

Purpose
Enterostomies in premature infants are associated with a high incidence of complications. This study analyzed the factors associated with complications in very low birth weight (VLBW) infants who underwent enterostomy.
Methods
VLBW infants with preoperative weights below 1,500 g who underwent enterostomy between January 2003 and May 2018 were analyzed. The gestational age, corrected age, birth weight, weight at the time of surgery, surgery location, causative disease, laboratory findings, and complications were also analyzed.
Results
A total of 61 cases were included, consisting of 16 cases with stomal complications (26.2%); 12 prolapses (19.7%), 3 cases of parastomal hernias (4.9%), and 1 case of prestomal obstruction (1.6%). Premature infants born before 28 weeks gestation had approximately a three-fold increase in complications, albeit without statistical significance (p=0.11). These infants also had high incidences of bedside operations (p=0.003). Differences in surgical sites did not significantly impact the complication rate. Seven patients (11.5%) underwent reoperation for their complications. Twelve patients had prolapses, and six of these patients (50%) underwent reoperative surgeries. The mortality rate among the included patients was 24.6% (15 patients). These deaths were not associated with enterostomy, and seven deaths (46.7%) were attributed to neonatal sepsis and necrotizing enterocolitis.
Conclusion
VLBW infants, particularly those born before 28 weeks of gestation, typically have stomal complications. Therefore, surgical techniques should be aimed at minimizing stomal complications when operating on VLBW patients.
Enterostomies in premature infants are associated with a high incidence of complications. This study analyzed the factors associated with complications in very low birth weight (VLBW) infants who underwent enterostomy.
VLBW infants with preoperative weights below 1,500 g who underwent enterostomy between January 2003 and May 2018 were analyzed. The gestational age, corrected age, birth weight, weight at the time of surgery, surgery location, causative disease, laboratory findings, and complications were also analyzed.
A total of 61 cases were included, consisting of 16 cases with stomal complications (26.2%); 12 prolapses (19.7%), 3 cases of parastomal hernias (4.9%), and 1 case of prestomal obstruction (1.6%). Premature infants born before 28 weeks gestation had approximately a three-fold increase in complications, albeit without statistical significance (p=0.11). These infants also had high incidences of bedside operations (p=0.003). Differences in surgical sites did not significantly impact the complication rate. Seven patients (11.5%) underwent reoperation for their complications. Twelve patients had prolapses, and six of these patients (50%) underwent reoperative surgeries. The mortality rate among the included patients was 24.6% (15 patients). These deaths were not associated with enterostomy, and seven deaths (46.7%) were attributed to neonatal sepsis and necrotizing enterocolitis.
VLBW infants, particularly those born before 28 weeks of gestation, typically have stomal complications. Therefore, surgical techniques should be aimed at minimizing stomal complications when operating on VLBW patients.
Enterostomies are primarily performed on neonates during emergencies. The survival rate of very low birth weight (VLBW) infants increases with neonatal intensive care [1, 2]. However, the incidence of gastrointestinal complications, including necrotizing enterocolitis (NEC), focal intestinal perforations (FIPs) [3, 4, 5], and meconium obstruction [6], also increases. Therefore, enterostomies in VLBW infants steadily increase. Previous studies have shown that the incidence of complications associated with enterostomies in neonates is approximately 18%–68% [7, 8, 9, 10]. Multiple studies have shown that low preoperative weight and gestational age are significant risk factors for enterostomy-related complication [8, 9]. Therefore, in this study, we analyzed postoperative enterostomy-related complications and factors influencing complications in VLBW infants.
Medical charts for VLBW infants (body weight <1,500 g), who underwent enterostomies between January 2003 and May 2018 at our institution, were postoperatively reviewed.
Enterostomies were created at incision sites via four-directed anchoring of the bowel wall and fascia using PDS 5-0. Two additional anchoring sutures were placed in the upper part of weak tissues.
Patient demographics, including gestational age, birth weight, and comorbidities, were extracted from the charts. Perioperative data, including corrected age, preoperative weight, operation duration, causative disease, laboratory findings (such as complete blood count, C-reactive protein, and blood gas analysis) within 24 hours of surgery, surgical theatre, type of enterostomy, and surgical complications associated with the enterostomy were also extracted. NEC and FIP were classified as one group, among the causative diseases, based on similar first-line factors, signs, and symptoms [11].
Postoperative complications included herniation and stomal issues, such as retraction, prolapse, stricture, and necrosis. Strictures are defined as partial or complete mechanical obstructions requiring surgical intervention. The onset of complications was classified as “immediate” (<1 week postoperative), “early” (>1 week and <1 month postoperative), and “late” (>1 month postoperative) according to the time elapsed since the enterostomy was created.
The correlations among patient demographics, operative variables, and the occurrence of stomal complications were statistically analyzed using the χ2 test and Fisher’s exact test. Statistical significance was set at p<0.05.
All procedures involving human participants were in accordance with the ethical standards of the ethics committee of Asan Medical Center Children’s Hospital of Ulsan University and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board (IRB) of Asan Medical Center Children’s Hospital of Ulsan University (IRB No. S2018-2029-0001).
Sixty-one infants (39 males, 22 females) who underwent enterostomy were identified. Patient demographics are listed in Table 1. The median gestational age was 22.5 weeks (22.4–33.6), and the median birth weight was 720 g (280–1,500). The median preoperative chronological age was 9 days (1–184), whereas the median preoperative age was 27.3 weeks (24.3–37.3). The median preoperative weight was 780 g (390–1,490). Fifty-two patients (85.2%) required mechanical ventilation for pulmonary conditions, and 25 patients (40.9%) needed interventions, including surgery, for heart conditions. The causative diseases included NEC, FIP, and meconium plug syndrome (MPS); NEC/FIP had the highest incidence (51/61, 83.6%). Fifteen cases of neonatal mortality were noted. However, none of these deaths were associated with enterostomy, and approximately 50% were attributed to neonatal sepsis from NEC (7/15, 46.7%).
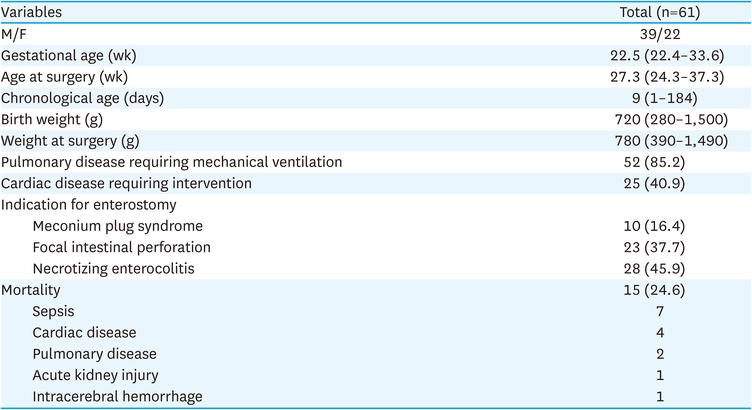
Table 1
Patient demographics
Features related to surgery are listed in Table 2. The median operation time was 56 minutes, and enterostomy creation was the only surgical procedure performed. The most frequent type of enterostomy was loop-enterostomy (46/60, 76.7%), followed by end-enterostomy (14/60, 23.3%) and double-barrel enterostomy (1/60, 1.6%). Sixteen patients showed stomal complications (26.2%), including parastomal hernias, stomal prolapses, and prestomal obstructions. The most frequent complication was stomal prolapse (12/61, 19.7%). The rate of reoperation was 11.5% (7/61), most commonly for stomal prolapses (6/12, 50%) and prestomal obstructions (1/1, 100%). Among the six patients who underwent reoperation for a prolapse, there were five cases of bowel necrosis and one case of take-down. Patient mortality was not associated with stomal complications.
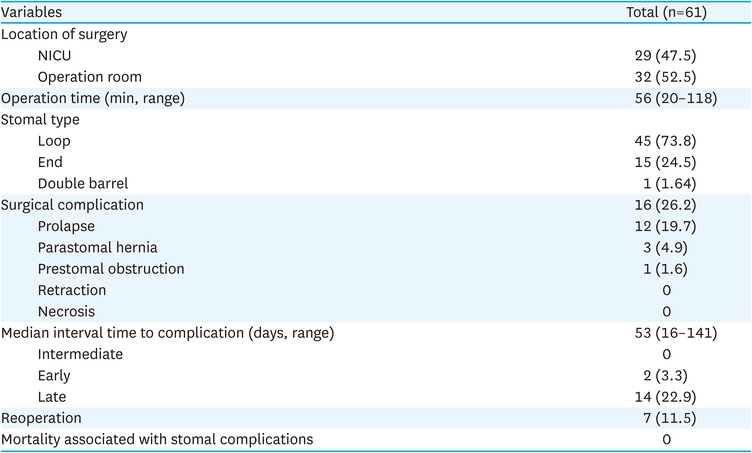
Table 2
Surgical features
Analyses of factors that might have influenced the occurrence of complications revealed no statistical significance (Table 3).
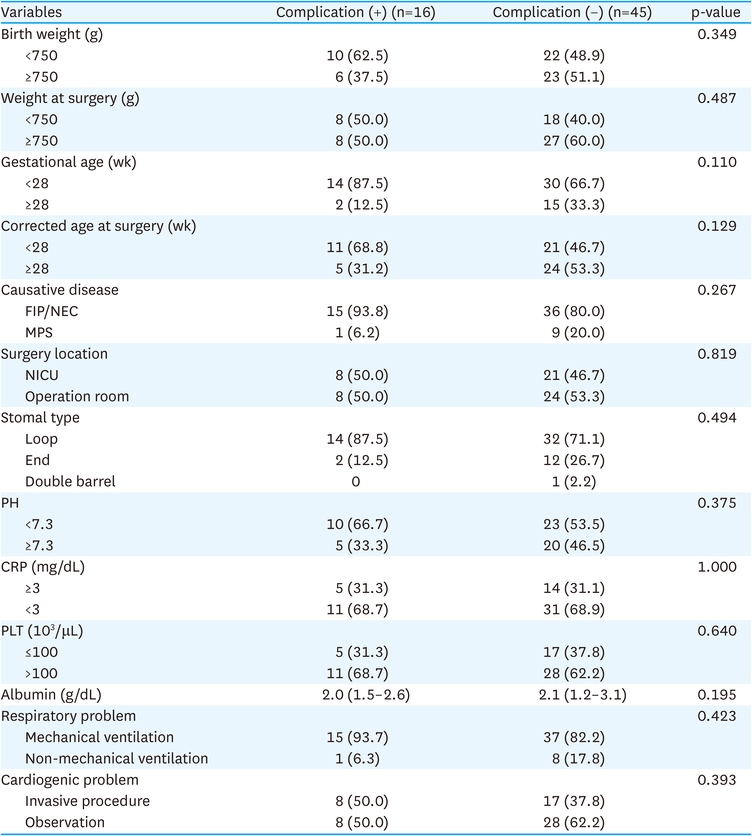
Table 3
Comparison between patients with and without complications
Enterostomy is performed in a wide variety of abdominal emergencies in pediatrics. In the current study, NEC, FIP, and MPS were causative diseases for enterostomies. These enterostomies led to complications, such as perforation or bowel necrosis.
The gold-standard treatment for bowel perforation or bowel necrosis is excision of the affected intestine and stoma creation [12, 13]. Although resecting bowel necrosis with enterostomy creation for decompression and diversion can be life-saving maneuvers [7], the stomal complication rates are higher in infants (25%–75%) than those in adults [14, 15]. O’Connor et al. [7] reported a 68% stoma-related complication rate in VLBW infants with NEC. Nour et al. [14] explained that the most reasonable explanation for this observation includes decompression of the obstructed distal bowel and improvement of intestinal edema after stoma creation. Steinau et al. [16] described increasing intra-abdominal pressure from crying in the case of a very young population as another etiological factor.
In our study, the enterostomy complication rate was 26.2%. These complications included prolapses, parastomal hernias, and obstructions. Although complication rates vary among studies, prolapse is consistently reported as the most frequent complication (9%–36%) [9, 14, 16, 17]; the findings of our study corroborate this (19.7%). Prolapse is mainly caused by elevated abdominal pressure when the surgical site on the intestine is too large or the length of the intestine is too long [9]. The abdominal walls of infants are weak, and in many cases, the intestines are enlarged or swollen during surgery. Therefore, appropriate-sized fascial defects may increase in size as ascites fail to resolve and a prolapse ensues. This complication is also related to the patient's prematurity. Other studies have also reported that low gestational age and preoperative weight can increase the likelihood of ostomy-related complications in VLBW infants [9, 17, 18]. Although there was no statistical significance, our study confirmed that patients with gestational age <28 weeks have significantly higher complications than those with gestational age >28 weeks (87.5% vs. 12.5%).
Correlations between the rate of complication and causative diseases are noteworthy. Although not statistically significant, the FIP/NEC group had thrice more complications than the MPS group. It is assumed that the extent and degree of the affected bowel were greater in FIP/NEC than those in MPS [16]. Factors, such as immature immunology and decreased metabolic response to surgery, also contributed to this. A previous study reported that the rate of neonatal sepsis associated with NEC was 26%–40% [19, 20]; this rate was higher than that in immunocompetent patients [21]. The high complication rate observed in premature infants may be attributed to the difficulties in maintaining appropriate metabolic responses to acute injury or immature immunological functions.
The overall incidence of complications in this study was lower than that of previous studies (26.2% vs. 20.8% to 100%). This might be related to the suture technique and nutritional care provided by the institution [7, 16]. In this study, the low incidence of prestomal obstruction (1%) represents improvements in suture technique. We performed a minimal anchoring technique to ensure minimal damage to the mesentery and small bowel. The median albumin concentration in infants who underwent surgery was 2.1 g/dL, which remained high compared to that reported in other studies [7]. The high albumin concentration was related to the efforts of the nutrition support team (NST) at our institution; the NST monitored the nutritional status of patients on a daily basis and provided adequate nutrition. The NST consisted of a pediatric surgeon or pediatric specialist, a specialist nurse, a nutritionist, and a pharmacist. Nutrition-related laboratory tests, including tests for trace elements, were performed regularly to provide patient-specific parental nutrition.
The study has some limitations owing to the retrospective nature of this review. Extracted data collected were not explicitly included in the study. Therefore, biases inherent in this methodology were introduced. In addition, the small sample size at a single institution hindered the ability to obtain statistical significance in some analyses.
Enterostomy might be a life-saving procedure in emergent situations for VLBW infants. As complications are frequently associated with the immaturity of VLBW infants and those with low gestational age, patients with low gestational age require much attention during enterostomy anchoring techniques and in the nutritional support provided to ensure optimal metabolic responses to surgery.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.Y., C.Y.J.
Data curation: C.Y.J., K.H., K.S.C., K.D.Y., N.J.M.
Formal analysis: K.D.Y.
Investigation: K.D.Y., C.Y.J.
Methodology: K.D.Y., C.Y.J.
Project administration: C.Y.J., K.H., K.S.C., K.D.Y., N.J.M.
Supervision: K.D.Y.
Validation: K.D.Y., C.Y.J.
Visualization: K.D.Y., C.Y.J.
Writing - original draft: C.Y.J.
Writing - review & editing: K.D.Y.
The authors would like to express their gratitude to those who participated in this project.
