

Purpose
During the coronavirus disease 2019 pandemic, with an aim to reduce the burden on the strained health care resources, operating on suspected perforated appendicitis while managing simple appendicitis conservatively was followed in our institution. The aim of this study was to determine the predictive value of clinical features and investigations for discriminating between perforated and non-perforated appendicitis in children and devise a scoring system.
Methods
A retrospective study of all consecutive children who underwent appendectomy for acute appendicitis at our institution, a tertiary care pediatric center in South India, between 1st June 2020 to 31st May 2021 (period, one year) was carried out. In line with our standard operative procedure suspected perforated appendicitis were operated while simple appendicitis were managed conservatively in our institution. Patient demographics details, clinical features and investigations data were collected, and univariate and multivariate analysis carried out.
Results
Total of 58 patients were included in the study. Longer duration of symptoms, leukocytosis, serum sodium <135 mEq/L, appendicolith and free fluid and abscess on ultrasonography are good predictors of perforated appendicitis. We have evolved a reliable scoring system to identify perforated appendicitis.
Conclusion
Accurate identification perforated appendicitis with our scoring system is possible and results in effective usage of health care resources.
During the coronavirus disease 2019 pandemic, with an aim to reduce the burden on the strained health care resources, operating on suspected perforated appendicitis while managing simple appendicitis conservatively was followed in our institution. The aim of this study was to determine the predictive value of clinical features and investigations for discriminating between perforated and non-perforated appendicitis in children and devise a scoring system.
A retrospective study of all consecutive children who underwent appendectomy for acute appendicitis at our institution, a tertiary care pediatric center in South India, between 1st June 2020 to 31st May 2021 (period, one year) was carried out. In line with our standard operative procedure suspected perforated appendicitis were operated while simple appendicitis were managed conservatively in our institution. Patient demographics details, clinical features and investigations data were collected, and univariate and multivariate analysis carried out.
Total of 58 patients were included in the study. Longer duration of symptoms, leukocytosis, serum sodium <135 mEq/L, appendicolith and free fluid and abscess on ultrasonography are good predictors of perforated appendicitis. We have evolved a reliable scoring system to identify perforated appendicitis.
Accurate identification perforated appendicitis with our scoring system is possible and results in effective usage of health care resources.
Coronavirus disease 2019 (COVID-19) pandemic has severely strained health care resources, overstretching health systems and hampering effective operations [1]. Further to the World Health Organization (WHO) guidelines to maintain essential services which stressed prioritization, the surgical community had a relook, aimed at deferring operative procedures and considering nonsurgical options [2].
Acute appendicitis in children, with a high propensity towards perforation, represents the most frequent reason for abdominal surgery, frequently in emergency setting [3]. Studies in the recent past have explored the possibility of antibiotic treatment without surgery of pediatric patients with simple appendicitis. Meanwhile there has been a paradigm shift towards early appendectomy in complicated appendicitis, as it is associated with lesser hospital stay, cost, complications, and frequency of hospital readmission, making it imperative to differentiate the two more so during the massive pandemic [4].
The aim of our study was to determine the predictive value of clinical features and investigations for discriminating between perforated & non-perforated appendicitis and devise a scoring system.
A retrospective study of all consecutive children who underwent appendectomy for acute appendicitis at our institution, a tertiary pediatric center in South India between 1st June 2020 to 31st May 2021 (period, one year) was carried out. During the COVID-19 pandemic we implemented a standard operative procedure to reduce the burden, especially on operating room wherein children with suspected perforated appendicitis were operated while simple appendicitis were managed conservatively with intravenous antibiotics and supportive care.
All consecutive children with suspected perforated appendicitis were included in this study. However, in case of acute appendicitis managed conservatively, medical records were not available. Those were excluded.
Data regarding patient demography, various standardized parameters among clinical features, and investigations, both laboratory and ultrasonography along with intra operative surgery findings were collected from the inpatient hospital records. The ultrasonography was done by two radiologists.
Symptoms included pain abdomen, vomiting, fever (elevated temperature >38°C), 1st episode. Signs included tenderness, rebound, guarding, and mass [3, 5, 7].
Laboratory outcomes included total leucocyte count, neutrophils, and serum sodium. Ultrasonography measured diameter, appendicolith, loss of echogenic submucosal layer, presence of peri-appendiceal echogenic fat, and free fluid & abscess [6, 8].
On the data collected univariate and multivariate statistical analysis as follows was carried out: χ2 test, Mann U Whitney test, receiver operating characteristic (ROC) curve, multiple linear regression.
Statistical analyses were performed using MS excel and Social Science Statistics (Socscistatistics.com).
n is the sample size, z is the statistic corresponding to level of confidence, p is expected prevalence (that can be obtained from same studies or a pilot study conducted by researchers), q=1−p, d is precision [3, 7].
z at 95% confidence index is 1.96, z2 is approximately 4, Chandrashekar et al. [7] in South India concluded that p is one-fifth of the pediatric appendicitis patients presenting in tertiary care patients had perforated appendicitis (hence p: 17 [one-fifth of 87], q: 1−p, d: precision 10% [0.1], n=4×0.17×0.83/0.01, n=56).
Institutional Ethical Review Board (IERB) approval was obtained for the study.
During the study period a total of 134 children were diagnosed with acute appendicitis of which 58 underwent appendectomy. Thirty-four were found to be perforated (P group) while 24 were non-perforated (NP group) during surgery. The age of the children ranged from 2-year 1 month to 17-year 4 month with mean of 8.83 year. There was no significant statistical difference of age between NP and P groups (NP: 9.73±3.97, P: 8.18±4.05; Mann–Whitney U test, p=0.08) (Table 1).

Table 1
Age distribution
The male to female ratio noted was 2:1 which was similar in both groups. Twenty-four of the total children were from rural regions and 34 from urban regions There was also no significant urban/rural regional variation among the two groups with distribution as follows: NP rural 11 and urban 13, P rural 13 and urban 21(χ2 test, p=0.78) (Table 2).
Table 2
Sex distribution
On analyzing the above-mentioned parameters and considering a cut off of significance at p<0.05, we ascertained eight parameters with sensitivity ranging from 46% to 96% and specificity 43% to 91% (Table 3).

Table 3
Significant 8 parameters with p<0.05 with sensitivity, specificity, PPV, NPV, and accuracy
We devised Indira Gandhi Institute of Child Health scoring system – I Gee score (I Gee is an acronym for our institution) with the above 8 parameters viz pain abdomen >48 hours, fever >24 hours, 1st episode, clinical guarding, total leucocyte count >14,000, serum sodium <135 mEq/L, presence of appendicolith and free fluid and abscess on ultrasonography. Each parameter was scored on a binary system 1 – yes, 0 – no with a total minimum score of 0 and maximum score of 8. Further categorization was done as follows: 0–2, no perforation 3, possible perforation; and 4–5 probable perforation and 6 and above definite perforation (Fig. 1).
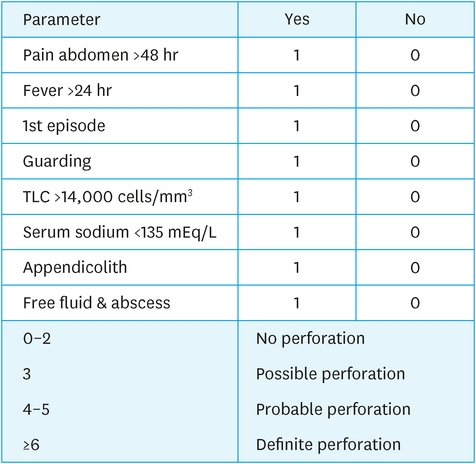
Fig. 1
I Gee score.
TLC, total leucocyte count.
On applying the I Gee score on our patient data for both the non-perforated and perforated groups and further categorization we noted that 16 were non-perforated while 0 were perforated at a score of 0–2 while 1 was non- perforated and 25 were perforated at a score of 4 and above (Table 4, Fig. 2).

Table 4
I Gee score for non-perforated and perforated groups and further categorization
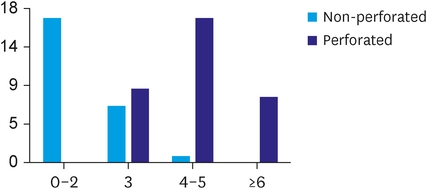
Fig. 2
I Gee score for non-perforated and perforated groups and further categorization.
Based on our data we propose a cut off score greater than 2 suggests perforated appendicitis and score 0–2 suggests no perforation with sensitivity 100% and specificity 66.67%.
ROC curve was plotted for the data which yielded area under the curve (AUC) of 0.945 (>0.7 acceptable, >0.9 outstanding) (Fig. 3).
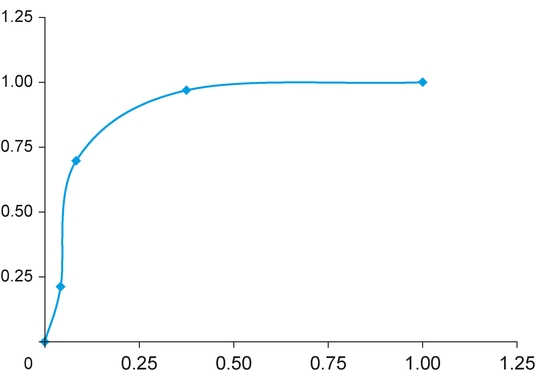
Fig. 3
ROC curve.
ROC, receiver operating characteristic.
Using multiple linear regression, we obtained a formula as follows Fig. 4.
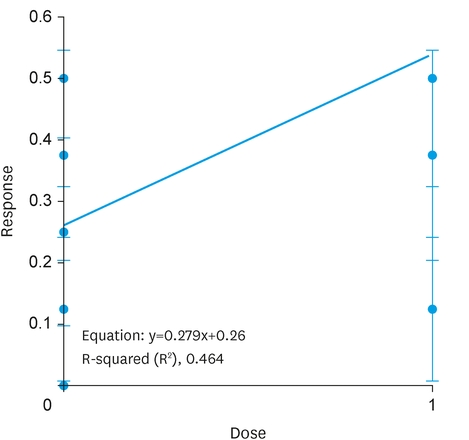
Fig. 4
Linear regression.
The novel COVID-19 pandemic presenting a once in a century challenge to human healthcare drastically changed the world health scene. In March 2020 the WHO released guidelines to help countries maintain essential health services during the COVID-19 pandemic in view of the great demands needed for the COVID-19 response and mitigating the risk of health system collapse. It urged countries to identify ‘priority’ essential services and make strategic shifts and adapt new guidelines [1, 2].
Surgical practice was significantly impacted, having to triage the urgency of surgical procedures and consider non-surgical management options where possible. The need of the hour was to devise specific guidelines and action plans to be able to continue to provide safe and effective care during the pandemic specially in resource limited settings. The surgical community at large was in agreement that where feasible non-operative management must be explored first. Worldwide Surgical bodies called for appendicectomy for acute complicated appendicitis, presence of appendicolith, perforation or disease extension outside right iliac fossa and defer cases of uncomplicated appendicitis, being managed with a trial of intravenous antibiotics [2].
Acute appendicitis, a common surgical emergency among children with up to 10% presenting with abdominal pain having acute appendicitis, represents the most frequent reason for abdominal surgery. Complicated appendicitis is a pertinent disease in pediatrics. Children with acute appendicitis have higher rates of perforation compared with adults with about 30%–75% of children progress to perforation, especially in children younger than 5 years [3, 5, 6]. It has been reported that one-fifth of the pediatric appendicitis patients presenting in tertiary care center in South India had perforated appendicitis [7].
Though literature indicates that the accuracy of a clinical diagnosis of acute appendicitis, ranges somewhere between 70% and 85%, to identify perforation more so in children may present a dilemma [4]. Several publications provide a detailed discussion on the role and validity of various clinical features, laboratory investigations and imaging including ultrasonography for diagnosis of acute appendicitis, uncomplicated and complicated, in children [3, 5, 6]. Laboratory markers, less affected by subjective factors, may be used as a more reliable index to predict perforation [3].
The findings of our study are in concordance with a recent article in 2019 which suggested that children with perforated appendicitis often presented with significantly longer duration of symptoms, higher white blood cell count and lower serum sodium level [6].
In our study also children with complicated acute appendicitis tend to have a higher average symptom duration, 24–48 hours as previously reported by Banerjee et al. [4] and Pham et al. [9].
Our finding of 91% specificity, the highest, for a serum sodium <135 mEq/L as a pointer for perforated appendicitis is significant. Recently, hyponatremia has been described as a new predictor of perforated appendicitis, being more useful than total leucocyte count in diagnosing complicated appendicitis. Our results are similar [6].
The exact pathophysiological mechanism between hyponatremia and complicated appendicitis including perforation is yet to be elucidated. Explanations include the “mmune-neuroendocrine interface,” involving cytokines in which interleukin-6 plays an important role leading to increased vasopressin secretion and inducing thirst and increased water intake. This dual combination results in hyponatremia. A role for antidiuretic hormone has also been postulated [10].
Our study reaffirms the role of ultrasonography in the management of perforated appendicitis and with presence of appendicolith and free fluid/ abscess being ominous markers. To reiterate, ultrasound is now standard practice in children, being useful, sufficient and modality of choice in the diagnosis of perforated appendicitis with computed tomography reserved for when the appendix is not identified or a high index of suspicion of perforation not confirmed on ultrasonography [8].
Literature is abounded with scoring systems related to acute appendicitis, with the role of Alvarado-, Tzanakis, and Pediatric Appendicitis Score being widely validated. Historically, most clinical prediction rules have been developed to support the diagnosis of acute appendicitis (without differentiation in type). However, they are not designed to identify perforated appendicitis, though few like the modified Heidelberg Appendicitis Score (HAS) and the Artificial Intelligence (AI) scores that hold some promise in this regard still need validation [5, 11].
The I Gee score we have devised combines clinical features and investigations including laboratory and ultrasonography to differentiate and detect perforated and non-perforated appendicitis to influence the management without compromising patient care and safety.
In comparison with other scores, we note a specificity of 95% and accuracy of 81% with AUC 0.945, higher than previous described scores (Table 5) [5, 11, 12].
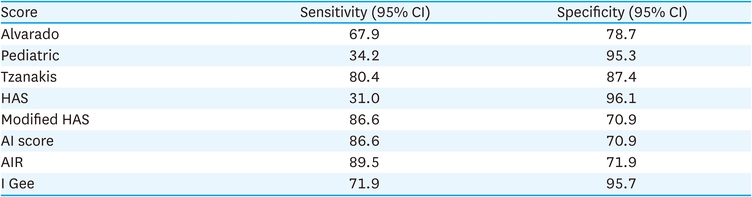
Table 5
Comparison with other scoring systems
The modified HAS and the AI scores also tend to suggest that clinical signs are less important than previously assumed in the diagnosis of pediatric appendicitis, with prominence being given to laboratory investigations and ultrasonography, which is also suggested by our results [5]. Of note, the findings of our study are similar to the AI score being notable that unlike all other scores, it does not consider tenderness of the right lower quadrant to be a significant predictor [5]. Also that a high score like in Appendicitis Inflammatory Response (AIR) score high probability score was related to evolutionary stage of the disease and perforation [4].
In conclusion, longer duration of symptoms, leukocytosis, serum sodium <135 mEq/L, appendicolith and free fluid/abscess on ultrasonography are good predictors of perforated appendicitis. The I Gee Score can accurately identify perforated appendicitis and results in effective usage of health care resources.
This study has limitations. Our findings are limited hospital-based, single center study, this should be validated in prospective, developed multicenter studies. Clinical features and ultrasonography are clinician/operator dependent with inter-observer variability.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Presentation:This study was presented as a free paper in IAPSCON 2021, the 47th annual conference of the Indian Association of Pediatric Surgeons.
Author Contributions:
Conceptualization: LN.S., J.V.
Data curation: LN.S.
Formal analysis: LN.S.
Investigation: LN.S.
Methodology: J.V., BC.G.
Project administration: BC.G.
Software: LN.S.
Supervision: BC.G.
Validation: J.V., BC.G.
Visualization: J.V., BC.G.
Writing - original draft: LN.S.
Writing - review & editing: J.V., BC.G.
