

Purpose
Meckel's diverticulum (MD) is the most common congenital malformation of the gastrointestinal tract. The clinical presentation of MD is nonspecific and various, which can make diagnosis difficult. The aim of this study was to analyze the clinicopathologic characteristics and treatment outcomes of symptomatic MD in children.
Methods
We retrospectively reviewed the medical records of 38 pediatric patients diagnosed with MD who underwent surgery from April 1999 to September 2017. Five MD cases which were found incidentally during another surgery were excluded from this study. Sex, age, clinical presentation, diagnostic method, surgical treatment, histopathological findings were analyzed.
Results
Twenty-five cases occurred in boys and 8 cases occurred in girls. At the time of diagnosis, the age ranged from 6 months to 17 years, with an average of 92.4 months.
Thirteen patients (39.4%) were presented with melena, 7 patients (21.2%) with intestinal obstruction, 5 patients (15.2%) with intussusception, 5 patients (15.2%) with perforation, and 3 patients (9%) with diverticulitis. Meckel's scan was performed in 12 out of 13 patients with lower gastrointestinal bleeding, and all 12 (100%) showed a positive tracer. Out of total 33 patients, 12 underwent laparoscopic assisted bowel resection, 7 underwent laparoscopic assisted diverticulectomy, 5 underwent laparoscopic diverticulectomy, 7 underwent open bowel resection, and 2 underwent open diverticulectomy. There was only 1 postoperative wound infection in all 33 cases. There were 21 (63.6%) ectopic tissues in 33 symptomatic MD patients. Gastric mucosa was observed in 19 patients (57.6%), pancreatic tissue was found in 1 patient (3%), and both gastric mucosa and pancreatic tissue was present in 1 patient (3%).
Conclusion
Surgical resection of MD is safe and effective in symptomatic MD. Laparoscopic or laparoscopic assisted diverticulectomy or bowel resection is the treatment option for symptomatic MD.
Meckel's diverticulum (MD) is the most common congenital malformation of the gastrointestinal tract. The clinical presentation of MD is nonspecific and various, which can make diagnosis difficult. The aim of this study was to analyze the clinicopathologic characteristics and treatment outcomes of symptomatic MD in children.
We retrospectively reviewed the medical records of 38 pediatric patients diagnosed with MD who underwent surgery from April 1999 to September 2017. Five MD cases which were found incidentally during another surgery were excluded from this study. Sex, age, clinical presentation, diagnostic method, surgical treatment, histopathological findings were analyzed.
Twenty-five cases occurred in boys and 8 cases occurred in girls. At the time of diagnosis, the age ranged from 6 months to 17 years, with an average of 92.4 months. Thirteen patients (39.4%) were presented with melena, 7 patients (21.2%) with intestinal obstruction, 5 patients (15.2%) with intussusception, 5 patients (15.2%) with perforation, and 3 patients (9%) with diverticulitis. Meckel's scan was performed in 12 out of 13 patients with lower gastrointestinal bleeding, and all 12 (100%) showed a positive tracer. Out of total 33 patients, 12 underwent laparoscopic assisted bowel resection, 7 underwent laparoscopic assisted diverticulectomy, 5 underwent laparoscopic diverticulectomy, 7 underwent open bowel resection, and 2 underwent open diverticulectomy. There was only 1 postoperative wound infection in all 33 cases. There were 21 (63.6%) ectopic tissues in 33 symptomatic MD patients. Gastric mucosa was observed in 19 patients (57.6%), pancreatic tissue was found in 1 patient (3%), and both gastric mucosa and pancreatic tissue was present in 1 patient (3%).
Surgical resection of MD is safe and effective in symptomatic MD. Laparoscopic or laparoscopic assisted diverticulectomy or bowel resection is the treatment option for symptomatic MD.
Meckel's diverticulum (MD) is the most common congenital malformation of the gastrointestinal tract with a 2% prevalence rate in the general population [1, 2, 3, 4, 5]. It is located at the antimesenteric border of the ileum and arises from persistence of the congenital vitello-intestinal duct at the fifth week of gestation [6, 7, 8]. Most children with a symptomatic MD are present with gastrointestinal bleeding, intestinal obstruction by band or intussusception, perforation, or diverticulitis [9, 10, 11]. Traditional treatment of symptomatic MD has been excision with laparotomy, by wedge resection or segmental bowel resection. With the advancement of minimally-invasive surgery, laparoscopic or laparoscopic-assisted excision became possible. Laparoscopic stapling devices enable totally laparoscopic diverticulectomy. However, there is an issue of having a remnant ectopic tissue after diverticulectomy, exposing the patient to the risk of symptoms recurring. To better recognize the clinicopathologic characteristics and treatment of symptomatic MD, we reviewed the clinicopathologic features, diagnosis, and treatment outcome of pediatric patients with symptomatic MD.
We retrospectively reviewed the medical records of 38 pediatric patients under 17 years old diagnosed with MD who underwent surgery from April 1999 to September 2017 at Kyungpook National University Hospital. Out of 38 MD cases, 5 cases were found incidentally during another surgery. Data for sex, age at presentation, clinical presentation, diagnostic method, surgical treatment outcomes, and histopathological findings were collected from the patient database of 33 MD patients, excluding incidentally found 5 cases. The study protocol was approved by the Institutional Review Board (IRB) of Kyungpook National University Hospital (IRB No. 2021-03-039).
Twenty-five cases occurred in boys and 8 cases occurred in girls, with a male to female ratio of 3.1:1. The sex distribution according to the presentations was prevalent in men in the case of melena, intestinal obstruction, and diverticulitis, but there was no difference between men and women in the case of intussusception and perforation. At the time of diagnosis, the age ranged from 6 months to 17 years, with an average of 92.4 months. In the age distribution, 6 patients (18.2%) were under 1 year of age, 6 patients (18.2%) were 1 to 5 years of age, and 21 patients (63.6%) were older than 5 years old. The mean age according to the presentations was 7.2 years, 9.2 years, 6.8 years, 8.4 years, and 6.8 years in melena, intestinal obstruction, intussusception, perforation and diverticulitis, respectively. Tables 1 and 2 summarized the sex and age distribution according to the clinical presentation.

Table 1
Sex distribution according to the clinical presentation

Table 2
Age distribution according to the clinical presentation
Out of total 38 MD cases, 5 were found incidentally during another surgery. Three patients were discovered during surgery for acute appendicitis, one was found during surgery for right ovarian mature teratoma, and the other was discovered while performing exploratory laparotomy for congenital megacolon. The remaining 33 MD cases were symptomatic and presented with varying clinical presentations. Thirteen patients (39.4%) were presented with melena, 7 patients (21.2%) with intestinal obstruction, 5 patients (15.2%) with intussusception, 5 patients (15.2%) with perforation, and 3 patients (9%) with diverticulitis (Table 3).
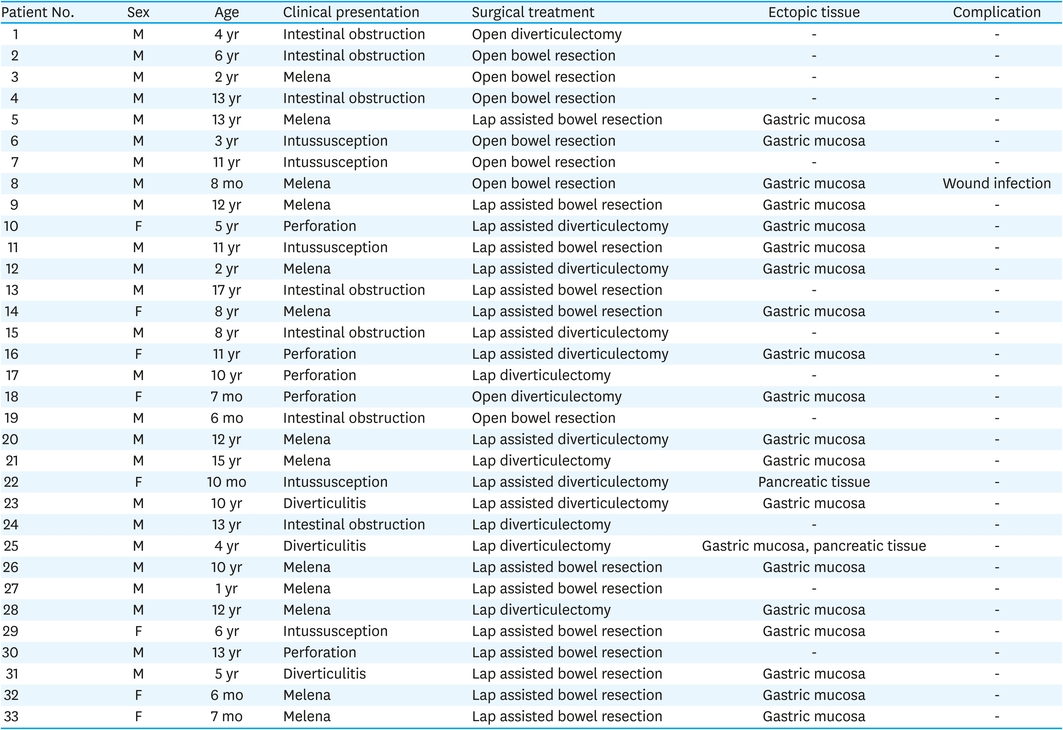
Table 3
Clinicopathologic characteristics and treatment outcome in the 33 symptomatic Meckel's diverticulum patients
Abdominal ultrasonography and computed tomography (CT) scan were performed in 13 cases and 28 cases respectively. Meckel's scan was performed in 12 out of 13 patients with lower gastrointestinal bleeding, and all 12 (100%) showed a positive tracer.
MD were located 20 cm to 130 cm proximal to the ileocecal valve on the antimesenteric margin of the ileum, with mean of 57.9 cm from ileocecal valve. The size of MD ranged from 1.5 cm to 12 cm (mean 4.0 cm), with a diameter of 0.5 to 3 cm (mean 1.7 cm).
When the base of MD was clean, diverticulectomy was performed, and when MD was accompanied by inflammation or ischemic change, bowel resection was performed. In addition, even if diverticulectomy was first considered at the time of surgery, if the possibility of remnant ectopic tissue or bowel stenosis was high, bowel resection was performed. Out of total 33 patients, 12 underwent laparoscopic assisted bowel resection, 7 underwent laparoscopic assisted diverticulectomy, 5 underwent laparoscopic diverticulectomy, 7 underwent open bowel resection, and 2 underwent open diverticulectomy. There was only 1 postoperative wound infection in all 33 cases.
One pathologist reviewed 33 tissue slides to determine the presence or absence of ectopic tissue. There were 21 (63.6%) ectopic tissues in 33 symptomatic MD patients. Gastric mucosa was observed in 19 patients (57.6%), pancreatic tissue was present in 1 patient (3%), and both gastric mucosa and pancreatic tissue was observed in 1 patient (3%). According to presentation, ectopic tissue was observed in 11 (84.6%) out of 13 patients with melena, 4 (80%) out of 5 patients with intussusception, 3 (60%) out of 5 patients with perforation. All 3 (100%) patients with inflammation were accompanied by ectopic tissue. However, there was no case of ectopic tissue in the 7 patients who presented with intestinal obstruction.
MD is the most common congenital malformation of the gastrointestinal tract. Yolk sac which is attached to the primitive gut by the omphalomesenteric duct is typically obliterated during fifth to ninth week of gestation. When omphalomesenteric duct is not obliterated during gestation, MD occurs [4]. Rule of 2 is commonly used to describe the characteristics of the MD, and refers to its male-to-female ratio of 2:1, prevalence rate of 2% in the general population, incidence rate of 2% of having a symptom due to MD, diverticular length of 2 inch, the occurrence of symptoms before 2 years of age, location of diverticulum 2 feet from the ileocecal valve, and 2 common types of ectopic tissues [11].
The reported male to female ratio ranges from 2:1 to 4:1 [4], which is similar to our study with male to female ratio of 3.1:1.
The clinical presentation of MD is nonspecific and various, which can make diagnosis difficult. However, children with complicated MD can present as surgical emergency such as diverticulitis, intestinal obstruction, intussusception, and gastrointestinal bleeding. Bleeding is the most common symptom of MD in children below the age of 10 [4]. In our series, gastrointestinal bleeding such as melena was also the most common presentation of symptomatic MD (39.4%).
Ectopic tissue in MD is present in 4.6% to 71.0% of symptomatic MD [3], with gastric tissue being most common, followed by pancreatic tissue. In our series, 63.6% of symptomatic MD had ectopic tissue such as gastric mucosa and pancreatic tissue, which was in accordance with other reports [3]. The existence of ectopic tissue is related to MD being symptomatic, especially with gastrointestinal bleeding. Burjonrappa and Khaing [12] reported that in patients with MD, the existence of ectopic tissue is the most important factor in establishing the necessity of a surgical intervention.
The accurate preoperative clinical diagnosis of MD may be difficult despite the availability of the modern imaging modalities. CT and Technetium-99m pertechnetate radionuclide scan are widely utilized in the diagnosis of MD [13, 14, 15, 16]. Technetium-99m pertechnetate scan has been the standard tool for the diagnosis of MD with ectopic gastric mucosa (EGM) in children. Sensitivity and specificity of the Meckel's scan is reported to vary from 60% to 90% and 90% to 98% [13, 14]. Sinha et al. [16] also reported the sensitivity of Meckel's scan to be 94% and its specificity to be 97%. In our series, Meckel's scan of 12 patients with melena showed positive in all 12 patients. Pharmacological administration of histamine type-2 receptor antagonists has been known to enhance the sensitivity of Meckel's scan after failure of the conventional test [13]. However, it is often during laparotomy or laparoscopy when MD can be correctly diagnosed.
Meckel's diverticulectomy can be done laparoscopically either by intracorporeal or extracorporeal method [17, 18, 19, 20, 21, 22, 23]. Intracorporeal diverticulectomy is possible totally laparoscopically with the use of endoscopic staplers, without the need to extend a trocar site. Laparoscopically stapled diverticulectomy can be done either transversely or obliquely to avoid narrowing of the adjacent bowel lumen. However, the concern of totally laparoscopic intracorporeal diverticulectomy is the risk of having remnant EGM. Determining the clearance of entire EGM within the diverticulum is a little problematic. EGM is difficult to detect through external inspection or by palpation of mucosal thickening. For long and narrow diverticula, EGM is likely to be confined near the tip of the diverticulum, and in short and broad-based diverticula, ectopic tissue is often located at the base, and sometimes extends to the adjacent bowel. Varcoe et al. [17] reported that all 5 cases of long MD with a height:diameter ratio (HDR) ≥ 2 had EGM in the tip and the body of the diverticulum. On the other hand, out of 20 short MD with HDR < 2, 12 cases had EGM involving the whole diverticulum including the base and only 8 had EGM confined to the tip and the body [17]. Mukai et al. [24] suggested simple resection for long diverticula. However, intraoperative frozen biopsy is necessary to ensure that the resection margin of the diverticulum is free of EGM [24]. Varcoe et al. [17] advised segmental resection of ileum if the height-to-diameter ratio of the MD is less than 2, due to the increased risk of having the ectopic mucosa in the adjacent ileum. A systemic review by Redman et al. [8] confirmed that if the risk of leaving remnant ectopic mucosa is low, laparoscopic diverticulectomy is a suitable technique in removal of MD in children. However, in cases such as 1) short and wide MD with an HDR of < 2; 2) ischemic change or thickening at the base of diverticula; 3) presence of small bowel obstruction or volvulus; and 4) when there is a suspicion that residual ectopic mucosa may be present while inspecting the resected specimen, laparoscopic-assisted extracorporeal segmental excision may be a safer option [8].
There is a controversy regarding prophylactic resection of silent MD when discovered incidentally during another surgery. Some authors recommend against resection of asymptomatic MD, due to high morbidity compared to its benefit. A systematic review by Zani et al. [25] reported the risk of complication after prophylactic resection to be 5.3% and the risk of MD left in situ developing symptoms to be 1.3%. After reviewing papers which reported follow up on patients with asymptomatic MD in situ, they concluded that there were no long-term complications due to leaving MD in situ. Also, they deduced that over 750 asymptomatic MD should be resected in order to avoid one case of mortality due to MD. Soltero and Bill [26] also advised against prophylactic resection. They calculated that roughly 800 asymptomatic MD must be removed to prevent one mortality due to complications of MD, and prophylactic surgery is likely to incur postoperative morbidity such as postoperative intestinal obstruction and infection [26].
On the contrary, Cullen et al. [27] suggested that the risk of asymptomatic MD becoming symptomatic did not decrease with age and recommended prophylactic resection, unless there are contraindications, such as generalized peritonitis or other conditions that can increase the risk of the operation. Others also advise prophylactic resection if certain criteria for asymptomatic MD becoming symptomatic are met. Park et al. [28] identified 4 such criteria to be presence of ectopic tissue, diverticular length greater than 2 cm, patient younger than 50 years, and male sex, from a retrospective study of patients from 2000 to 2017. When 1 of 4 criteria were met 17% of Meckel's diverticula were symptomatic. When 2, 3, or all 4 criteria were met chances of Meckel's diverticula being symptomatic were 25%, 42%, and 70% respectively. In our series, all 5 MD cases found incidentally during another surgery underwent resection of MD without complications.
In summary, Meckel's scan was very confirmative in diagnosing MD, especially in patients with melena. The authors performed diverticulectomy or segmental resection of bowel as a treatment for MD according to the status of MD at the time of surgery. However, this study has limitation in comparing the results of the 2 surgical methods due to its retrospective nature. We believed that prospective studies related to the results of these 2 surgical methods would be needed in the future.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: P.J.
Data curation: S.H.W., P.J, K.Y.N.
Formal analysis: S.H.W., P.J.
Investigation: S.H.W., P.J., K.Y.N.
Methodology: S.H.W., P.J.
Project administration: P.J.
Resources: P.J.
Supervision: K.Y.N., P.J.
Validation: P.J.
Visualization: P.J.
Writing - original draft: S.H.W., P.J.
Writing - review & editing: S.H.W., P.J.
