

Purpose
Increases in intestinal length (IL) in patients with short bowel syndrome (SBS) may differ by age and underlying diseases. This study analyzed the elongation rate of the remnant IL according to underlying disease to establish a therapeutic plan for intestinal rehabilitation.
Methods
The charts of SBS patients who underwent surgery at our center from 2000 to 2018 were retrospectively reviewed. The enrolled patients included those with a remaining IL less than 25% of the average and those with a remaining IL of approximately 50% who had been administered parenteral nutrition for more than one year. Patients were excluded if they underwent only one operation or two operations with the first being a serial transverse enteroplasty procedure, meaning that base length was not known.
Results
Ten patients were enrolled. Causes of SBS included total colonic aganglionosis (TCA) in seven patients (70.0%), necrotizing enteritis in two (20.0%), and malrotation/volvulus in one (10.0%). The IL growth rate in the three non-TCA patients was 9-fold higher than the estimated proportion, whereas the growth rate of the IL according to age was significantly lower in the TCA than in the non-TCA group (p=0.01).
Conclusion
The IL growth rate may differ between TCA and non-TCA patients in SBS. Rehabilitation protocols might consider the underlying disease. Additional larger trials are required to confirm these findings.
Increases in intestinal length (IL) in patients with short bowel syndrome (SBS) may differ by age and underlying diseases. This study analyzed the elongation rate of the remnant IL according to underlying disease to establish a therapeutic plan for intestinal rehabilitation.
The charts of SBS patients who underwent surgery at our center from 2000 to 2018 were retrospectively reviewed. The enrolled patients included those with a remaining IL less than 25% of the average and those with a remaining IL of approximately 50% who had been administered parenteral nutrition for more than one year. Patients were excluded if they underwent only one operation or two operations with the first being a serial transverse enteroplasty procedure, meaning that base length was not known.
Ten patients were enrolled. Causes of SBS included total colonic aganglionosis (TCA) in seven patients (70.0%), necrotizing enteritis in two (20.0%), and malrotation/volvulus in one (10.0%). The IL growth rate in the three non-TCA patients was 9-fold higher than the estimated proportion, whereas the growth rate of the IL according to age was significantly lower in the TCA than in the non-TCA group (p=0.01).
The IL growth rate may differ between TCA and non-TCA patients in SBS. Rehabilitation protocols might consider the underlying disease. Additional larger trials are required to confirm these findings.
Pediatric short bowel syndrome (SBS) is a malabsorptive state caused by the substantial loss of small intestine due to congenital or acquired lesions, such as necrotizing enterocolitis, gastroschisis, volvulus, total colonic aganglionosis (TCA), or multiple intestinal atresia. These infants, therefore, require long-term parenteral nutrition (PN) caused by a reduced absorptive surface or an intact mucosal surface with extensive motility dysfunction [1]. Prolonged dependence on PN is an essential treatment but predisposes to intestinal failure associated liver disease (IFALD), catheter sepsis, and the loss of the venous access sites [2, 3]. Because these morbidities are correlated with the duration of PN, complete weaning from PN is a pivotal goal of intestinal rehabilitation. Although the most rapid weaning occurs within the first year after PN initiation, patients continue to achieve enteral autonomy after many years of PN dependence as their intestinal adapts [4]. Through intestinal adaptation, including dilatation and elongation following intestinal loss, the surface of absorption could be increased [5]. Successful intestinal adaptation can make the patients wean off from PN. Contributing factors of PN weaning are age, underlying disease, remnant bowel length and part, the presence of ileocecal valve (ICV) [1, 6]. Although not the only factor, intestinal length (IL) is critical for PN weaning [1, 6, 7, 8]. IL has been reported to increase with age [6, 8]. Despite the growth rate being dependent on the disease underlying SBS, no study to date has assessed the relationship between underlying disease and IL elongation.
The purpose of this study was to compare and analyze the growth rate of IL between SBS patients and non-SBS patients over age. Furthermore, we specifically sought to evaluate the relationship between IL elongation and the diseases underlying SBS in patients treated for SBS at our institution.
This retrospective study included patients who underwent laparotomy for diseases resulting in SBS at our institution between 2000 and 2018. Data collected included gestational age, age at onset of SBS, etiology of SBS, small bowel length, presence of absence of the ICV, colonic remnant, duration of PN use, calories from PN. The primary outcome was the growth rate of IL; the secondary outcome was the ability to wean off PN. Patients were considered eligible if they were clinically diagnosed with SBS, defined as having a remaining IL of less than 25% of the average [9] or having an IL of approximately 50% and being administered PN for more than one year. We excluded the cases when the IL was uncertain. That is, patients were excluded if they underwent only one operation or if they underwent two operations with unknown IL because the first operation included a serial transverse enteroplasty procedure [10]. And patients with unclear records about IL were also excluded. By doing this, we ensured the IL of patients.
All patients underwent laparotomy, with the small bowel length measured along the antimesenteric border, starting at the ligament of Treitz (Fig. 1). IL was measured with a standard 5-cm straight ruler by a pediatric staff surgeon in all surgeries. We utilized the same measurement techniques in all patients. Data on average IL elongation according to age have been reported by Struijs et al. [8]. We set the age-dependent average IL elongation presented by Struijs et al. [8] as a control group and compared it with patients participating in the study. The IL growth rate was the ratio of IL length change in patients participating in our study, and the age-based IL growth rate was the ratio of IL length change in the control group according to age. Duration of PN use was defined as the time from the onset of SBS until the time of weaning from PN, or the last follow-up at which dependence on PN was known.
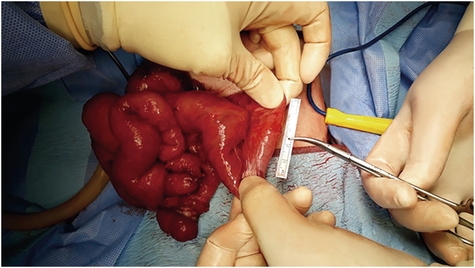
Fig. 1
Intestinal length measurement with a ruler.
Statistical analyses included the Mann-Whitney U test and the χ2 test. All analyses were performed with SPSS version 21 (IBM Corp., Armonk, NY, USA), with statistical significance defined as p≤0.05.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the ethics committee of Asan Medical Center (IRB No. 2019-0228).
Of 45 patients treated with SBS during the period, ten patients with SBS fit the inclusion criteria of this study; their demographic characteristics are outlined in Table 1. The median gestational age was 38.0 weeks (range, 24.0–40.0 weeks), with two patients being premature. The median birth weight was 2,750 g (range, 600–3,700 g), and the median postmenstrual age at the time of surgery for SBS was 38.5 weeks (range, 29.6–61.1 weeks). The underlying causes of SBS included necrotizing enteritis in two patients, including one with intestinal atresia; midgut volvulus in one patient; and TCA in seven patients, including two with accompanying intestinal atresia. Median remnant small IL after the first operation was 70 cm (range, 24–110 cm), with median percent remnant small bowel by age being 30.4% (range, 10–77.1%). None of the patients underlying TCA had remaining ICV.
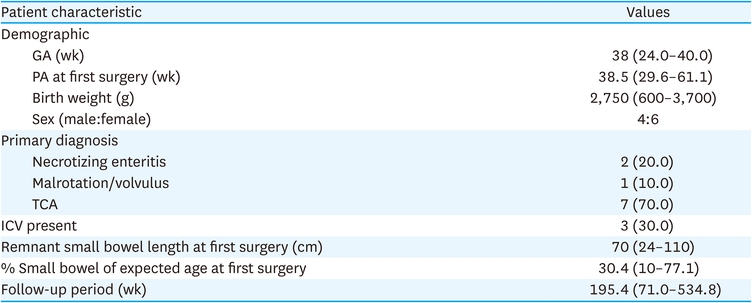
Table 1
Demographic and clinical characteristics of patients with SBS (n=10)
The median postmenstrual age at the last surgery, at which elongated IL was measured, was 92.7 weeks (range, 59.1–295.0 weeks) (Table 2). Prior to the last surgery, patients underwent 1–7 operations or an average of 2.5 operations. One patient underwent small bowel transplantation; however, graft failure resulted in its removal after 3 months later. Two patients underwent serial transverse enteroplasty (STEP) procedure at the last surgery. The median growth rate of the remnant intestine was 70.9% (range, 25.0%–218.2%), with all but three patients showing a greater than 100% growth rate relative to the remnant small bowel. Relative to control IL in children [8], the median small bowel growth rate relative to age in these patients was 1.3-fold (range, 0.3–45.8-fold) (Fig. 2A). The growth rate of the remnant small bowel according to age was significantly lower in the TCA than in the non-TCA group (TCA group vs. non-TCA group, 78.6% vs. 129.7%; p=0.01) (Fig. 2B).
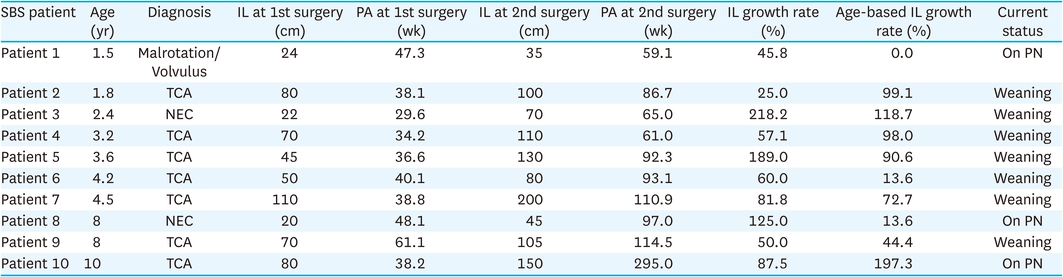
Table 2
Small intestinal length change of patients
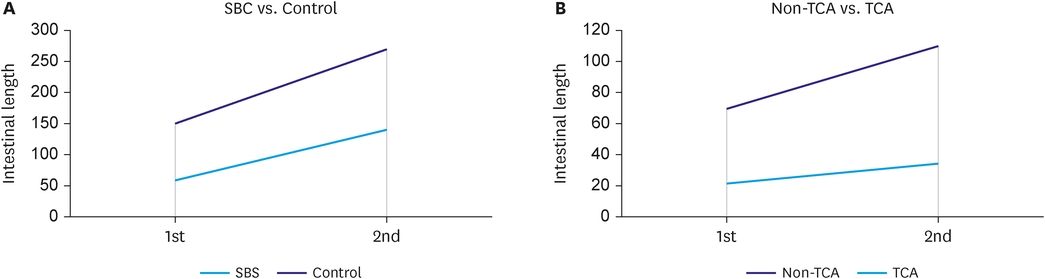
Fig. 2
Exploring small bowel growth patterns. (A) Small bowel growth rate relative to age in SBS. (B) Small bowel growth rate of non-TCA and TCA.
IL, intestinal length; SBS, short bowel syndrome; TCA, total colonic aganglionosis.
Of the 10 patients in the study, seven patients (70.0%) were weaned from PN (Table 2). Weaning from PN was not significantly associated with TCA (p=0.1). Out of the patients who failed to wean off PN, two patients had the shortest remnant small bowel. We did not find a statistically significant correlation between the proportion of remnant small bowel and weaning off PN (p=0.06).
SBS in children is a chronic condition, requiring long-term, complex care, with high morbidity and mortality rates. Common causes of SBS in pediatrics include midgut volvulus, necrotizing enterocolitis, multiple intestinal atresia, gastroschisis, and TCA [6, 11, 12, 13]. These patients are likely to have various complications, such as liver disease, sepsis, and renal complications, due to prolonged PN and frequent hospitalization [2], resulting in a mortality rate of 40% [11, 12, 14]. Other common complications depend on the remaining intestinal length and nature. Fluid and electrolyte abnormalities, micronutrient deficiencies, bacterial overgrowth, malabsorptive diarrhea can occur in children with SBS [1]. They need careful monitoring and treatment to follow the growth curve. Compared to adults, infants and children need significantly more calories and nutrients for normal growth and development. This increased caloric requirement appears to be a contributing factor in the intestinal failure associated liver disease. Intestinal adaptation is essential in the medical or surgical management of SBS.
Intestinal adaptation is critical for achieving independence from PN. Bowel adaptation depends on multiple factors, such as remnant IL, the presence of terminal ileum, diseases underlying SBS, age, lack of a colon, gut hormones, and growth factors. The most important factor is IL, with PN duration being inversely associated with IL [1, 6, 7, 8]. Intestinal adaptation starts within a few hours after intestinal resection, as several genes are expressed in the remnant intestine. Adaptation is generally complete within 24 to 60 months [15, 16]. Structural increases in villous height and crypt depth lead to increased absorption and digestion of nutrients [5, 17, 18]. Moreover, the remnant intestine increases in length, albeit slowly, over time. Animal studies have shown that hormones increase small IL, mucosal height, and villus height [5, 19]. The study demonstrated that hormones such as growth hormone, insulin-like growth factor-1, and epidermal growth factor had been shown to enhance the rates of enterocyte proliferation after small bowel resection. In our study, we found that the IL growth rate of SBS patients was higher than in normal healthy pediatric patients of the same age, which was shown in Struijs et al. [8]. This might have been caused by adaptation after small bowel resection.
Multidisciplinary approaches in medical, surgical, and nutritional care have resulted in survival benefits to children with SBS. The STEP procedure, a surgical method of bowel lengthening, can improve the incidence of PN weaning from 38% to 68% [20]. However, the ideal candidate for this procedure remains unclear because the extent of bowel lengthening in patients with the shortest bowel length is undetermined. In addition, limited data are available to explain that bowel lengthening is effective for patients with the shortest bowel lengths. In the previous study, Javid et al. [20], the patients who benefited the most from the STEP procedure were those patients with the longest bowel lengths and children who were tolerating a reasonable percentage of enteral nutrition before bowel lengthening. Similarly, in our study, four patients (patient #1, #3, #8, #10) who had done STEP procedure to elongate bowel length, only one patient had the independence of weaning off PN and did not to the rest.
The difference in IL growth rate between the TCA and non-TCA groups may be associated with the pathophysiology of TCA. Despite surgical resection of the aganglionic bowel, 40% of patients with Hirschsprung’s disease were shown to experience recurrent Hirschsprung’s-associated enterocolitis (HAEC) [21]. The change in gut microflora is a major etiological cause of significant recurrent HAEC, and intestinal dysbiosis is a significant risk in adaptation [5, 7, 22, 23]. In addition, reduced bacterial diversity is associated with an increased relative abundance of proteobacteria and bacteroids, comprising only a minor proportion of gut flora in healthy individuals [7, 22]. Intestinal dysbiosis may play a role in disrupting the intestinal epithelial barrier, allowing for bacterial translocation and contributing to chronic low-level inflammatory conditions such as in patients with inflammatory bowel disease and infants with necrotizing enterocolitis [22, 24, 25]. Children with SBS may be at risk of chronic malnutrition due to their inability to tolerate enteral nutrition. Enteral nutrition plays a significant role in stimulating the secretion of trophic hormones and signaling molecules such as insulin-like growth factor, glucagon-like peptide-2, epidermal growth factor, leptin, thyroxine, and corticosteroids, with intestinal dysbiosis eventually affecting adaptation including intestinal elongation [5].
Furthermore, segmental dysmotility in TCA patients is likely to affect intestinal elongation because intraluminal nutrients may reduce direct contact with epithelial cells. Four of the seven patients with TCA in our study underwent stomal revision due to dysmotility more than once, with the small bowel growth rate/estimated proportion of small bowel in three of these patients being relatively low (range, 0.3–2.1).
In addition to the remnant IL, many factors that affect the weaning off PN, such as colonic length, loss of the ICV, sepsis, cholestasis, gestational age, are known [26, 27, 28, 29]. Conservation of the colon is associated with a lower dependency on PN, as absorption of water, electrolytes, some nutrients, maintaining a normal rate of gastric emptying of liquids, and stimulating small intestinal hyperplasia [3, 28, 30]. The previous studies have reported better intestinal rehabilitation in SBS patients with an intact ICV [3, 26]. A preserved ileogastric reflex and the resulting slower transit of luminal contents through the distal ileum are likely contributory. TCA group did not preserve ICV and colon in our study, but all but one achieved independence from PN and successful intestinal rehabilitation. On the contrary, two of three patients in the non-TCA group failed to achieve independence from PN. As to the growth rate of the remnant small bowel according to age, the non-TCA group has a higher growth rate than the TCA group, but the remnant IL itself is short. The previous study found that the remnant IL less than 10-25% of the expected length of age was the strong negative predictor of intestinal rehabilitation [1, 26].
This study has several limitations in addition to the small number of patients in a retrospective review. Individual patient factors such as terminal ileum, age, lack of a colon in TCA, gut hormones, and growth factors may have affected our clinical results. There was also a significant difference in the number of diseases within each group in this study because of the nature of the disease that required corrective surgery; that is, TCA had more opportunities to identify IL changes than non-TCAs. The data may have been affected by differences among operators because the patients underwent a number of surgeries in addition to taking length measurements. Moreover, a small sample size, especially the non-TCA group, could make a bias to define the effect of the underlying disease on the growth of IL or achieving enteral autonomy. Lastly, the lack of research on the difference in intestinal elongation in patients with different underlying diseases suggests the need for follow-up studies involving larger numbers of patients and multiple centers.
In conclusion, to our knowledge, this study is the first to compare intestinal elongation rates between children with SBS and control children of similar age. We deduced that children with SBS grow rapidly in their IL faster than children of similar age through the process of intestinal adaptation. Furthermore, we found that TCAs underlying SBS had a lower growth rate of IL than non-TCAs. Given the nature of TCA, the management of SBS with TCA may be considered differently from other underlying diseases. With a better understanding of the biological differences between underlying diseases, we could develop a rehabilitation program for SBS in the future.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: C.Y.J., K.D.Y.
Data curation: C.Y.J., K.H., K.Y.J., K.S.C., K.D.Y., N.J.M.
Investigation: C.Y.J., K.H., K.Y.J., K.S.C., K.D.Y., N.J.M.
Writing - original draft: C.Y.J., K.D.Y.
