnormalities. The distal limb of the atretic bowel can be confirmed by continuity by passing warm saline through a small rubber catheter. Colonic continuity can be confirmed by contrast enema before surgery, or if not performed, by a transrectal catheter placed before surgery.
The histologic villi of the proximal dilated and hypertrophied blind end are normal. However, there is no effective peristalsis in that intestine. Therefore, if the length of the functional bowel is sufficient, resection of the dilated and hypertrophied proximal bowel, with primary end-to-end anastomosis with or without tapering of the proximal bowel, is the most common technique (Fig. 7) [27]. Side-to-side anastomosis should not be performed because it increases the risk of blind loops [27]. If proximal bowel resection is not feasible, tapering enteroplasty or plication of the dilated bowel is a useful technique [28]. In most end-to-end anastomosis situations, there is a size discrepancy between the transected proximal and distal ends. In this case, an incision can be made along the antimesenteric border of the distal bowel to create an appropriate distal enterotomy for anastomosis.
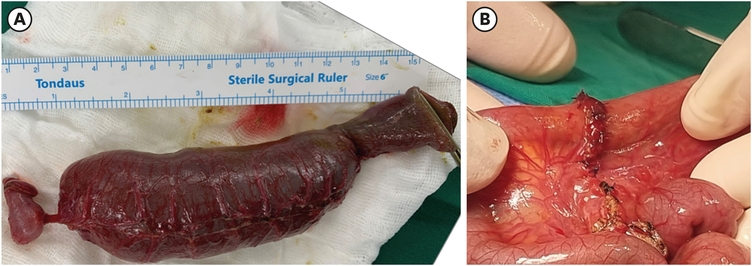
Fig. 7
Resected specimen and anastomosis. (A) Resection of proximal dilated and hypertrophied bowel. (B) End-to-end anastomosis.
The surgery for type IIIb atresia should divide the restricting bands that are attached along the distal coiled and narrow mesentery to maximize blood supply. After that, the bowel is restored to the abdomen, and care should be taken to prevent bowel torsion. If distal bowel viability is suspected, limited resection should be performed to prevent complications such as volvulus. When such limited resection is done, the long-term result has been favorable [29]. Surgery for type IV atresia depends on whether the multiple atresia is close together and whether sufficient bowel length remains after resecting this section. If yes, a single anastomosis is preferred. Otherwise, multiple anastomoses should be performed. The ultimate goal of surgery in JIA is to restore intestinal continuity while maintaining both intestinal function and length.
The length of the small bowel in types I and II of JIA is similar to that of a normal infant; therefore, the prognosis after surgery is favorable. In type IIIa, the dilated proximal blind bowel is often aperistaltic and prone to volvulus or overdistension, leading to secondary necrosis and perforation [30]. Therefore, the overall length of the small bowel in type IIIa is variable, but is generally shorter than normal as the affected bowel would have undergone intrauterine resorption. Type IIIb appears as proximal jejunal atresia, with the distal bowel at high risk of volvulus and impaired vascularity [31]. This type is often born premature, up to 50% with malrotation, and 63% morbidity and 54% mortality have been reported [13, 32]. The most likely explanation is that this type is the result of proximal superior mesenteric artery occlusion with extensive infarction of the proximal midgut, and is also thought to occur as a result of in utero midgut volvulus [31, 33]. Most of type IV cases are sporadic, with no family history of intestinal abnormalities. Around 25% of non-familial multiple intestinal atresia patients have reported central nervous system abnormalities [34]. Some have been associated with severe immunodeficiency linked to a rare mutation in the TTC7A gene [2]. A familial form of multiple atresia is thought to be autosomal recessive, with atresia occurring throughout the intestine, and is a lethal type characterized by long segments of completely occluded intestine without a recognizable lumen [35].
Infections like pneumonia, peritonitis, or sepsis are the most common causes of early death in JIA patients [13]. Functional obstruction and leakage at the surgical junction after surgery are significant postoperative complications, with a reported mortality rate of 15% due to these complications [13, 36]. Other factors affecting morbidity and mortality include associated anomalies, respiratory distress, prematurity, short bowel syndrome, and postoperative mechanical intestinal obstruction [13]. Today, the survival rate of JIA patients is over 90% [10]. A survey by the KAPS in 2010 found that the mortality rate for JIA from 1994 to 1996 was 13.8%, but it improved to 3.4% from 2007 to 2009 [4]. Significant improvements in mortality have been observed worldwide. These improvements are due to the following factors: First, the understanding that the proximal dilated and hypertrophied bowel is dysfunctional. Second, improvements in the anastomotic technique and suture material. Third, the development of total parenteral nutrition. Poor prognosis is mostly associated with short bowel syndrome. The prognosis of short bowel syndrome is determined by the remnant small bowel length, the presence of the ileocecal valve, and the dependence on long-term parenteral nutrition [37]. The length of the small bowel in newborns is not easy to measure accurately immediately after birth, but generally if less than 25 cm of small bowel remains after surgery, long-term parenteral nutrition and intestinal lengthening procedures are necessary. Several studies reported that the occurrence rate of short bowel syndrome following surgery for JIA ranges between 10.9% and 22.3%. Meanwhile, the need for intestinal lengthening was reported to be between 0.8% and 3.8% [10, 38, 39, 40]. JIA accounts for 10% of surgical causes of intestinal failures in pediatrics [41].
With the advent of imaging and genomics, there is a growing interest in identifying specific biomarkers or imaging profiles that could aid in the early detection of JIA, which could potentially enable earlier intervention or management. However, as of now, no definitive biomarkers for JIA have been identified. Estimation through ultrasound in the mother’s late stages of pregnancy is currently the fastest diagnostic method.
Among the recently spotlighted studies are those related to intestinal organoids and stem cells. One such study was conducted by Takahashi et al. [42] in 2021. The study discusses the use of organoids to model intestinal stem cell function and the cholinergic system involved in intestinal epithelial cells and intestinal stem cells. The authors outline an organoid-based organ replacement approach for intestinal diseases. Another study in 2020 describes the establishment and culture of human intestinal organoids derived from adult stem cells [43]. The study highlights the usefulness of intestinal organoids for the study of intestinal physiology as well as many disease conditions. While the current studies remain foundational, the progression of such research raises hopes for a future where conditions like JIA could be treated without the need for surgical interventions.
The management and prognosis for JIA have improved dramatically with advances in surgical techniques and neonatal intensive care. Early diagnosis, aggressive resuscitation, timely surgical intervention, and meticulous postoperative care are essential for a favorable outcome. While most patients can be expected to live a normal life, those with associated anomalies or short bowel syndrome may require long-term parenteral nutrition and face a higher risk of associated complications. The future should focus on innovations in surgical techniques, better understanding of the disease, and improved postoperative care to enhance outcomes further. Additionally, further research into the genetics and etiology of JIA is required to provide more comprehensive insights into this condition and its management.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
