

Catecholamine-producing tumors are rare, and the classical symptoms include maintained or paroxysmal hypertension, headaches, palpitations and sweating. However, its symptoms can vary greatly, which is why it has been called “the great masquerader.” We are reporting case of a patient with a left adrenal pheochromocytoma with multiple abdominal paragangliomas who presented with severe ischemic involvement of both the upper and lower limbs due to catecholamine induced vasospasm.
Catecholamine-producing tumors are rare, and the classical symptoms include maintained or paroxysmal hypertension, headaches, palpitations and sweating. However, its symptoms can vary greatly, which is why it has been called “the great masquerader.” We are reporting case of a patient with a left adrenal pheochromocytoma with multiple abdominal paragangliomas who presented with severe ischemic involvement of both the upper and lower limbs due to catecholamine induced vasospasm.
Catecholamine-producing tumors are rare and called pheochromocytomas when their origin is intra-adrenal and paragangliomas (PPGLs) when they are extra-adrenal [1]. The classical symptoms of pheochromocytoma include maintained or paroxysmal hypertension, headaches, palpitations and sweating. However, its symptoms can vary greatly, which is why it has been called “the great masquerader” [2].
We are reporting case of a patient with a left adrenal pheochromocytoma with multiple abdominal PPGLs who presented with severe ischemic involvement of both the upper and lower limbs due to catecholamine induced vasospasm and internal jugular vein (IJV) thrombosis.
A 13 years boy presented in our emergency room with altered sensorium, hypertensive crisis, peripheral ischemia and breathlessness. Patient was in his usual state of health till 9 years of age. Then he started having symptoms of pain in left lower abdomen, nausea, vomiting and headache. He was diagnosed with hypertension and was started on antihypertensives by a physician. After an uneventful period of about 4 years with intermittent episodes of headache, excessive sweating and pain abdomen patient developed chest pain and dyspnea. During this episode echocardiography showed a decreased left ventricular ejection fraction (LVEF) of 20%. Two weeks back patient developed features of acute abdomen with blackening of fingers and toes (Fig. 1 and B) along with altered sensorium and visited us. His blood pressure (BP) was very high (210/120 mmHg) and heart rate was 180 per minute. Classical history of headache, palpitations and sweating along with hyper-enhancing mass on contrast enhanced computed tomography (CECT) suggested the diagnosis of PPGL syndrome. There was no history of any similar kind of illness in any other family member. He was admitted in intensive care unit and emergent hypertensive crisis management was started. Patient was started on alpha blocker—prazosin 5 mg once daily and gradually increased to 25 mg per day, nifedipine 10 mg twice daily per day. Beta blocker (Metoprolol 150 mg daily) was added after 5 days of alpha blocker therapy. With this his symptoms subsided and peripheral ischemia resolved. His further evaluation revealed very high plasma free normetanephrine (4,668 pg/mL), normal plasma free metanephrine (46 pg/mL), normal serum calcitonin (2 pg/mL) and normal serum calcium (8.4 mg/dL). Triple phase CECT abdomen showed hyper-enhancing tumors at left suprarenal, right perihilar, inter-aortocaval and organ of Zuckerkandl locations (Fig. 2A-D). CECT done for screening of von Hippel Lindau syndrome revealed left IJV thrombosis and thrombosis of segmental branches of left pulmonary artery (Fig. 2E and F).

Fig. 1
(A, B) Showing peripheral ischemia of upper and lower limbs. (C) Follow up picture after 6 weeks showing completely resolved ischemia.
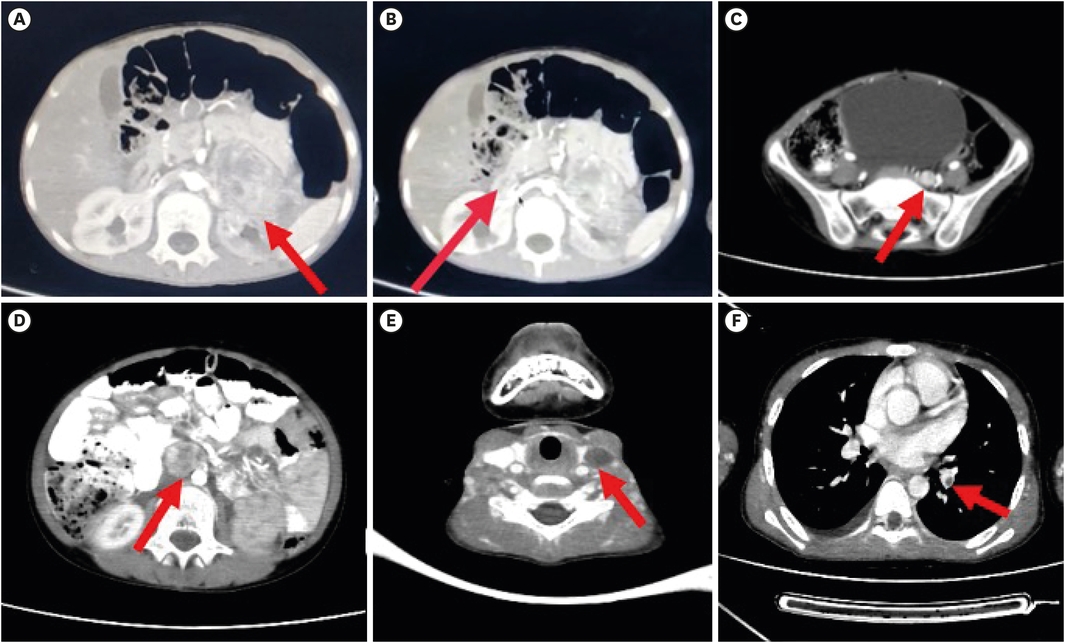
Fig. 2
CECT abdomen axial images showing (A) enhancing mass in left suprarenal location extending anterior to left kidney (arrow). (B) Another enhancing lesion noted at right renal hilum (arrow). (C) Enhancing lesion noted anterior to left sacral ala adjacent to left iliac vessels (arrow). (D) Enhancing mass noted in inter-aortocaval location (arrow). (E) Axial CECT neck showing left IJV thrombosis (arrow). (F) Axial CECT thorax showing thrombosis in segmental branch of lift pulmonary artery (arrow).
CECT, contrast enhanced computed tomography; IJV, internal jugular vein.
After adequate pre-operative preparation and alpha blockade therapy for 2 weeks, he was operated under general anaesthesia. Midline incision was placed. Intra-operatively left adrenal pheochromocytoma was densely adhered with left kidney and renal vessels, this was dissected off and left kidney preserved. A 2×2 cm right perihilar, two 2×2 cm inter-aortocaval tumors densely adhered with precaval fascia, one 1.5×1 cm organ of Zuckerkandl paragangliomas were excised (Fig. 3). Patient had BP fluctuation and highest systolic BP went up to 220 mmHg for which nitroglycerin infusion was started. After removal of all the tumors child developed hypotension (systolic BP 60 mmHg) and nor-epinephrine support was required for 4 hours post-operatively. Post-operative course was uneventful, and the patient was discharged on post-operative day 5. During follow up it was observed that the peripheral ischemia had resolved (Fig. 1C) and his BP was normal without any medication. Lymph nodal architecture was not seen in any of the excised PPGLs. Hence, final histopathology report was suggestive of left adrenal pheochromocytoma and multiple PPGLs. His LVEF improved to 45% after 6 months of surgery. Hormonal pattern along with multiple intra-abdominal PPGLs suggest a genetic susceptibility. MEN2 related features were absent in family members and physical examination was normal. However, due to financial constraints, we were not able to perform genetic testing. We are arranging financial help for him for genetic testing and Ga-68 DOTANOC positron emission tomography scan.
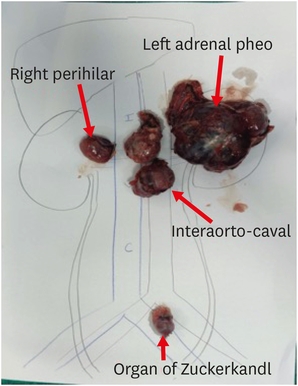
Fig. 3
Photograph of excised tumors.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent obtained from the parent of the child. This was approved by the Institute Ethics Committee of NSCB Medical College (IEC Apr-00/2021).
PPGLs are called the great mimic or the great masquerader as they can present with a myriad of clinical symptoms. However, a pediatric patient with peripheral vascular ischemia and IJV thrombosis has not been reported previously. Our extensive review of English language literature revealed around 15 cases of PPGL presenting as peripheral ischemia reviewed by Rios et al. [3]. Ours is first patient in pediatric age group and second patient having both upper and lower limb ischemia. We could not identify any case reporting IJV thrombosis.
The pathophysiology of peripheral ischemia in PPGLs is related to catecholamine induced vasoconstriction rather than any baseline condition [4]. Pre-existing peripheral vasculopathy and prolonged hypotension can increase the risk of catecholamine induced digital necrosis. In our young patient, however, there was no history of peripheral vasculopathy and systolic BP remained at ≥120 mmHg almost constantly throughout his hospital stay. This suggests that it was a pure manifestation of catecholamine excess induced vasoconstriction.
The simultaneous occurrence of PPGLs and inferior vena cava thrombosis is reported sporadically [5, 6]. Our patient had left IJV thrombosis and left main pulmonary artery thrombosis. The relationship between cancer and thrombosis has been extensively described [7]. However, this case turned out to be a benign PPGL. A bland thrombus in any vessel could be due to hypercoagulable status of the patient, stasis of blood due to obstruction, and trauma to the vessel as described by Virchow [8]. Our patient did not have any hypercoagulable state or obstruction. Hence, sustained hypertension leading to vascular endothelial injury is most plausible explanation in our patient. Important point to note here is that IJV thrombosis in a young hypertensive patient can be an indicator of PPGL.
In conclusion, pheochromocytomas and PPGLs have a wide variety of presentation. Symptoms and signs of peripheral vascular disease and or thrombosis in a young hypertensive patient should raise the suspicion of pheochromocytoma-PPGL.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: Y.S.K.
Data curation: Y.S.K.
Formal analysis: Y.S.K.
Investigation: Y.S.K.
Methodology: Y.S.K.
Writing - original draft: Y.S.K.
Writing - review & editing: A.N., S.R., Y.N., S.A.
