
 , Suhyeon Ha
, Hyunhee Kwon
, Jung-Man Namgoong
, Dae Yeon Kim
, Suhyeon Ha
, Hyunhee Kwon
, Jung-Man Namgoong
, Dae Yeon Kim

Since the first introduction of robotic surgery systems in Korea in 2005, there has been a gradual increase in the number of robotic surgeries performed. However, robotic liver resection is one of the most complex procedures, and its application, especially to children, is still limited. Therefore, in this study, we aim to present our experiences with 2 pediatric patients who underwent robotic liver resection in Asan Medical Center and discuss the safety and feasibility of robot-assisted hepatectomy in pediatrics.
Since the first introduction of robotic surgery systems in Korea in 2005, there has been a gradual increase in the number of robotic surgeries performed. However, robotic liver resection is one of the most complex procedures, and its application, especially to children, is still limited. Therefore, in this study, we aim to present our experiences with 2 pediatric patients who underwent robotic liver resection in Asan Medical Center and discuss the safety and feasibility of robot-assisted hepatectomy in pediatrics.
The majority of liver surgery worldwide continues to be performed open, as laparoscopic hepatectomy is technically challenging with a steep learning curve [1]. Likewise, liver resection with minimally-invasive techniques has been successfully used in pediatric hepatic lesions but still presents immense challenges due to its technical difficulties which only further exemplify the need of qualified pediatric surgeons and optimal selection of cases depending upon the resectability of the lesion [2]. Robotic technology overcomes many of the technical limitations of laparoscopy and improves the ability of hepatobiliary surgeons to safely perform minimally invasive hepatectomy [3].
The robotic surgery was first introduced in Korea in 2005 and the first robotic surgery was performed in the same year, which was cholecystectomy, and it has been gradually increasing in Korea [4]. Robotic liver resection is one of the complex procedures among robotic general surgery and its application is still limited in pediatric patients. In this article, we would like to present 2 robotic liver resection cases in pediatrics and technical method and outcome.
There were 2 patients underwent robotic partial hepatectomy with Da Vinci Xi Surgical System (Intuitive Surgical, Sunnyvale, CA, USA). They both are diagnosed with focal nodular hyperplasia(FNH) of liver from preoperative core-needle biopsy.
A 2-year-old female patient presented with abdominal distension and palpable mass. The abdominal ultrasound and computed tomography scan revealed a 6 cm sized hepatic mass with prominent central feeding artery in left lateral segment of liver and the tumor was diagnosed as an FNH from sonography guided core needle biopsy. Then she was followed up on outpatient setting every 6 months. The tumor had been stable in size for 5 years, but in 2022, when she got 8 years old, there was newly noted FNH lesion about 1.6 cm in liver segment VII. In 2022, she presented persistent mild abdominal pain and the surgeon decided to operate liver resection.
She was 8-year-old and 134 cm, 28.9 kg with body mass index (BMI) 16 kg/m2 when she got robotic liver resection. America Society of Anesthesiologists physical status classification score was 2 due to previous febrile seizure. She has got robot assisted partial hepatectomy for her liver mass located in segment II and III. Tumor size was 6.0 × 3.0 cm and operation time was 210 minutes. There was no complication including bleeding and she was discharged in postoperative day 6 (Fig. 1).
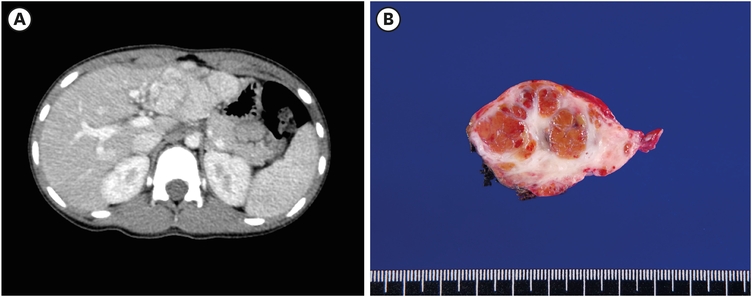
Fig. 1
Case 1. (A) preoperative abdominal pelvic CT scan; (B) resected specimen.
CT, computed tomography.
A five-year-old male patient complained abdominal pain and he went through sonographic work up and there was about 9 cm sized liver mass in left hemi-liver. The lesion was confirmed as a FNH by sonography guided needle biopsy. He was routinely followed up by 6 months with sonographic imaging and the mass had been growing gradually, so he went through robotic liver resection when he got eight years old.
When he got surgery, he was 140 cm and 30 kg with BMI 15.7 kg/m2. American Society of Anesthesiologists physical status classification score was one. He went through robotic assisted partial hepatectomy. Tumor was located in segment II, III, IV and size was 12.0×7.0 cm. Operation time was 193 minutes. There was no complication including bleeding and he was discharged in postoperative day 6, same as 1st case patient (Fig. 2).
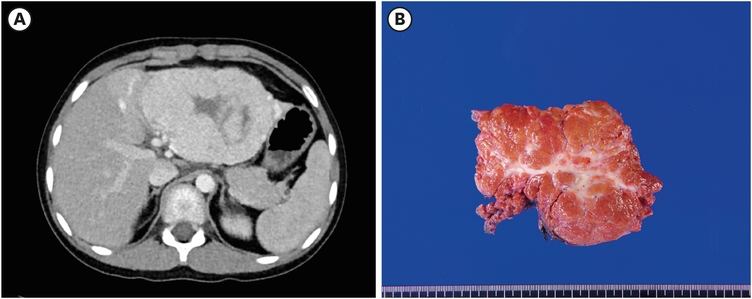
Fig. 2
Case 2. (A) preoperative abdominal pelvic CT scan; (B) resected specimen.
CT, computed tomography.
Patients were admitted the day before surgery and there was no other preoperative preparation for robotic approach.
In the supine position, umbilical single port, additional one 5 mm trocar and two 8 mm trocars were inserted (Fig. 3). Tumor was identified, and resection margin was confirmed. The liver was elevated by extracorporeal suture through the falciform ligament. Surgeon explored and identified calot’s triangle and measured distance from tumor resection margin and started liver resection with Maryland bipolar forcep and vessel sealer extend. Since both patients went through partial hepatectomy for tumor in left lobe, dissections of inferior vena cava and hilum of liver was not performed in order to obtain segmental vascular control. Also, cholecystectomy was not done in both patients. Liver resection was done by vessel sealer extend using sow fracture technique with assist of Maryland bipolar forcep and ProGrasp forceps (Figs. 4 and 5).
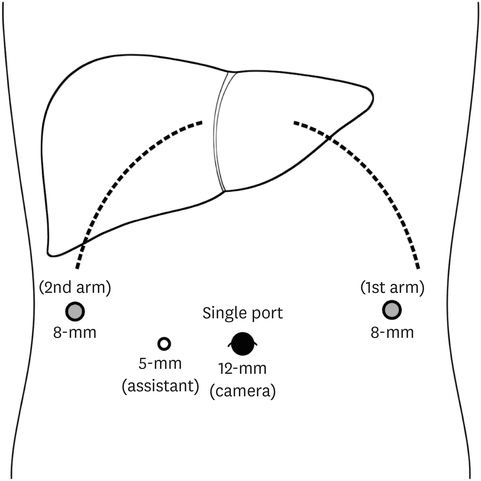
Fig. 3
An umbilical single port, two 8-mm robot trocars and one 5-mm assistant trocar were inserted for robotic hepatectomy. The exact trocar sites can vary depending on patient’s size and tumor location.
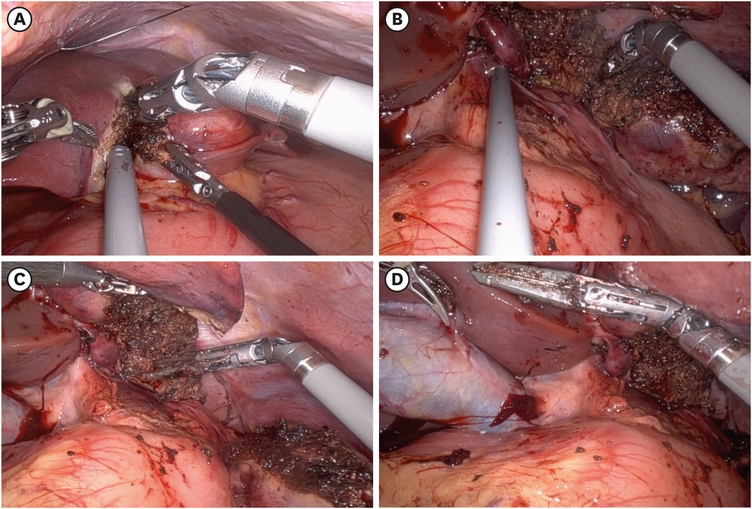
Fig. 4
Case 1. (A) Maryland forceps and assist grasp forceps are utilized to apply traction on the liver in opposite directions, while the vessel sealer is initiating liver resection. (B) Articular movement of vessel sealer. (C) Resection done. (D) After hepatectomy, hilum and gallbladder.
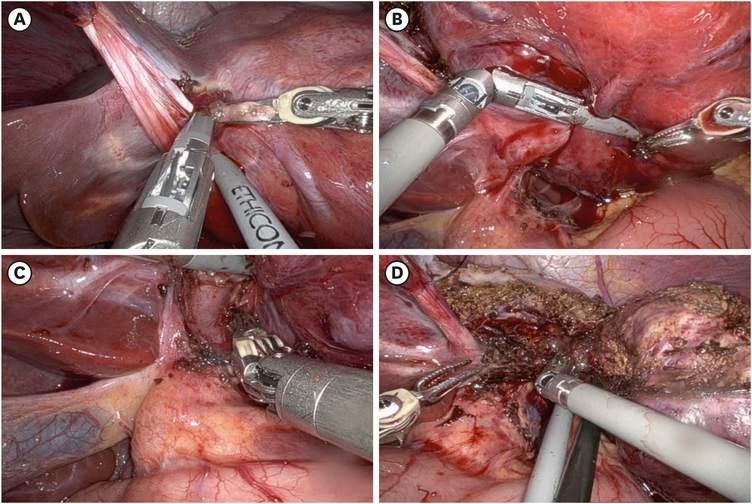
Fig. 5
Case 2. (A) Using the left Maryland forceps and right vessel sealer, proceed with bleeding control along the umbilical fissure and advance with the resection. (B) Right upper, left lateral portal vein was identified. (C) The process of left lateral portal vein coagulation through the using of a vessel sealer. (D) Articular movement of vessel sealer.
Umbilical wound was minimally elongated to pull out the resected specimen and both patients’ specimens were not ruptured. Both patients’ total estimated blood loss was “minimal,” less than 100 mL and both patients did not need transfusion during surgery. There was no intra-operative complication for both patients.
Both patients were admitted to pediatric intensive care unit postoperatively, on cefotaxime and pain killers. The next day they both transferred to general ward without any events. The drainage of the 2 patients was minimal after operation; no complication such as biliary leakage, postoperative bleeding, nor liver failure was observed. Both patients needed pro re nata pain killer injection until postoperative day 3. The Case 2 patient had to get foley reinserted due to voiding difficulty and he could self-void on postoperative day 5. Both patients started sips of water on postoperative day 3 and the next day they started oral feeding. Drain was removed on postoperative day 4 in Case 1 and postoperative day 5 in Case 2. The postoperative hospital stay was 6 days in both patients. Postoperative histologic examination of the specimen demonstrated focal nodular hyperplasia with clear resection margin.
With over a year of follow up (follow up period; 28 months for Case 1, 30 months for Case 2), none of the patients suffered complications. For the Case 1 patients, the hypoechoic lesion newly seen in segment VII was disappeared on post operation 4 months follow up sonography. Both patients and parents of them are satisfied with the wound.
Robot assisted liver resection is a great innovation in liver resection for hepatic tumors in pediatrics, featuring articular movement of robotic wrist with tremor filtration function and 3-dimensional HD magnification imaging system [5, 6, 7]. Hepatobiliary surgery stands as one of the most challenging parts in surgery requiring meticulous dissection, fine and stable hand movements, enhanced magnification with a wide field of vision, and expansive hand range movements within the confines of a restricted surgical field, particularly when dealing with small children. Robotic liver resection has emerged as feasible and safe approach for various anatomical liver resections, even in more complex surgery recently. Despite the existing limitations in the available instruments for robotic liver resection, continual advancements in technology and the ongoing evolution of robotic instruments signify promising developments [4].
Learning robotic liver resection is generally considered easier compared to standard laparoscopy, owing to the flexibility and stability of the instruments. Several studies have indicated that even novice surgeons can rapidly acquire robotic skills through a well-structured training curriculum [8]. However, it is advisable to commence the robotic procedure following through extensive simulation and wet lab training. The early learning curve is a great advantage for pediatric surgeons, given the rarity of pediatric cases. Magistri et al. [9] demonstrated that a minimum of 30 cases of robotic liver resection are required to achieve reductions in operative time, blood loss, and hospital stay. Similarly, using an analysis based on open conversion rates, Zhu et al. [10] reported a learning curve for robotic minor/major hepatectomy consisting of only 30 cases. Chen et al. [11] delineated a 3-phase learning curve, encompassing initial (phase 1, 15 patients), intermediate (phase 2, 25 patients) and mature (phase 3, 52 patients). The findings revealed improvements in operation time and hospital stay during initial phase, reduced blood loss during the intermediate phase, and enhancements in both operation time and blood loss during the mature phase.
While robot-assisted liver resection is not widespread in pediatric patients due to the lack of robotic liver resection device, need for multiple large caliber trocar incisions and the associated cost, there is a relatively higher incidence of robot-assisted choledochal cyst excision. Jin et al. [12], involving 133 patients with choledochal cyst, reported that robot-assisted resection of choledochal cyst is safe and feasible, and its postoperative recovery was shorter compared to traditional laparoscopy [12]. Another systemic review article by Zhang et al. [13] also reported shorter hospital stay of robot-assisted surgery than laparoscopic surgery through pooled analysis.
The primary constraint in robotic liver surgery lies in the absence of efficient robotic transection device. In open and laparoscopic hepatectomies, there are multiple effective energy devices including variety of harmonic scalpels, bipolar tissue sealing devices, radiofrequency and fluid-based devices such as the TissueLink and Aquamantys, and ultrasonic aspirators such as the cavitron ultrasonic surgical aspirator. However, robot-compatible instruments available for the parenchymal division are limited. Currently, these include the harmonic scalpel and bipolar tissue sealing devices (LigaSure™ Maryland Vessel Sealer; Medtronic, Minneapolis, MN, USA). Harmonic scalpel has the potential risk for partially injuring large vessels within the deep liver parenchyma and exhibits limited effect on controlling bleeding from the moderately sized portal pedicles and healing bile ducts. Also harmonic scalpel is difficult to track various parenchymal transection planes because it does not have EndoWrist function. Therefore, in these 2 cases, we used Maryland on left hand and vessel sealer on right hand of surgeon to resect liver.
Also, for pediatric patients, small abdominal cavity limit working space. Insufflation volumes and pressures are limited in small children in anesthesia aspect, which limits the working space too. Also unique port placement is required based on child’s size and there is a limitation for ability to use the fourth arm. The Da Vinci system was approved by the US Food and Drug Administration for intra-abdominal surgery for pediatrics but the only available instrument sizes on the Da Vinci system are 5 and 8 mm, thus limiting the ability of this system to be used in neonates and small children. More recently, the Senhance robotics system has developed 3 –mm instrument sizes, which is not approved for pediatric usage but could make robotic surgery more technically feasible for even the smallest pediatric patient [14]. And robotic endoscopes are currently only available as 12.0 and 8.5 mm, as a previously available 5-mm scope was discontinued owing to low use. And the manufacturer of the Da Vinci surgical platform recommends placement of ports 8 cm apart, which makes it difficult to achieve in small children or neonates where anatomic space is limited. However, Denning et al. [15] suggested that small size, less than 10 kg, is not necessarily a contraindication, depending on the specific patient and procedure. Meehan et al. [16] reported their experience of over 300 cases of patients ranging from 1 day old to 22 years old age and weights of 2.2 up to 120 kg.
The first pediatric robot surgery has been conducted in 2001, a case of Nissen fundoplication [17], and there have been numerous advancements that have allowed for successful robotic-assisted operations in multiple pediatric subspecialties. Single-site robotic surgery has been developed for use in pediatric patients [18]. And telerobotic surgery, or telesurgery, has been conducted and the first case was a robotic cholecystectomy, which performed in 2001 in New York for a patient located in Strasbourg, France [19]. These developments will allow for the expansion and widespread implementation of pediatric robotic surgery. Furthermore, instruments designed with pediatric patients in mind may also be developed and allow more safe and feasible pediatric robot surgery. More studies and larger case series are needed to compare the results with other modalities of surgery or other diagnosis to figure out the oncologic outcome of robot surgery in pediatrics.
In conclusion, based on our single center experience of two cases of robotic hepatectomy in pediatric patient, it is considered as safe and effective treatment. We cautiously suggest that robotic hepatectomy as an alternative to traditional open hepatectomy in selective cases for pediatric patients. Further, robotic hepatectomy could be applicable to liver malignancy of pediatrics as well.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.D.Y.
Data curation: P.J., H.S.
Supervision: K.D.Y.
Writing – original draft: P.J.
Writing – review & editing: P.J., K.H., N.J.M., K.D.Y.
