

Gallstone ileus occurs when there is a fistula between the gallbladder and the small intestine, by which the gallstone reaches the small bowel and thereby inducing bowel obstruction. This condition is very rare in the overall population, accounting for only 0.1–5%. It is also very rare in the pediatric population and in the patients who undergo Kasai operation as well. Worldwide, only two cases have been reported. Gallstone production may be facilitated under certain circumstances, and migrated stone induces ileus. Diagnosis is usually done by imaging studies such as abdominal ultrasonography and computed tomogram (CT). Surgical removal of stone is decisive treatment. The 22-year-old female patient with a history of Kasai operation at age of 1 month visited emergency department for abdominal pain. The most reasonable impression was the acute exacerbation of the chronic cholangitis, but it was improved soon after intravenous antibiotics treatment. At the same time, mechanical ileus was diagnosed and exacerbated during admission. CT was done to find out the cause. Small bowel obstruction by a round material was observed. By considering its clinical course and the imaging, the material was suspected to be gallstone. The patient underwent enterolithotomy under general anesthesia. She was fully recovered from gallstone ileus after stone removal. There has been no recurrence of ileus nor cholangitis. When a patient with a history of Kasai portoenterostomy complains mechanical ileus, the clinician need to allow for gallstone ileus referring patient’s history and medical condition which promotes to induce stone formation.
Gallstone ileus occurs when there is a fistula between the gallbladder and the small intestine, by which the gallstone reaches the small bowel and thereby inducing bowel obstruction. This condition is very rare in the overall population, accounting for only 0.1–5%. It is also very rare in the pediatric population and in the patients who undergo Kasai operation as well. Worldwide, only two cases have been reported. Gallstone production may be facilitated under certain circumstances, and migrated stone induces ileus. Diagnosis is usually done by imaging studies such as abdominal ultrasonography and computed tomogram (CT). Surgical removal of stone is decisive treatment. The 22-year-old female patient with a history of Kasai operation at age of 1 month visited emergency department for abdominal pain. The most reasonable impression was the acute exacerbation of the chronic cholangitis, but it was improved soon after intravenous antibiotics treatment. At the same time, mechanical ileus was diagnosed and exacerbated during admission. CT was done to find out the cause. Small bowel obstruction by a round material was observed. By considering its clinical course and the imaging, the material was suspected to be gallstone. The patient underwent enterolithotomy under general anesthesia. She was fully recovered from gallstone ileus after stone removal. There has been no recurrence of ileus nor cholangitis. When a patient with a history of Kasai portoenterostomy complains mechanical ileus, the clinician need to allow for gallstone ileus referring patient’s history and medical condition which promotes to induce stone formation.
Formation of biliary stones after Kasai procedure is an uncommon complication. Gallstone ileus after Kasai operation is also a very rare clinical entity [1, 2]. We present a case of intestinal obstruction due to gallstone in a patient 22 years after a Kasai portoenterostomy for biliary atresia. She initially visited the emergency department (ED) for acute cholangitis, however, gallstone ileus was found during admission. It was resolved by enterolithotomy. Possible etiology of this clinical presentation is discussed.
A 22-year-old female patient visited the ED with epigastric pain and high fever up to 39°C which started on the day of visit. She had received Kasai portoenterostomy 41 days after birth due to biliary atresia and redo-Kasai after 14 days due to recurrence of biliary obstructive symptoms, such as whitish pasty stool. After Kasai operation, she was lost to follow-up for several years. Recently she underwent a repeated cholangiohepatitis requiring admission.
Considering her previous history, cholangiohepatitis was the first impression. Her aspartate transaminase and alanine transaminase level were elevated (131 IU/L and 67 IU/L, respectively). Her total bilirubin level was mildly increased (1.6 mg/dL). Her serum levels of alkaline phosphatase and gamma-glutamyl transpeptidase were also increased (136 IU/L and 145 IU/L, respectively). Abdomen X-ray taken at ED suggested ileus with bowel dilatation and a step-ladder sign.
She was admitted to the pediatric department for conservative management of cholangitis and ileus. Liver ultrasonography was done on the 2nd day of admission. It revealed acute on chronic cholangiohepatitis. Echogenic material with posterior shadowing at portoenterostomy site was found in liver ultrasonography at two months prior to the ED visit. This finding was substituted by echogenic fluid at the same site (Fig. 1A). Abdominal computed tomography (CT) taken around the same time revealed stone-like material at the same location (Fig. 1B). Intravenous teicoplanin and meropenem were applied. They were also used in the previous event. However, on hospital day 9, she started to complain more severe abdominal pain. Gaseous distension in the X-ray did not improve. It seemed to be exacerbating (Fig. 2A). Abdominal CT was taken on hospital day 12. It showed long segmental dilatation of the small bowel with obstruction with a dense material that was about 3.1×3.9 cm size in the ileum. Distally migrated biliary stone was suspected for the dense material (Fig. 2B).
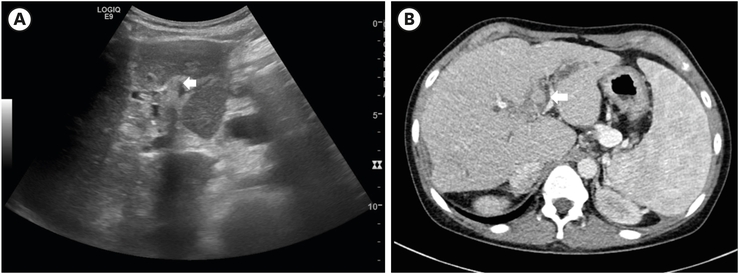
Fig. 1
Stone-like material in the portoenterostomy site (A) in liver ultrasonography and (B) in computed tomogram found at 2 months before visiting emergency room (arrow).
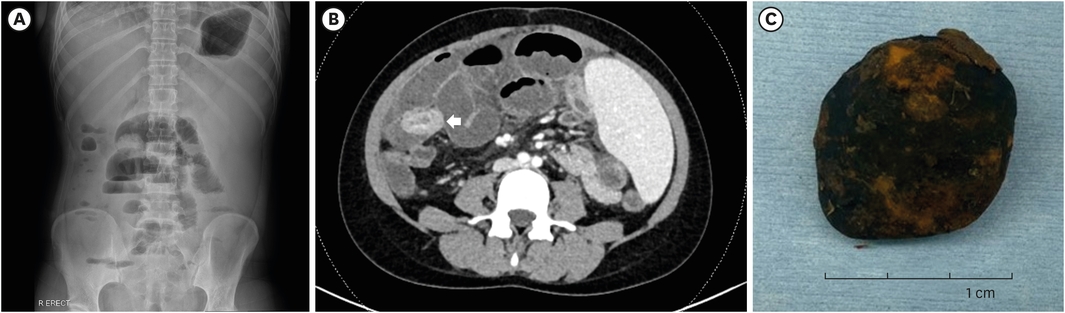
Fig. 2
Gallstone that induced small bowel obstruction. (A) Plain abdominal radiography revealing an obstructive small bowel ileus. (B) Computed tomogram reveling gallstone (arrow) in the small bowel. (C) A brown-colored gallstone of 3.7×3.2 cm in size found during operation.
Due to no improvement of bowel obstruction, she was transferred to the pediatric surgery department for surgical correction of gallstone ileus on hospital day 15. Laparoscopic approach was tried at first. However, open conversion via previous incision was done due to severe adhesion along the whole visceral organs. Adhesiolysis was done and a stone was removed via enterotomy at the distal ileum. It was a brown-colored gall stone of 3.7×3.2 cm in size (Fig. 2C).
Postoperatively, she showed satisfactory progress. She was discharged on post-operative day (POD) 14. She is now stable without recurrence of cholangitis nor ileus.
Gallstone ileus is a mechanical obstruction of bowel by cholelithiasis impaction. It accounts for 0.1%–5% of bowel obstruction cases in the general population [3]. It is mainly a geriatric disease with comorbidities. It is also rare in the pediatric population [3]. However, a few patients with Roux-en-Y hepaticojejunostomy (portoenterostomy) have been reported recently [1, 2, 3, 4, 5]. A 68-year-old female who presented with gallstone ileus 20 years after cholecystectomy and 14 years after Whipple procedure was reported in 2000 as the 1st case of gallstone ileus in a patient with hepaticojejunostomy [1]. For the pediatric population, Van den Eijnden et al. has reported two cases as complications following excision of choledochal cyst excision and hepaticojejunostomy formation [5]. It is also a rare condition in post-Kasai status with only two cases reported up to date, worldwide [1, 2].
In a report from the Japanese biliary atresia registry, more than half (52.8%) of patients achieved 10-year survival without liver transplantation like our patient [6]. Since 1998, most patients have received Kasai operation for correcting biliary atresia. The incidence of post-operative cholangitis was 62% for portoenterostomy and 56% for portoenterostomy with intestinal valve [6]. As these patients grow older, the possibility of a problem associated with gallstone formation can increase. Nichol et al. has reported that the staple used for antireflux value can act as precipitating factor for gallstone formation [1]. Another case has reported gallstone ileus in a pregnant female patient [2].
Portoenterostomy seems to provide a condition that favors the formation of a gallstone. It acts as an artificial fistula between biliary system and small bowel and provides space in which a large gallstone grows. Repeated bacterial cholangitis by bile acid reflux also contributes to stone formation. In contrast, its rarity can be explained by a ‘neogallbladder’ function of efferent loop storing and concentrating of biliary cholesterol complex as time passes [4]. Continuous bile acid flow without stasis might lead to gallstone formation [7]. Small stones which can pass the ileocecal valve are not problematic because they are excreted before they cause bowel obstruction. In our patient, the stone was observed in the portoenterostomy site in the CT and US done at outpatient clinic 2 months before ileus. Stone which was found in CT during hospitalization seemed to be the same one, so we concluded that the migrated stone from portoenterostomy site to distal small bowel induced obstructive ileus.
She had many factors affecting the gallstone formation. Hypersplenism and accompanied cytopenia which promoting bilirubin excretion, long-term administration of high dose steroid including methyl prednisolone pulse therapy (not low dose) and followed hyperlipidemia, dilated portoenterostomy space, and liver cirrhosis itself contributed to progression of stone formation. She has suffered chronic cholangiohepatitis after Kasai portoenterostomy. She had a history of repeated acute on chronic cholangiohepatitis. She was also diagnosed and exacerbated since adolescence with juvenile idiopathic arthritis and idiopathic thrombocytopenia with long-term application of medications. Adalumumab was administered but changed to tocilizumab due to lupus progression. Prednisolone was kept over a long term. In addition, she received several methylprednisolone pulse therapies to control flare-up of her rheumatic disease. Her immunosuppressive status might be the precipitating factor for the repeated acute cholangitis. Prednisolone is known to promote gallstone formation and slow small intestinal transit [8, 9]. Use of immunosuppresant can aggravate relapsing acute choangiohepatitis [10]. Redo-Kasai operation at POD14 in which the portal bed was enlarged into 5cm in diameter probably allowed large-size anastomosis and provided enough space for large gallstone formation. Post-portoenterostomy cholangitis might have initiated the formation of gallstone. Other medical conditions might have aggravated its progression.
Gallstone without calcification usually cannot be visualized in a routine abdominal X-ray, which is the present case. The stone was diagnosed by CT. Enterolithotomy is a surgical procedure of choice [11].
Gallstone ileus is a definite rare condition in post-Kasai status, especially after a considerable time has passed after an operation. However, in a patient with certain medical conditions that can promote large gallstone formation as in our patient, the practitioner should take into consideration gallstone ileus as a differential diagnosis of bowel obstruction.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: G.S., K.H.Y.
Investigation: G.S., Y.J.K., K.H.Y.
Writing - original draft: G.S.
Writing - Review & editing: Y.J.K., K.H.Y.
