

Purpose
Gastroesophageal reflux disease (GERD) frequently affects patients with esophageal atresia (EA). GERD is often resistant to medical therapy, and anti-reflux surgery in the form of fundoplication is required. However, there are no generally accepted indications for fundoplication in EA patients with significant gastroesophageal reflux (GER). This study aimed to report the outcomes and review the clinical characteristics and treatment of GERD with Nissen fundoplication among EA patients.
Methods
The medical records of patients with EA repair who underwent Nissen fundoplication for GERD treatment from January 2005 to December 2018 were retrospectively reviewed. Twenty patients were included in this study.
Results
In total, 166 patients with EA underwent treatment during the study period. Among these, 20 (12%) patients underwent Nissen fundoplication. The median age at the time of fundoplication was 5.3 (range, 1.6–49.4) months, and the mean body weight was 6.3±2.4 kg. The indications for Nissen fundoplication were hiatal hernia in 18 (90%) patients, feeding intolerance in 17 (85%), recurrent aspiration pneumonia in 13 (65%), GER-related refractory anastomosis stenosis in seven (35%), and reflux-related acute life-threatening events in five (25%). The median follow-up duration after Nissen fundoplication was 5.7 (range, 2.4–10.7) years; two (10%) patients experienced surgery-related complications, 11 (55%) had recurrent hiatal hernia, and three (15%) required re-operation. Feeding intolerance improved (p<0.001), and the number of esophageal dilatations decreased following Nissen fundoplication (p=0.038). There was no mortality during the follow-up period.
Conclusion
Nissen fundoplication was required in patients with more complicated EA and was performed at a young age. Nissen fundoplication was relatively effective in controlling EA-associated GERD. However, Nissen fundoplication in patients with EA may be associated with a high rate of recurrent hiatal hernia. A careful follow-up is necessary because poor long-term outcomes are common for such patients.
Gastroesophageal reflux disease (GERD) frequently affects patients with esophageal atresia (EA). GERD is often resistant to medical therapy, and anti-reflux surgery in the form of fundoplication is required. However, there are no generally accepted indications for fundoplication in EA patients with significant gastroesophageal reflux (GER). This study aimed to report the outcomes and review the clinical characteristics and treatment of GERD with Nissen fundoplication among EA patients.
The medical records of patients with EA repair who underwent Nissen fundoplication for GERD treatment from January 2005 to December 2018 were retrospectively reviewed. Twenty patients were included in this study.
In total, 166 patients with EA underwent treatment during the study period. Among these, 20 (12%) patients underwent Nissen fundoplication. The median age at the time of fundoplication was 5.3 (range, 1.6–49.4) months, and the mean body weight was 6.3±2.4 kg. The indications for Nissen fundoplication were hiatal hernia in 18 (90%) patients, feeding intolerance in 17 (85%), recurrent aspiration pneumonia in 13 (65%), GER-related refractory anastomosis stenosis in seven (35%), and reflux-related acute life-threatening events in five (25%). The median follow-up duration after Nissen fundoplication was 5.7 (range, 2.4–10.7) years; two (10%) patients experienced surgery-related complications, 11 (55%) had recurrent hiatal hernia, and three (15%) required re-operation. Feeding intolerance improved (p<0.001), and the number of esophageal dilatations decreased following Nissen fundoplication (p=0.038). There was no mortality during the follow-up period.
Nissen fundoplication was required in patients with more complicated EA and was performed at a young age. Nissen fundoplication was relatively effective in controlling EA-associated GERD. However, Nissen fundoplication in patients with EA may be associated with a high rate of recurrent hiatal hernia. A careful follow-up is necessary because poor long-term outcomes are common for such patients.
Gastroesophageal reflux (GER) is commonly encountered in patients with repaired esophageal atresia (EA) [1]. The cause of GER in EA revolves around the anatomical changes and abnormal innervation of the esophagus, resulting in lower esophageal sphincter dysfunction and esophageal dysmotility [2, 3, 4]. GER may cause vomiting, anoxic spells, recurrent aspiration pneumonia, and recurrent anastomotic strictures [5]. Post-anastomotic stricture is a common complication of repaired EA [6], and GER may exacerbate the anastomotic stricture [7]. Conservative management of GER after EA repair by positioning, anti-reflux medication, or waiting for the disappearance of the symptoms during infant growth may not be effective; thus, anti-reflux surgery is necessary in such cases [8]. Nissen fundoplication is the most common surgical procedure for treating gastroesophageal reflux disease (GERD). However, the incidence of GERD in repaired EA and the rate of fundoplication varies widely in the literature from 25% to 72% [5]. Additionally, previous studies have not reported consistent surgical outcomes for such patients [9, 10, 11]. Therefore, anti-reflux surgery to treat GERD in repaired EA cases remains debatable. Thus, this study aimed to review the clinical characteristics of GERD and the result of Nissen fundoplication in patients with repaired EA at our institution.
This retrospective follow-up study analyzed patients who underwent Nissen fundoplication after EA repair at the author’s institution between January 2005 and December 2018. During the study period, 166 children with EA were treated and followed. A total of 20 (12%) patients underwent Nissen fundoplication to treat GER. Medical records of patients with EA were analyzed retrospectively, and the patient’s demographic characteristics, treatments, and long-term prognoses were analyzed.
Patient data are presented as descriptive statistics, including frequencies, percentages, medians and ranges, and means and standard deviations. Two-sample t-tests, the Mann–Whitney U test, and the Wilcoxon signed-rank test were used to analyze data, with p-values <0.05 considered significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, version 23.0 (IBM Corp., Armonk, NY, USA).
This study was approved by the Institutional Review Board of Severance Children’s Hospital (#4-2021-1167). The requirement for informed consent was waived because of the study’s retrospective design.
The demographic characteristics of patients with EA are summarized in Table 1. A total of 166 patients underwent treatment for EA. The patients in terms of median gestational age was 38 weeks (range, 30–44 weeks), and the mean birth weight was 2.5±0.4 kg. The most common gross type of EA was C (n=142), followed by types A (n=21), B (n=1), and E (n=1). Of these 166 patients, 83 were transferred after repair at other hospitals. The number of complicated cases after EA repair was higher among the referred patients. Re-operation was performed in 25 (15%) cases (3 inside vs. 22 outside, p<0.001), and tracheomalacia (27 inside vs. 47 outside, p=0.002) was treated with aortopexy, which was more significant in referred patients (1 vs. 13, p<0.001). In addition, 20 (12%) patients underwent Nissen fundoplication, and more operations were performed among the referred patients (3 vs. 17, p<0.001).
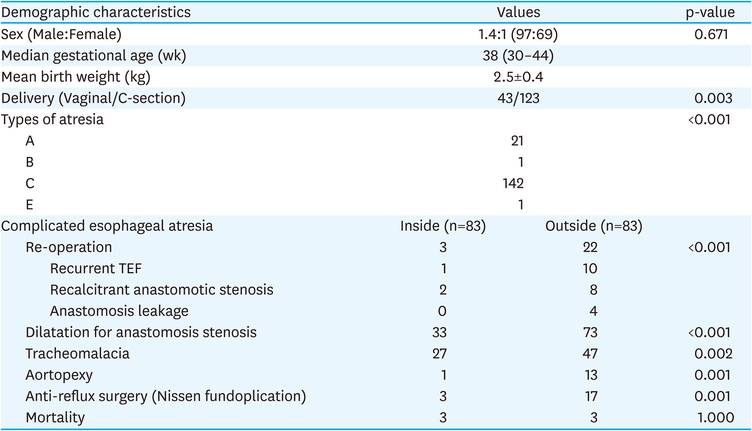
Table 1
Clinical and demographic characteristics of esophageal atresia (n=166)
The demographic characteristics of the patients who underwent Nissen fundoplication are summarized in Table 2. The median age at the time of operation was 5.3 (range, 1.6–49.4) months, and the mean body weight at operation was 6.3±2.4 kg. The Nissen fundoplication was performed in 14 (9.6%) of 144 patients with type C EA and six cases (27.3%) of 22 patients with type A EA. The difference was significant, as more Nissen fundoplication procedures were performed for type A EA cases (p=0.034). Among the combined anomalies were cardiac anomalies (required surgery) in six (30%) patients, gastrointestinal anomalies in three (15%), and anorectal malformation in three (15%). Pre-existing gastrostomy was performed in five (25%) cases and simultaneously in four (20%) cases. Of the 20 patients, 12 (60%), four (20%), and four (20%) patients underwent open, laparoscopic, and robotic surgery, respectively. The reason for Nissen fundoplication was hiatal hernia in 18 (90%) patients, feeding intolerance in 17 (85%), recurrent aspiration pneumonia in 13 (65%), GER-related refractory anastomosis stenosis in seven (35%), and a reflux-related acute life-threatening event (ALTE) in five (25%). The symptoms overlapped in each patient. The median follow-up duration was 5.7 (range, 2.4–10.7) years.
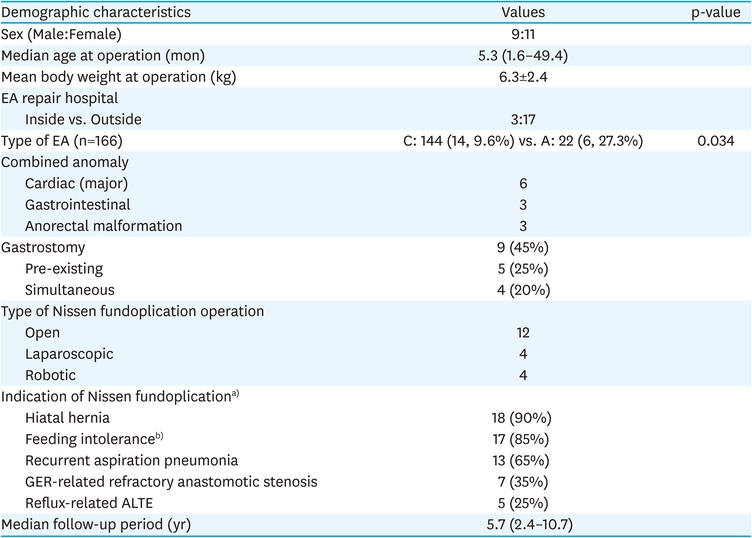
Table 2
Demographic characteristics of the patients who underwent Nissen fundoplication (n=20)
The surgical outcome of Nissen fundoplication is summarized in Table 3. The surgery-related complications occurred in two (10%) patients: one had delayed gastric perforation, and the other developed surgical wound infection. During the follow-up, 11 (55%) patients had recurrent hiatal hernia, and; three (15%) patients underwent re-operation because of progressive reflux symptoms. The median time to re-operation was 34.7 (1.6–77.7) months. The GERD-related complication was compared between pre- and post-Nissen fundoplication (Table 4). Feeding intolerance improved (p<0.001), and the number of esophageal dilatations reduced post-Nissen fundoplication (1.31 vs. 2.38, p=0.038). Recurrent aspiration pneumonia (2.85±2.7 vs. 3.6±3.8, p=0.096) and reflux-related ALTE (0.4±0.89 vs. 2.4±1.6, p=0.116) rates decreased after surgery, although the differences were not significant. Table 5 shows the characteristics of recurrent hiatal hernia. Compared with non-recurrent hiatal hernia patients, those with recurrent hiatal hernia who had undergone Nissen fundoplication were younger (4.9±1.6 months vs. 11.9±14.7 months, p=0.038) and had a lower body weight (5.7±1.6 kg vs. 6.9±3.1 kg, p=0.093). No significant difference was observed in the type of EA atresia, complicated EA, gastrostomy insertion, or the type of fundoplication procedure.

Table 3
Surgical outcomes of Nissen fundoplication (n=20)

Table 4
Comparison of GERD-related complications after Nissen fundoplication
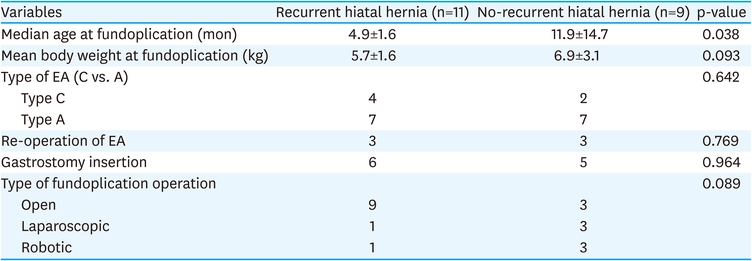
Table 5
Recurrent hiatal hernia
In this study, we aimed to evaluate the outcomes and review the clinical characteristics and treatment of GERD with Nissen fundoplication among patients with EA. We found that the rate of fundoplication in patients with EA was 12%, and the median age of patients at the time of surgery was less than one year. Primarily, anti-reflux surgery was more commonly performed in patients with complicated EA.
GERD following EA repair is a common complication, affecting over 50% of patients [12]. This pathologic entity poses an especially unique abnormal esophageal anatomy after EA repair. The repaired esophageal length is shorter and may displace the gastroesophageal junction upward, causing an obtuse angle of His. This condition is especially true in patients with long-gap atresia with significant anastomotic tension [10]. Therefore, in the case of pure and long-gap EA, the barrier mechanisms against reflux are even more damaged, and such patients might benefit from fundoplication [11]. Our findings suggest that the Nissen fundoplication was more common in EA type A than in type C (27.3% vs. 9.6%, p=0.034). In addition, of the 20 patients who had undergone Nissen fundoplication, 17 were referred from outside hospitals after EA repair. Most of the transferred patients were those who needed treatment for complications after EA repair or those with severe conditions. As evident from the study results, more re-operations of EA, tracheomalacia, and aortopexy were performed in referred patients. Furthermore, this is in line with the opinion that patients with complicated EA or difficult anastomosis more commonly require anti-reflux surgery.
GER can lead to recurrent respiratory tract infections, a life-threatening cyanotic spell, severe stenosis of the anastomosis, and failure to thrive [13]. Most of the symptoms associated with GER occur in combination, and some clinicians are not familiar with GER symptoms, resulting in delayed treatment. Similarly, as observed in our study, patients may have complex clinical features. The indications for Nissen fundoplication in patients with EA were reportedly recalcitrant anastomotic stenosis, an ALTE event, and recurrent respiratory symptoms [14]; poor nutrition, surgical anastomosis difficulties, and long-gap EA are predictive factors for early anti-reflux surgery in EA [15]. In our study, the surgical indications were similar to those from other reports. However, reflux can appear in combination with various symptoms. Therefore, clinicians should carefully determine whether the symptoms are caused by GER.
In previous studies, the rate of anti-reflux surgery after EA repair ranges from 23% to 73% [16, 17]. Approximately 12% of all patients with EA in our study underwent Nissen fundoplication, which is at the lower end of this range. In retrospect, we believe that the need for GERD treatment may have been underestimated for some patients in our study. Other studies have reported that the timing of anti-reflux surgery in patients with EA was very common before one year of age [8, 18, 19]. Similarly, in our study, the median age at operation was 5.3 months. These characteristics indicated that the repaired esophagus has more aggressive reflux symptoms than cases without anatomical abnormality, and anti-reflux surgery was performed even at a young age.
Among the complications occurring after EA surgery, anastomotic stenosis has a clinically adverse effect on prognosis. Dilatation is performed in 30%–60% of patients to treat anastomotic stenosis [18, 20]. A dilatation rate of 63% was observed in our study. Postoperative GER may exacerbate anastomotic strictures caused by a long gap, postoperative leaks, tension on the anastomosis, or tissue ischemia at the esophageal ends [6, 7]. Reflux of gastric contents may lead to mucosal irritation and peptic strictures and might also exacerbate inflammatory changes already present at the anastomosis site [21]. Anti-reflux surgery has been suggested for patients with recalcitrant anastomosis stenosis [22, 23]; however, its effectiveness has not been proven scientifically [11]. In our study, the need for dilatation procedures decreased significantly after Nissen fundoplication. However, there are multiple risk factors for esophageal stenoses such as long-gap EA with consequent anastomotic tension, postoperative anastomotic leakage, and GER [24, 25, 26]. Although fundoplication alone does not mean that the stenosis can be completely resolved, it is considered effective to some extent in treating recalcitrant anastomosis stenosis.
The recurrence rate of fundoplication disruption and recurrent reflux in patients with EA ranges from 20% to 45% [27, 28, 29]. This is significantly higher than those undergoing fundoplication without any underlying anatomic defects [28]. Furthermore, our findings revealed a high rate of recurrent hiatal hernia (55%). A previous multicenter study reported that the risk factors of recurrence were younger age, postoperative retching, and extensive dissection of the esophageal hiatus [30]. In our study, younger age and lower body weight were also more significant in patients with recurrence. However, GER can lead to serious GERD-related complications in patients with EA. Patients in whom the procedure is unavoidable require anti-reflux surgery despite their young age and lower body weight. A previous study recommended active treatment of GERD in patients with EA [8]. According to our study results, although anti-reflux surgery performed at a young age and low body weight are risk factors for recurrence, Nissen fundoplication was relatively effective in controlling EA-associated GERD, thus consenting to aggressive GERD treatment in patients with EA.
Re-operation was not performed in all patients with recurrence but was performed in those with severe or progressive reflux symptoms. Patients with mild symptoms received conservative care, including medical treatment, during follow-up. We believe that the effect of fundoplication is often temporary because of the anatomical characteristics of EA, and a high re-operation rate might be observed during the long-term follow-up.
This study is inherently limited by its retrospective design. Hospitalization and treatment history in other hospitals may have been omitted, and a few data were difficult to obtain. A multicenter study with a long-term follow-up of GERD treatment might be required in the future in patients with EA.
In summary, the Nissen fundoplication was required more often for patients with complicated EA and was performed at a young age. Nissen fundoplication was relatively effective in controlling EA-associated GERD. However, fundoplication performed in patients with EA was associated with a high rate of recurrent hiatal hernia. A careful follow-up study is necessary because poor long-term outcomes are frequently observed.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Previous Presentation:Presented at the 37th Annual Meeting of the Korean Association of Pediatric Surgery.
Author Contributions:
Conceptualization: H.S.J.
Data curation: I.K., J.H.J., L.D.
Formal analysis: H.I.G. Funding acquisition.
Investigation: H.I.G.
Methodology: H.I.G.
Project administration: O.J.T., H.S.J.
Resources: I.K.
Software: I.K.
Supervision: H.S.J.
Validation: O.J.T.
Visualization: J.H.J.
Writing - original draft: H.I.G.
Writing - review & editing: H.S.J.
