

Obscure gastrointestinal bleeding (OGIB) from the small bowel is difficult to diagnose, especially in children. We report a 10-year-old boy who presented sudden onset of severe anemia with massive OGIB who had a history of total gastrectomy in the neonatal period. Abdominal computed tomography, esophagogastroduodenoscopy, colonoscopy, Meckel's diverticulum scan, superior mesenteric arteriography, and celiac arteriography found no definite bleeding focus. Finally, capsule endoscopy revealed numerous vascular ectasias and multiple bleeding foci at jejunoileal region. With laparotomy and manual milking up of the small bowel by the surgeon, intraoperative endoscopy with argon plasma coagulations and hemo-clippings were done by the gastroenterologist, successfully. Intraoperative endoscopic management seems to be the treatment of choice for preventing massive unnecessary bowel resection. Here, we report a patient with OGIB, 10 years after gastrectomy for spontaneous rupture of stomach in the neonate period, which was diagnosed and managed successfully with a multiteam approach.
Obscure gastrointestinal bleeding (OGIB) from the small bowel is difficult to diagnose, especially in children. We report a 10-year-old boy who presented sudden onset of severe anemia with massive OGIB who had a history of total gastrectomy in the neonatal period. Abdominal computed tomography, esophagogastroduodenoscopy, colonoscopy, Meckel's diverticulum scan, superior mesenteric arteriography, and celiac arteriography found no definite bleeding focus. Finally, capsule endoscopy revealed numerous vascular ectasias and multiple bleeding foci at jejunoileal region. With laparotomy and manual milking up of the small bowel by the surgeon, intraoperative endoscopy with argon plasma coagulations and hemo-clippings were done by the gastroenterologist, successfully. Intraoperative endoscopic management seems to be the treatment of choice for preventing massive unnecessary bowel resection. Here, we report a patient with OGIB, 10 years after gastrectomy for spontaneous rupture of stomach in the neonate period, which was diagnosed and managed successfully with a multiteam approach.
Jejunoileal bleeding in children with no history of trauma is extremely rare. Finding the bleeding foci in the jejunoileal region and managing the bleeding is challenging because of the length, tortuosity, and anatomic location of the region [1]. Ten years after a neonate underwent gastrectomy for spontaneous rupture of the stomach, the patient presented with massive jejunoileal bleeding, which was diagnosed and managed successfully through a multiteam approach.
A 10-year-old boy was admitted with the chief complaints of sudden onset of pallor and weakness after fasting of 2 meals with preceding history of intermittent abdominal pain and tarry stools for several days. He has been on vitamin B12 injection treatment for intrinsic factor deficiency every 2–3 months since the neonatal period.
The boy was admitted with a sudden onset of pallor and weakness after several days of intermittent abdominal pain and refusal to eat 2 meals. He had been born at 35 weeks of gestational age by cesarean section after prelabor rupture of membranes; birth weight was 2,570 g, length was 48 cm, and head circumference was 33.9 cm. His Apgar scores were 8 at 1 minute and 10 at 5 minutes. On the second day after birth, he appeared lethargic, pale, and weak, with scanty urination and abdominal distension. Simple abdominal radiographs showed free air in the abdominal cavity, and ultrasonography showed bilateral hydronephrosis. Emergency exploratory laparotomy revealed gastric perforation with residual necrotic material from the fundus to the antrum. Total gastrectomy and Roux-en-Y esophagojejunostomy were performed. Biopsy revealed extremely thin anterior wall of the gastric body and antrum and 2 perforations. With total parenteral nutrition (TPN) and supportive care, the patient's postoperative course was uneventful. Vitamin B12 injections for intrinsic factor deficiency were administered every 2–3 months thereafter. In addition, the parents were advised to feed him frequently in small amounts. According to his growth chart over the next 10 years, his weight was in the third to fifth percentiles, and height in the fifth to tenth percentiles. For intermittent mild anemia, he received iron supplementation.
On admission, his temperature was 36.7°C; heart rate, 100 beats/minute; respiratory rate, 24 breaths/minute; and blood pressure, 110/60 mmHg. His weight was 25.8 kg (fifth percentile), and his height was 131.2 cm (tenth percentile). On physical examination, he was pale, the conjunctivae were pale, the abdomen was soft and flat with no tenderness, and bowel sounds were audible. The liver and spleen were not palpable. Laboratory findings were as follows: white blood cell count, 7.22×103/µL; hemoglobin level, 4.9 g/dL; hematocrit, 14.7%; reticulocyte count, 7.22%; platelet count, 280×103/µL; mean corpuscular volume, 86.0 fL; mean corpuscular hemoglobin level, 28.7 pg; and mean corpuscular hemoglobin concentration, 33.3 g/dL. The stool was positive for occult blood, with more than 1,200 ng/mL (normal, 0–100 ng/mL).
Transfusions of packed red blood cells were followed by efforts to locate the bleeding focus. Abdominal computed tomography revealed no bleeding focus; esophagogastroduodenoscopy (EGD) demonstrated no bleeding in the esophagus or jejunojejunostomy site; colonoscopy yielded normal findings; and a Meckel scan with technetium-99m pertechnetate demonstrated focal tracer uptake in the left upper quadrant of the abdomen. However, we could rule out Meckel's diverticulum since previous EGD showed normal findings.
Capsule endoscopy (CE) with the PillCam (26.2×11.4 mm; Medtronic, Dublin, Ireland) revealed multiple focal lesions of vascular ectasia (angiodysplasia) with active bleeding throughout the jejunum and ileum (Fig. 1). Arteriography of the superior mesenteric and celiac arteries was attempted for embolization; however, the bleeding foci were not visualized.
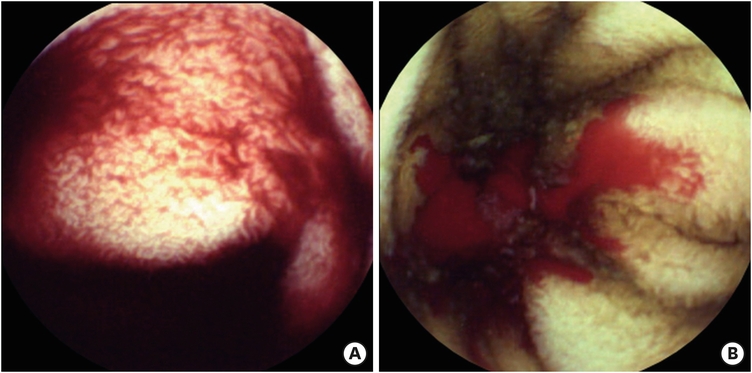
Fig. 1
Capsule endoscopy. (A) Numerous vascular ectasias were visualized throughout the small bowel (jejunum, ileum) and (B) multiple bleedings from vascular ectasias.
Exploratory laparotomy with intraoperative push-endoscopic bleeding control revealed multiple adhesive bands on the small bowel, and adhesiolysis was performed. Vascular anomalies such as angiodysplasia or hemangioma were not found in the mesentery including the serosa side of the bowel. After inspection of the intra-abdominal cavity, the gastroenterologist examined the whole small bowel by oral intubation with colonoscope (EVIS EXERA II® CF-Q180AL, working length 1,680mm; Olympus America, Center Valley, PA, USA). While the gastroenterologist inspected the small bowel mucosa, the surgeon performed gentle manual milking of the small bowel down to the ileocecal valve. Multiple mucosal bleeding foci were found from the proximal jejunum to the proximal ileum. There were no visible blood clots suspicious of bleeding at the opening site of jejunojejunostomy. Hemo-clippings were applied in 10 places, and argon plasma coagulations (APCs) were performed 34 times (Fig. 2).
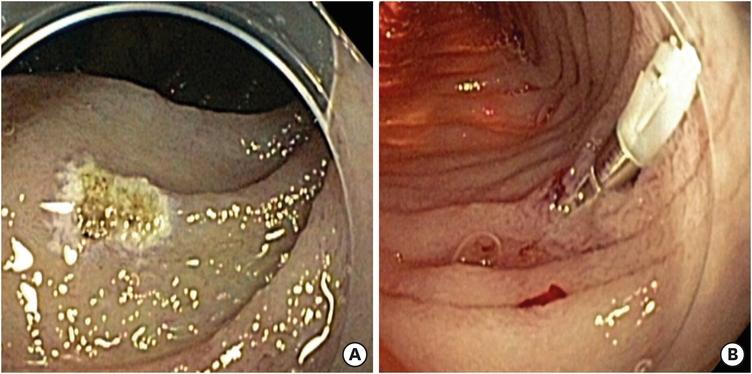
Fig. 2
Intraoperative endoscopy. Multiple bleeding foci were treated with (A) argon plasma coagulations and (B) hemo-clippings.
The postoperative course was uneventful; TPN and supportive care were administered. Simple abdominal X-rays were taken for 3 days and they showed a resolving paralytic ileus pattern. Hemoglobin levels were followed up every 1 to 2 months and remained normal. It was 3 years after the procedure when the hemoglobin level dropped to 9.7 g/dL from 11.0–12.0 g/dL with negative stool occult blood. Dietary history revealed inappropriate dietary intake of poorly balanced meals with parental neglect. After dietary counseling with dietician and physician regularly, hemoglobin levels steadily rose to over 11.0 g/dL and recent levels remain over 13.0 g/dL. Five-year follow-up CE revealed hypertrophied microvilli but no bleeding focus.
This case was reviewed and approved by the Institutional Review Board (IRB) of Daegu Fatima Hospital (IRB No. DFE20ORIO085-R1). The requirement for informed consent was waived after reviewing of IRB because it was practically impossible and this study was retrospective design.
The etiology of neonatal gastric perforation remains unclear. Terui et al. [2] reported that no factors were observed that could have caused neonatal gastric perforation other than malformations associated with distal obstruction in 5 of 11 cases. The causes of neonatal gastric perforation remain controversial. Congenital defect of the musculature of the perforated gastric wall, high gastric acidity in combination with local ischemia, and increased gastric pressure due to distal gastrointestinal anomalies those evoke gastric outlet obstruction are possible mechanisms [3].
Obscure gastrointestinal bleeding (OGIB) accounts for approximately 5% of all cases of gastrointestinal bleeding in adults [4, 5], as well as 5% in pediatrics [6]. OGIB is the most common indication for CE, which has been used worldwide for diagnosing OGIB [7], with high rates of detection (41.6%–61.4%) and low retention rates (0%–5%) [8]. In our patient, bleeding foci did not appear on conventional EGD or colonoscopy, but were found on CE.
Recent studies show that angiodysplasia was mainly found in the small bowel [9]. DeBenedet et al. [10] reported their cases of 114 patients with angiodysplasia in the gastrointestinal tract that showed 32% in the stomach, 50% in the duodenum, 37% in the jejunum, 15% in the ileum, and 44% in the colon. The pathogenesis of angiodysplasia remains unclear. Elevated levels of vascular endothelial growth factor may result in mucosal hypoxia [11], and chronic obstruction at the submucosal level creates pressure on the vessels of the submucosa, which results in their dilatation [11]. A history of prior bowel surgery could be related to the development of angiodysplasia. The usual diagnostic tools are generally unsuccessful in identifying these lesions. Angiography is rarely positive. Instead, most small bowel vascular lesions require enteroscopy or CE for identification. In cases of severe hemorrhage requiring emergent operative intervention, intraoperative endoscopy may be helpful. These lesions have a high rebleeding rate, and segmental small bowel resection might be required [12].
Small bowel bleeding can be treated with push enteroscopy, deep enteroscopy, spiral enteroscopy, intraoperative endoscopy, and surgical resection [13]. Our team performed intraoperative endoscopy because the patient had previously undergone gastrectomy; adhesions were expected in the small bowel, and checking the entire small bowel by other methods would have been difficult. With the multiteam approach, the gastroenterologist carefully searched for angiodysplasia and bleeding foci, simultaneously applying multiple hemo-clippings and numerous treatments with APCs. This was possible only because the surgeon manually milked the small bowel gently down to the ileocecal valve. In this way, diffuse and multiple mucosal angiodysplasia and active bleeding areas could be treated successfully without resection of the jejunum or ileum.
These processes were possible in close cooperation with multiple specialists: diagnostic approach and supportive care by the pediatrician, endoscopic management by the gastroenterologist, and surgical management by the pediatric surgeon. Three specialists' dedicated and continuous discussion and simultaneous cooperative management made the complicated patient's treatment successful. We would like to emphasize the importance of a multiteam approach for the OGIB especially for the massive jejunoileal bleeding in a child.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.I., K.H., K.W.D., H.J.O.
Investigation: J.J., K.I., K.H., H.J.O.
Writing - original draft: J.J., H.J.O.
Writing - review & editing: H.J.O.
