

Jejuno-ileal atresia is often associated with various other gut pathologies. A 5-day male presented with bilious vomiting, abdominal distension and non-passage of stools. Exploratory Laparotomy showed a type IIIA ileal atresia with midgut volvulus and atypical malrotation for which Ladd’s Procedure and anastomosis of atretic bowel was done. A fleshy tubular structure extracted from distal bowel showed ileal duplication. In JIA, the vascular theory of pathogenesis is widely accepted with multiple studies to suggest the same. The mechanism being mesenteric ischemia leading to intestinal necrosis, resorption, and atresia. It has been found that abdominal duplication cyst often occurs simultaneously with short bowel, intestinal atresia, stenosis and enteric duplication for which a common vascular pathogenetic mechanism has been suggested. Our case serves as an in vivo description of the proposed theory where the findings may be described elegantly. We describe and discuss the mesenteric ischemia theory in bowel atresia and hope to further our understanding about the same.
Jejuno-ileal atresia is often associated with various other gut pathologies. A 5-day male presented with bilious vomiting, abdominal distension and non-passage of stools. Exploratory Laparotomy showed a type IIIA ileal atresia with midgut volvulus and atypical malrotation for which Ladd’s Procedure and anastomosis of atretic bowel was done. A fleshy tubular structure extracted from distal bowel showed ileal duplication. In JIA, the vascular theory of pathogenesis is widely accepted with multiple studies to suggest the same. The mechanism being mesenteric ischemia leading to intestinal necrosis, resorption, and atresia. It has been found that abdominal duplication cyst often occurs simultaneously with short bowel, intestinal atresia, stenosis and enteric duplication for which a common vascular pathogenetic mechanism has been suggested. Our case serves as an in vivo description of the proposed theory where the findings may be described elegantly. We describe and discuss the mesenteric ischemia theory in bowel atresia and hope to further our understanding about the same.
Jejuno-ileal atresia (JIA) in neonates has been known to be associated with various other gut pathologies such as duodenal or pyloric atresia, malrotation with volvulus, duplication of gut and anorectal malformation. The incidence of JIA with small bowel duplication has been previously reported at 0%–4.7% [1, 2]. Here we report a triple anomaly of type IIIA ileal atresia with ileal duplication and atypical malrotation with midgut volvulus.
A 5-day, full term, male was referred to us with vomiting which was initially semi-digested milk but become bilious over 24 hours. The baby also developed progressive abdominal distension and non-passage of stools. Clinical examination revealed a moderately dehydrated baby with no meconium per rectum even after a rectal saline wash. No antenatal ultrasound findings were available. Abdominal X-ray was suggestive of multiple dilated bowel loops with air fluid levels (Fig. 1). Exploratory laparotomy was planned with a provisional diagnosis of small bowel atresia.
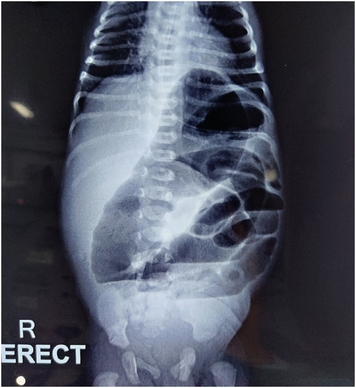
Fig. 1
Erect X-ray done in Emergency Room showing dilated bowel loops with few air-fluid levels.
On exploration via right upper quadrant transverse incision, a dilated, blind ending ileum with a wide mesenteric defect was noted at about 120 cm distal to Duodeno-jejunal flexure. The proximal ileum and jejunum were rotated 1.5 turns clockwise about their mesentery with maintained bowel viability. On de-rotation the mesentery was narrow and Ladd’s bands were also noted. Duodeno-Jejunal flexure was at its normal position. Ladd’s bands were divided and primary resection and anastomosis was planned. On incising the blind end of the distal ileum, a tubular structure of about 3 cm was extracted from its lumen (Fig. 2). This fleshy tube had no luminal communication with the distal bowel and its distal most part appeared blackish and necrotic. The dilated proximal atretic bowel about 15 cm & the tubular 3 cm structure along with a portion of distal ileum was excised and end to end anastomosis performed.

Fig. 2
Distal atretic bowel (bowel lip grasped with forceps) from whose lumen a thin fleshy tube-like structure (duplicated intussuscepted bowel) with blackish necrotic distal end was pulled out.
The excised specimen (Fig. 3) on histopathology examination was reported as a dysplastic proximally atretic ileum and a tubular duplication cyst in the fleshy structure fished out from the distal end. Post operative course was uneventful (Fig. 4). Patient was kept nil per oral for 5 days, gradually weaned to full feeds and discharged by 9th post operative day. On follow up visit he was doing well.
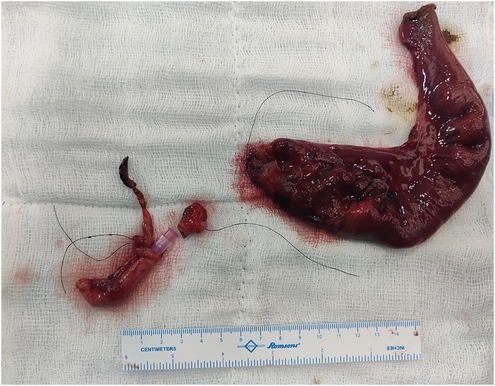
Fig. 3
Complete resected specimen of proximal (dilated) and distal atretic bowel with the fleshy structure.

Fig. 4
Bowel after resection and anastomosis.
JIA has been associated with gastrointestinal anomalies like malrotation, volvulus, duplication cysts, duodenal atresia and colonic atresia. The two major theories of pathogenesis suggested for atresia are the non-recanalization theory by Tandler and vascular accident theory by Louw and Barnard [3]. In case of JIA the vascular theory is more widely accepted with multiple studies to suggest the same [2, 4, 5].
Originally, Louw and Bernard [3] were able to demonstrate the effects of mesenteric vascular accidents/ischemia on puppies. They also noted high incidence of abnormal mesenteric fixation, volvulus and intussusception in neonates with atresia. Various reports support this theory, the mechanism being mesenteric ischemia leading to intestinal necrosis, resorption, and atresia. In a landmark report of 37 neonates by Favara et al. [4], it was found that abdominal duplication cyst often occurred simultaneously with short bowel, intestinal atresia, stenosis and enteric duplication. They suggested that a common vascular pathogenetic mechanism exists which leads to different lesion depending on the severity of vascular accident and subsequent healing.
Our case serves as an in vivo description of the proposed theory where the findings may be described elegantly. In our case, recurrent episodes of intra uterine ileo-ileal intussusception at a certain portion of ileum may have led to bowel edema and subsequent irreducibility of the intussuscepted portion of bowel. Vascular compromise would have set in slowly leading to ischemia and necrosis of intussuscepted bowel at its neck and the distal most portion. Gradually the non-viable intestine and mesentery supplying it would have undergone necrosis, resorption and atresia thus leading to V shaped mesenteric defect. The small tubular tissue extracted out from the distal atretic segment (labelled as intraluminal duplication cyst by the pathologist) represents the intussuscepted portion of the bowel which has partially remained viable in the middle and partially undergone necrosis at the most vulnerable portions (the distal most tip - blackish tissue attached to the fleshy tube; and the neck - leading to atresia). With progressive period of gestation, the proximal atretic segment gradually distended as it filled with the swallowed amniotic fluid. This dilated portion of bowel with a narrow hanging mesenteric defect led to a volvulus just like a loaded sigmoid colon and is demonstrated in the findings of our case.
On closely observing the previously reported cases of atresia associated with duplication, we noted the site of the duplication cyst is usually in proximity to either of the atretic ends [6, 7, 8]. Of 17 duplication cysts studied by Rattan et al. [6], associated atresia of gut was observed in 4 cases (1 duodenal, 1 jejunal and 2 ileal). Although Peterson [5] described ileal intussusception caused by an ileal duplication cyst, which may be one of the mechanisms of bowel duplication causing atretic changes in the adjacent bowel, we presume that the intussusception would have been the inciting event leading to atresia presumed as intraluminal duplication and not vice-versa.
Few previously published reports [9, 10] have shown intussuscepted bowel in the distal atretic portion bearing similar findings to our case. However, these cases have either reported a cord like structure connecting the atretic ends or a visible intussuscepted bowel at the distal end thus making our findings unique.
We are reporting the unique findings of intraluminal intussusception leading to JIA and midgut malrotation with volvulus and the residual intussuscepted bowel reported as an intraluminal duplication cyst while describing the mechanism which could have led to the formation of such associated defects.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.B.
Data curation: D.S.
Formal analysis: S.A.K.
Investigation: S.B.
Methodology: S.R.
Project administration: S.R.
Resources: S.B.
Software: D.S.
Supervision: K.B.
Validation: S.A.K.
Visualization: S.A.K.
Writing - original draft: D.S.
Writing - review & editing: S.B.
