

Purpose
Pyloric muscle thickness (PMT) equal to or greater than 4 mm and canal length equal to or greater than 15 mm are used to be widely accepted for diagnosis of idiopathic hypertrophic pyloric stenosis (IHPS). However, up to 25% of IHPS patients show ultrasonic parameters discordant to current diagnostic criteria. The authors tried to look if previously suggested criteria could be applied to the IHPS patients of a single center and find new concepts by analyzing the ultrasonic parameters and patient characteristics.
Method
Medical records and ultrasonography (US) of 131 IHPS patients who received pyloromyotomy from 1994 to 2016 were reviewed. All presented with characteristic clinical symptoms. The patients were divided into 2 groups according to their eligibility for current criteria used in the authors' institution, as discordance group (n=32) and concordance group (n=99). Baseline characteristics were reviewed, and ultrasonic parameters were measured, and then the volume of pylorus was estimated by calculation using the measured parameters.
Results
The proportion of neonates was greater and the mean postconceptional age was younger in Discordance group than that of Concordance group at the time of US examination. Average weight at the time of US were lighter in discordance group than those of concordance group, as well. Also, mean pyloric volume (PV) and proportion of PMT/pyloric diameter were lesser in discordance group (1.72±0.49 mL vs. 2.98±0.87 mL and 31.87%±3.24% vs. 35.06%±3.61%, p<0.001), while mean luminal volume was similar in both groups. Postconceptional age and being neonate were significant variables for PV after multivariate linear regression (R 2 =0.390).
Conclusion
The calculated PV of IHPS patients was strongly related to their postconceptional age, and it suggested that the diagnostic criteria may differ according to the patients' sizes and the time of their diagnoses. Future diagnostic criteria for IHPS should be applicable even with the dynamic nature of the patients.
Pyloric muscle thickness (PMT) equal to or greater than 4 mm and canal length equal to or greater than 15 mm are used to be widely accepted for diagnosis of idiopathic hypertrophic pyloric stenosis (IHPS). However, up to 25% of IHPS patients show ultrasonic parameters discordant to current diagnostic criteria. The authors tried to look if previously suggested criteria could be applied to the IHPS patients of a single center and find new concepts by analyzing the ultrasonic parameters and patient characteristics.
Medical records and ultrasonography (US) of 131 IHPS patients who received pyloromyotomy from 1994 to 2016 were reviewed. All presented with characteristic clinical symptoms. The patients were divided into 2 groups according to their eligibility for current criteria used in the authors' institution, as discordance group (n=32) and concordance group (n=99). Baseline characteristics were reviewed, and ultrasonic parameters were measured, and then the volume of pylorus was estimated by calculation using the measured parameters.
The proportion of neonates was greater and the mean postconceptional age was younger in Discordance group than that of Concordance group at the time of US examination. Average weight at the time of US were lighter in discordance group than those of concordance group, as well. Also, mean pyloric volume (PV) and proportion of PMT/pyloric diameter were lesser in discordance group (1.72±0.49 mL vs. 2.98±0.87 mL and 31.87%±3.24% vs. 35.06%±3.61%, p<0.001), while mean luminal volume was similar in both groups. Postconceptional age and being neonate were significant variables for PV after multivariate linear regression (R2=0.390).
The calculated PV of IHPS patients was strongly related to their postconceptional age, and it suggested that the diagnostic criteria may differ according to the patients' sizes and the time of their diagnoses. Future diagnostic criteria for IHPS should be applicable even with the dynamic nature of the patients.
Idiopathic hypertrophic pyloric stenosis (IHPS) is one of the most common causes of abdominal surgery in neonates and infants. Incidences reported are 2 to 5 in 1,000 live births and as high as 8.2 to 12.3 cases per 1,000 live births in the United States [1, 2, 3]. It is an idiopathic cause of gastric outlet obstruction, which typically occurs during the 2nd to 12th week of life and is more common in boys than girls [4, 5]. Premature infants tend to present at a later chronological age than term infants [6, 7]. Clinical diagnosis is easily made with characteristic symptoms such as nonbilious vomiting and hypochloremic hypokalemic metabolic alkalosis. Treatment is either open or laparoscopic pyloromyotomy, while some report natural course without surgery [8].
Although thorough examination is sufficient to establish the diagnosis without the need for any imaging modality [9], upper gastrointestinal (GI) study with contrast was once considered as the test of choice. These days, ultrasonography (US) has become a critical adjunct in confirming the diagnosis of IHPS by measuring pyloric muscle thickness (PMT) and pyloric canal length (PCL).
However, there is some discrepancy in the literature concerning the diagnostic criteria which should be used to interpret an US study result as abnormal. Also, clinical diagnosis of IHPS is inconclusive in 15%–25% of the cases [10]. In the Republic of Korea, as suggested by Stunden et al. [11], diagnostic criteria of PMT equal to or greater than 4mm and PCL equal to or greater than 15 mm are widely accepted in consensus of pediatric surgeons [12]. Diagnostic criteria of US may differ in other countries, as PMT equal to or greater than 3 to 4 mm and PCL equal to or greater than 15 to 18 mm have been reported in many previous studies [3, 4, 5, 13].
In several studies, pyloric volume (PV) was calculated with ultrasonic measurements to suggest new diagnostic criteria for IHPS because of discordance between clinical symptoms and measured parameters. Westra et al. [14] suggested the PV of 1.4 mL or more as the volumetric criteria. Rohrschneider et al. [9] showed in their study with 85 IHPS patients that they had a mean PV of 2.7±1.1 mL while normal group had a mean PV of 0.6±0.3 mL. In Korea, Lee et al. [15] showed a result with an average PV of 3.26±1.38 mL.
In this study, the authors first analyzed ultrasonic parameters of pylorus retrospectively in IHPS patients, and next, they compared to see any discordance with commonly used two-dimensional diagnostic criteria and relatively novel volumetric criteria. Then, they analyzed if the parameters were proportional to specific patient factors such as age at presentation, duration of symptoms, body measurements, and other gestational factors. Finally, the authors searched for any common characteristics between those who met the diagnostic criteria and those who did not. This is the first series of Korean IHPS patients, which compared the characteristics of the patients who fulfill the criteria and those who do not.
We reviewed the medical records of 322 pediatric patients who underwent Fredet-Ramstedt pyloromyotomy after diagnosis of IHPS from May 1994 to December 2016. All were confirmed with pyloric muscle hypertrophy in the operational field according to their operational record. Among them, electronically accessible ultrasonic records were available for 131 patients. As a result, 131 patients were selected for the final analysis (Fig. 1). The patients were divided into two groups according to the current IHPS criteria used in Korea. Thirty-two patients with PMT thinner than 4 mm or canal length shorter than 16 mm were grouped as discordance group and 99 patients who fulfilled the criteria for both dimensions were called concordance group.
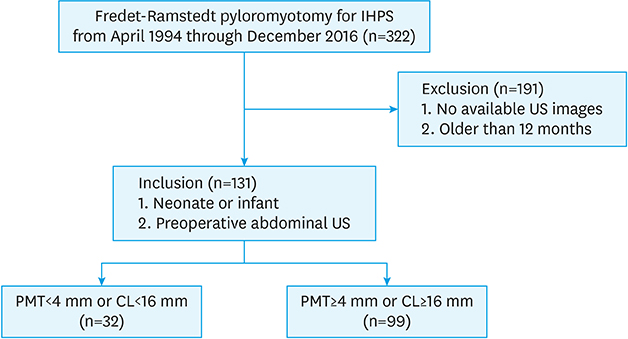
Fig. 1
Study population.
IHPS, idiopathic hypertrophic pyloric stenosis; US, ultrasonography; PMT, pyloric muscle thickness; CL, canal length.
Baseline characteristics of each patient were collected from the electronic medical records (Table 1). Pyloric parameters of the patients did not remain in the electronic medical record archives, so they were measured on the saved images of the preoperative US using picture archiving and communication system. The muscle thickness was measured for the muscularis propria only, excluding other layers such as mucosa, submucosa, and serosa on the cross-sectional image of pylorus. The diameter was measured for the longest line across the middle portion of the cross-sectional pylorus. The canal length was re-measured as well, for the longest length of the canal shown among the captured images.
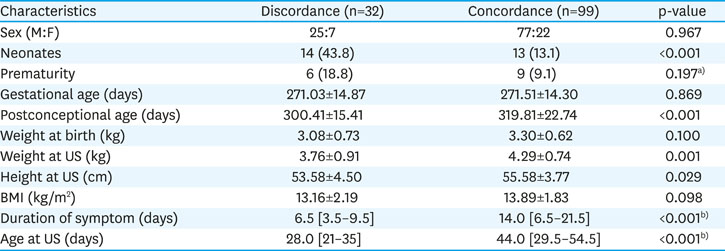
Table 1
Baseline characteristics
For volumetric analysis of pylorus, PV was calculated to visualize the amount of hypertrophy. The volume of the pylorus was estimated by calculation of the volume of a pipe (Fig. 2). The volume of the lumen was estimated by calculation of the inner cylinder of the pylorus model.
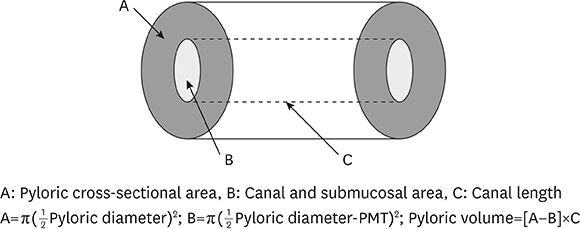
Fig. 2
Calculation of the volume of pylorus with the pipe model.
The study was approved by the Institutional Review Board of Ajou University Hospital (AJIRB-MED-MDB-19-240), and informed consents were waived due to its retrospective study design.
Student's t-test and Mann-Whitney U test were used to compare the continuous variables between the two groups, which were expressed as mean standard deviation or median (interquartile range [IQR]). The categorical variables were presented as frequency (%) and statistically compared using the χ2 or Fisher's exact test when appropriate. Related factors of the patients and pyloric muscle volume were evaluated by Pearson correlation and partial correlation. Multiple linear regression analysis was performed for variables that showed statistical significance in correlations. Statistical analysis was performed using SPSS® Statistics 25.0 (IBM Corp., Armonk, NY, USA).
A total of 32 patients were classified as discordance group and 99 patients were classified as concordance group (Table 1). The discordance group, whose initial diagnosis was inconclusive because of the discordance to known criteria, made up to 24.4% of the total population. They underwent upper GI series with contrast to support the diagnosis. In both groups, male to female ratio was about 3.5:1.
The proportions of neonates were 43.8% in discordance group and 13.1% in concordance group, which had a statistical significance (p<0.001). Although the proportion of premature patients with gestational age <37 weeks were 18.8% and 9.1% in discordance group and concordance group respectively, they did not have a statistical significance. In both groups, mean gestational age was 271 days, which could be converted to 38 weeks and 5 days. However, postconceptional age showed a difference between the 2 groups. Concordance group showed a mean of 19.4 days of older postconceptional age in days at the time of US examination, and it also had a statistical significance (p<0.001).
Body weight at the time of birth did not show statistically significant difference but the body weight and height at the time of US examination showed a statistical significance. Concordance group was 4.29±0.74 kg in weight and 53.58±4.50 cm in height while discordance group was 3.76±0.91 kg and 55.58±3.77 cm, respectively. However, body mass index (BMI) did not show a significant difference. The median duration of symptom was shorter in discordance group (6.5 [3.5–9.5] days) than in concordance group (14.0 [6.5–21.5] days), which had a statistical significance (p<0.001). Also, the median chronological age at the time of US was 28.0 [21–35] days in discordance and 44.0 [29.5–54.5] days in concordance groups (p<0.001).
Values of PMT were significantly lesser in discordance group than concordance group (3.74±0.35 mm vs. 4.86±0.59 mm, p<0.001). Values of PCL, pyloric diameter (PD), and PV were also greater in concordance group (Table 2). Mean pyloric muscular volume was 1.72±0.49 mL in discordance group while that of concordance group was 2.98±0.87 mL. However, the values of the luminal volume were not statistically different in both groups (0.29±0.18 mL vs. 0.33±0.21 mL, p=0.423). Thus, the proportion of lumen volume to PV was significantly higher in discordance group. In discordance group, proportion of PMT in PD was 31.87%±3.24%, while it was 35.06%±3.61% in concordance group.
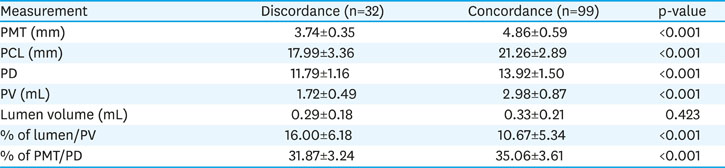
Table 2
Ultrasonic measurements of pylorus
PV was positively related to postconceptional age (Fig. 3), with R2=0.338. It was seemed to be related to body weight at US with R2=0.190 (Fig. 4). Multivariate linear regression analysis was performed with significant variables found by Pearson and partial correlation and a dummy variable. If the patient was a neonate under chronological age of 28 days, it was scored as 1, while infants were scored as 0. Postconceptional age and being neonate remained as significant variables (R2=0.390) (Table 3).
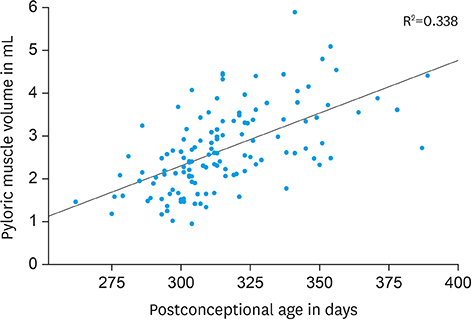
Fig. 3
Pyloric muscle volume in mL according to postconceptional age in days.
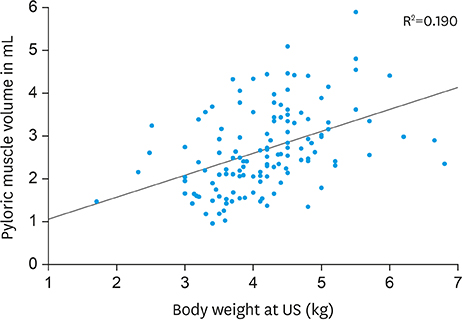
Fig. 4
Pyloric muscle volume in mL according to body weight in kg at the time of US examination.
US, ultrasonography.

Table 3
Multivariate linear regression analysis (stepwise forward)
Clinical diagnosis of IHPS can still be made with characteristic symptoms, yet diagnostic imaging modality of IHPS has been evolving. Upper GI study with contrast was once considered the test of choice but advances in real-time US has become a critical adjunct in confirming the diagnosis of IHPS by measuring PMT and PCL. Furthermore, evaluation of peristaltic movement and gastric emptying by US can be considered as an aid to the morphologic diagnostic criteria. However, evaluation of functional aspects of pylorus would be vague and subjective to radiologists.
Up to 25% of IHPS patients are initially inconclusive in diagnosis because even though their symptoms are present, ultrasonic measurements do not fulfill the criteria. In this cohort, IHPS patients discordant to diagnostic criteria were 24.4%, and this was similar to the previous report [10]. The characteristics of these patients tend to be “smaller” in size and “younger” in age, in terms of body weight, height, and chronological age and postconceptional age at presentation. Iqbal et al. also suggested in their series of 318 ultrasounds, that the measurements of the pylorus had correlations with age and weight [3].
The authors chose the postconceptional age as a variable because the number of premature infants were too small to undergo statistical analysis. Also, the duration of vomiting symptom tends to be shorter in discordance group but this variable did not show any correlation to PV after adjustment by chronological age. Although Hsu et al. [16] suggested that the size of pylorus did not matter in diagnosis of IHPS, our result showed that smaller pylorus can be a hypertrophic pylorus in smaller infants.
PV was suggested as a possible diagnostic criteria decades ago while it was not popularized due to the complexness of its calculation and possible errors in measuring the dynamic shape of the pylorus. Mean PV of all patients in this cohort was 2.67±0.97 mL, which was similar to the study reported by Rohrschneider et al. [9], showing mean PV of 2.7±1.1 mL in patients and 0.6±0.3 mL in normal group. Simplifying the curved pipe to a straight pipe, Westra et al. [14] suggested a cutoff value of 1.4 mL to confirm the diagnosis of IHPS. According to our result, the least value of pyloric muscular volume was 0.95 mL, and while 94.7% of the patients met Westra's criteria, 5.3% of the patients still did not match, whose postconceptional age were under 310 days.
In the multivariate linear regression model in predicting PV, postconceptional age and being a neonate were the two factors that showed statistical significance. Although the equation may not be able to suggest a pathologic limit of PV in all patients, it could be interpreted that the pathologic PV could be a dynamic value according to patient factors, not a set number.
However, the volume of the lumen seemed to be relatively consistent in discordance and concordance groups in this study. If the luminal volume is a stable factor among the patients, and the pyloric size varies with body weight and chronological age, the authors wondered if there could be a breaking point in terms of muscle proportion where the hypertrophy progresses and exceeds the “normal” value.
So, the authors looked into the proportion of PMT over PD. PD consists of thickness of two muscle layers and a lumen diameter. The proportion of single layer of PMT to the PD was 31.87%±3.24% in Discordance group while 35.06%±3.61% in Concordance group. Although this study was conducted without a control group, Rohrschneider et al. [9] reported that the PD and PMT of normal group were 8.4±1.7 mm and 1.8±0.5 mm, respectively. Calculating the proportion of mean PMT to mean PD according to their data, it would be 21.43% in the control group, and their IHPS group had PMT of 4.7±0.9 mm and PD of 14±2 mm, thus the proportion of mean PMT to mean PD would be 33.57%. The authors found that the mean PMT/PD in all patients of this study was 34.28%±3.78%, with the least value of 27% and the greatest value of 45%.
The limitation of this study is that this is a retrospective study conducted in a single center in Korea. Also, this study includes patients only. A larger cohort with a control group is needed to review if the proportion of PMT to PD could be used as a novel adjunctive diagnostic criteria for IHPS patients with inconclusive diagnosis.
In conclusion, while treatment for IHPS is relatively easy, diagnosis is still an enigma. Because up to 25% of IHPS patients show discordant ultrasonic parameters compared to current diagnostic criteria, other variables that could be used in adjunct is needed. Although upper GI test with contrast study could be useful, it is often difficult to conduct because of recurrent vomiting of the contrasts by the young patients.
This study shows that PV of IHPS patients was strongly related to the postconceptional age and suggests that the 2-dimensional diagnostic criteria may not be the best values, disregarding the chronological factor. Future diagnostic criteria for IHPS should reflect the dynamic nature of the patients. Further study should be conducted with control group to evaluate if there exist normal range and diagnostic value of the proportion of PMT to PD.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: S.J., H.J.
Data curation: S.J., H.J.
Formal analysis: S.J.
Investigation: S.J., H.J.
Writing - original draft: S.J.
Writing - review & editing: S.J., H.J.
We appreciate Yeon Hee Ahn and Hyun-A Jung for their unconditional help for patient care and data management for the Department of Pediatric Surgery.
