

Purpose
Late presenting congenital diaphragmatic hernia (CDH) in children has various clinical manifestations and serious pitfalls in diagnosis, which make differentiation very difficult. Thus, we intended to identify the clinical manifestations and to build the proper strategy of diagnostic imaging for late presenting CDH on the base of our institutional experience.
Methods
We performed a retrospective review of medical records for 6 patients who received the operation for late presenting CDH from December 2003 to March 2018 in our hospital.
Results
The range of age was 55 days to 13 years and the ratio of sex (male:female) was 2:1. The most common symptom was vomiting, followed by abdominal pain, chest discomfort, dyspnea, and cyanosis. As an initial diagnostic imaging study, chest X-ray was performed in all patients, of whom one patient checked it after the insertion of a gavage tube. As a secondary additional imaging study, chest computed tomography (CT) was performed in 4 patients, abdominal ultrasonography was performed in 2 patients, and chest magnetic resonance imaging, abdominopelvic CT, renal scan were each carried out for 1 patient.
Conclusion
If late presenting CDH is suspected in initial chest X-ray of patient who has gastrointestinal or respiratory symptoms, chest X-ray after insertion of a nasogastric tube or additional imaging study such as chest CT should be checked.
Late presenting congenital diaphragmatic hernia (CDH) in children has various clinical manifestations and serious pitfalls in diagnosis, which make differentiation very difficult. Thus, we intended to identify the clinical manifestations and to build the proper strategy of diagnostic imaging for late presenting CDH on the base of our institutional experience.
We performed a retrospective review of medical records for 6 patients who received the operation for late presenting CDH from December 2003 to March 2018 in our hospital.
The range of age was 55 days to 13 years and the ratio of sex (male:female) was 2:1. The most common symptom was vomiting, followed by abdominal pain, chest discomfort, dyspnea, and cyanosis. As an initial diagnostic imaging study, chest X-ray was performed in all patients, of whom one patient checked it after the insertion of a gavage tube. As a secondary additional imaging study, chest computed tomography (CT) was performed in 4 patients, abdominal ultrasonography was performed in 2 patients, and chest magnetic resonance imaging, abdominopelvic CT, renal scan were each carried out for 1 patient.
If late presenting CDH is suspected in initial chest X-ray of patient who has gastrointestinal or respiratory symptoms, chest X-ray after insertion of a nasogastric tube or additional imaging study such as chest CT should be checked.
Late presenting congenital diaphragmatic hernia (CDH) is defined as a nontraumatic diaphragmatic hernia which was diagnosed after infancy. Its rare incidence, variety of clinical manifestations, and pitfalls in initial chest X-ray make the differential diagnosis very difficult [1, 2, 3, 4]. In this study, we intended to identify the clinical manifestations and to build the proper strategy of diagnostic imaging for late presenting CDH on the base of our institutional experience.
From December 2003 to March 2018, six children received the operation for late presenting CDH in our hospital. We investigated the patients' clinical information relating to age at diagnosis, sex, chief complaint during the first visit, diagnostic imaging study, and operative findings through a retrospective review of medical records. Hiatal hernia was excluded. This study was approved and the requirement for informed consent from individual was waived by the Institutional Review Board of Jeonbuk National University Hospital (IRB No.: 2020-03-052).
As shown in Table 1, the range of patients’ age at diagnosis was scattered insignificantly from 55 days to 13 years. The ratio of sex (male:female) was 2:1. The clinical manifestations of the patients were not typical nor single but mixed or various. The most common symptom was vomiting, followed by abdominal pain, chest discomfort, dyspnea, and cyanosis. As an initial diagnostic imaging study, chest X-ray was performed routinely in all patients, of whom one patient checked it after the insertion of a gavage tube fortunately. As a secondary additional imaging study, chest computed tomography (CT) was performed in four patients, abdominal ultrasonography was performed in 2 patients, and chest magnetic resonance imaging (MRI), abdominopelvic CT, renal scan were each carried out for one patient. Fig. 1 shows initial chest X-ray and convincing secondary additional imaging studies for these patients. In operative findings, the location of the diaphragmatic defect was the left posterolateral side in 5 patients and the right posterior side in 1 patient. The small bowel and colon were herniated into the thoracic cavity through the diaphragmatic defect in all of the patients. Spleen herniation was identified in 3 patients. Stomach and kidney herniation were each identified in 2 patients. Malrotation of the cecum and Meckel's diverticulum were discovered incidentally during operation. Most of the operations were performed promptly after confirmation of diaphragmatic hernia; however, 1 patient with right posterior side CDH received preoperative care for acute bronchiolitis for 9 days. The postoperative outcomes were excellent without significant complications.
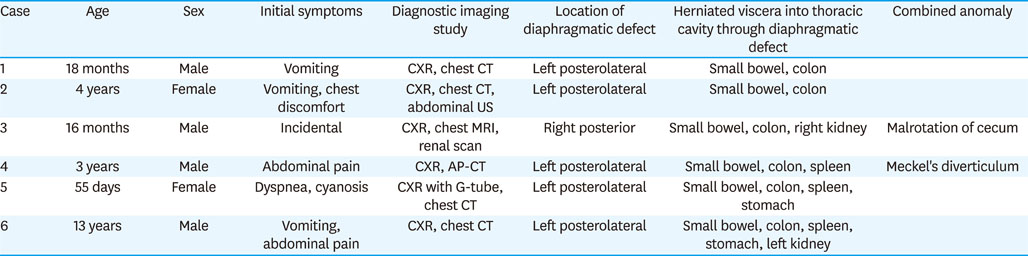
Table 1
Clinical manifestations, diagnostic tools, and operative findings of late presenting congenital diaphragmatic hernia in children (n=6)
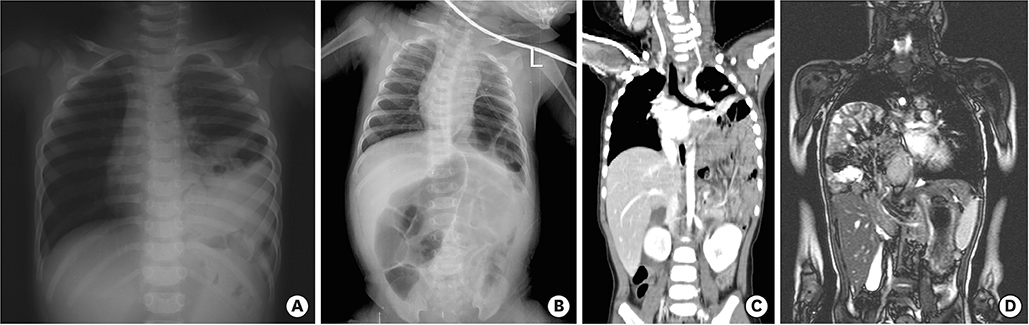
Fig. 1
Initial chest X-rays and convincing secondary additional imaging studies of late presenting CDH in children. (A) Initial chest X-ray of the left side CDH which was vague. (B) Chest X-ray after a gavage tube insertion in the left side CDH. (C) Chest CT showing the left side CDH. (D) Chest MRI showing the right side CDH.
CDH, congenital diaphragmatic hernia; CT, computed tomography; MRI, magnetic resonance imaging.
Late presenting CDH is difficult to differentiate with initial chest X-ray and misdiagnosis is not uncommon, which can result in various iatrogenic complications [1]. Also, delayed diagnosis can result in serious complications such as herniated bowel necrosis, peritonitis, respiratory arrest, and death [3, 5, 6]. Thus, early diagnosis and prompt surgical treatment is very important.
The clinical manifestations of patients were not typical but various. In other words, the initial symptoms of late presenting CDH could be respiratory or gastrointestinal or mixed, or patients could be asymptomatic [7]. This study reconfirmed this as shown in the results.
Rarely late presenting CDH can be combined with lung hypoplasia and malrotation, which may influence clinical manifestations and herniated viscera through diaphragmatic defect [8]. In this study, there was no lung hypoplasia nor typical malrotation in combined anomaly, so herniated viscera also contained the organs adjacent to hernial defect. Thus, we could not identify the correlation between clinical manifestations and combined anomaly.
There have been a few reports about the clinical manifestations in late presenting CDH noting that younger patients have more respiratory symptoms, and left side CDH patients have more gastrointestinal symptoms [7, 9]. Although the number of patients in this study was too small to obtain statistical significance, most of the left side cases (4 out of 5) presented gastrointestinal symptoms, and the youngest patient, who was 55 days old, showed respiratory symptoms only.
As a diagnostic imaging strategy in this study, initial chest X-ray and secondary additional imaging studies were performed for all of the patients. As a secondary additional imaging study, CT was performed in most of the patients (5 out of 6). Chest X-ray supplemented by cross-sectional imaging like chest CT can be very helpful in the differential diagnosis of intrathoracic lesions and provide better understanding of diaphragmatic pathology [10, 11]. The radiation hazard caused by diagnostic CT scans could be reasonably accepted as compared with the risk of serious complications of late presenting CDH [12].
The clinical manifestations of late presenting CDH have a wide spectrum, and were various and mixed between gastrointestinal symptoms and respiratory symptoms. The initial chest X-ray should be checked carefully, especially if a patient has the mixed symptoms. If necessary, the chest X-ray should be rechecked after a nasogastric tube insertion. Moreover, judging from the results of this study—that over half of the initial chest X-ray were vague, and secondary additional imaging studies like CT or MRI were performed to obtain conviction for CDH in all cases—if late presenting CDH is suspected at all, there should be no hesitation in ordering additional image studies like chest CT.
Funding:This paper was supported by Fund of Biomedical Research Institute, Jeonbuk National University Hospital.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: S.H.B, J.Y.J.
Data curation: S.H.B.
Funding acquisition: S.H.B., J.Y.J.
Supervision: J.Y.J.
Writing - original draft: S.H.B.
Writing - review & editing: J.Y.J.
