
 , Dayoung Ko2, Eun-Jung Koo2, Hyunhee Kwon2, Dae Yeon Kim2, Soo-Hong Kim2, Wontae Kim2, Hae-Young Kim2, Hyun Young Kim2, Seong Chul Kim2, Younghyun Na2, Jung-Man Namgoong2, So Hyun Nam2, Sungjoo Park2, Junbeom Park2, Jinyoung Park2, Tae-Jun Park2, Jeong-Meen Seo2, Ji-Young Sul2, Joonhyuk Son2, Hyun Beak Shin2, Joohyun Sim2, Jung-Tak Oh2, Chaeyoun Oh2, Joong Kee Youn2, Sanghoon Lee2, Ju Yeon Lee2, Cheolgu Lee2, Kyong Ihn2, Eunyoung Jung2, Jae Hee Chung2, Yong-Hoon Cho2, Yun Mee Choe2, Soo Jin Na Choi2, Seok Joo Han2, In Geol Ho2
, Dayoung Ko2, Eun-Jung Koo2, Hyunhee Kwon2, Dae Yeon Kim2, Soo-Hong Kim2, Wontae Kim2, Hae-Young Kim2, Hyun Young Kim2, Seong Chul Kim2, Younghyun Na2, Jung-Man Namgoong2, So Hyun Nam2, Sungjoo Park2, Junbeom Park2, Jinyoung Park2, Tae-Jun Park2, Jeong-Meen Seo2, Ji-Young Sul2, Joonhyuk Son2, Hyun Beak Shin2, Joohyun Sim2, Jung-Tak Oh2, Chaeyoun Oh2, Joong Kee Youn2, Sanghoon Lee2, Ju Yeon Lee2, Cheolgu Lee2, Kyong Ihn2, Eunyoung Jung2, Jae Hee Chung2, Yong-Hoon Cho2, Yun Mee Choe2, Soo Jin Na Choi2, Seok Joo Han2, In Geol Ho2 
Purpose
This study provides insights into the prevalence at birth, clinical characteristics, and outcomes of gastroschisis and omphalocele in Korea over the past decade, addressing the lack of localized data despite advanced healthcare capabilities.
Methods
The study retrospectively analyzed data from 20 pediatric surgical centers in Korea from January 2012 to December 2021, including 269 patients diagnosed with gastroschisis or omphalocele. Data variables included gender, gestational age, birth weight, associated anomalies, type of defect, surgical interventions, and outcomes.
Results
The study covered 269 patients, with 80 gastroschisis and 189 omphalocele cases. Gastroschisis prevalence at birth remained stable at 2.15 per 100,000 live births, while omphalocele increased to 5.08 per 100,000. Both conditions had similar gender ratios (0.95). Gastroschisis patients had lower birth weights (2,463.90±505.50 g) and smaller head circumferences (31.97±1.86 cm) compared to omphalocele patients (2,757.65±761.24 g, 32.78±2.64 cm). Omphalocele cases had more associated anomalies, especially cardiovascular issues. Prenatal diagnosis rates were high: 93.7% for gastroschisis and 86.4% for omphalocele. About 96.3% of gastroschisis and 84.1% of omphalocele patients were born in their treatment hospitals. Gastroschisis patients underwent surgery sooner (average 3.5 days) and started feeding later (16.5 days) than omphalocele patients (average 56.5 days to surgery, 6.6 days to start feeding). Hospital stays and follow-up durations were similar, averaging around 782.6 days for gastroschisis and 800.3 days for omphalocele patients. Survival rates were 89.7% for gastroschisis and 87.1% for omphalocele.
Conclusion
The study highlights the need for early diagnosis, centralized care, and specialized surgical approaches to optimize outcomes for gastroschisis and omphalocele patients in Korea. Enhanced prenatal screening and surgical protocols are recommended to improve these patients' prognosis.
This study provides insights into the prevalence at birth, clinical characteristics, and outcomes of gastroschisis and omphalocele in Korea over the past decade, addressing the lack of localized data despite advanced healthcare capabilities.
The study retrospectively analyzed data from 20 pediatric surgical centers in Korea from January 2012 to December 2021, including 269 patients diagnosed with gastroschisis or omphalocele. Data variables included gender, gestational age, birth weight, associated anomalies, type of defect, surgical interventions, and outcomes.
The study covered 269 patients, with 80 gastroschisis and 189 omphalocele cases. Gastroschisis prevalence at birth remained stable at 2.15 per 100,000 live births, while omphalocele increased to 5.08 per 100,000. Both conditions had similar gender ratios (0.95). Gastroschisis patients had lower birth weights (2,463.90±505.50 g) and smaller head circumferences (31.97±1.86 cm) compared to omphalocele patients (2,757.65±761.24 g, 32.78±2.64 cm). Omphalocele cases had more associated anomalies, especially cardiovascular issues. Prenatal diagnosis rates were high: 93.7% for gastroschisis and 86.4% for omphalocele. About 96.3% of gastroschisis and 84.1% of omphalocele patients were born in their treatment hospitals. Gastroschisis patients underwent surgery sooner (average 3.5 days) and started feeding later (16.5 days) than omphalocele patients (average 56.5 days to surgery, 6.6 days to start feeding). Hospital stays and follow-up durations were similar, averaging around 782.6 days for gastroschisis and 800.3 days for omphalocele patients. Survival rates were 89.7% for gastroschisis and 87.1% for omphalocele.
The study highlights the need for early diagnosis, centralized care, and specialized surgical approaches to optimize outcomes for gastroschisis and omphalocele patients in Korea. Enhanced prenatal screening and surgical protocols are recommended to improve these patients' prognosis.
Gastroschisis and omphalocele represent two of the most significant congenital abdominal wall defects confronting pediatric surgeons worldwide [1]. These conditions not only pose substantial challenges in surgical management but also have profound implications for neonatal care, long-term morbidity, and parental support. Although both result from errors during the embryologic development of the fetal abdominal wall, gastroschisis and omphalocele are unique disorders with different clinical sequelae. Gastroschisis is generally a solitary anomaly with postnatal outcomes related to the underlying integrity of the prolapsed bowel. In contrast, omphalocele is frequently associated with other structural anomalies or genetic syndromes that contribute more to postnatal outcomes than the omphalocele defect itself [2]. The incidence and outcomes of gastroschisis and omphalocele vary significantly across different geographic regions and healthcare systems, influenced by factors such as prenatal diagnosis rates, surgical techniques, and postoperative care protocols. In Korea, despite advanced healthcare services and high rates of prenatal screening, comprehensive data on these congenital anomalies have been sparse and fragmented. The Korean Association of Pediatric Surgeons (KAPS) conducted a national survey of its members to assess the birth prevalence of gastroschisis and omphalocele and to analyze data regarding patient characteristics, the rate of associated anomalies, treatment and prognosis of gastroschisis and omphalocele in Korea over the last 10 years. The 2022 annual nationwide survey conducted by the KAPS focused on gastroschisis and omphalocele. The results were first discussed at the KAPS annual meeting in Yeosu on June 9–10, 2022.
The study included patients who had been treated for gastroschisis and omphalocele from January 2012 to December 2021. It was based on the Case Report Form (CRF), which included data on gender, gestational age, birth weight, any associated anomalies, type of defect, type of surgery, management, and outcome. The national survey using CRF was sent to the members of the KAPS and was completed in 20 pediatric surgical centers, totaling 269 patients. Follow-up data for these patients were also included in the study. Microsoft Excel (Microsoft, Redmond, WA, USA) was used for patient registry and data collection. All data were analyzed using the IBM SPSS version 27 statistical software (IBM Co., Armonk, NY, USA), and p-values <0.05 were considered statistically significant. The study protocol was approved by the Institutional Review Board (IRB) of Jeonbuk National University Hospital (IRB No. 2024-08-028).
Over the 10-year period from January 2012 to December 2021, a total of 269 patients were included in the study, comprising 80 cases of gastroschisis and 189 cases of omphalocele, treated across 20 pediatric surgical centers. The distribution of patients among these hospitals varied significantly, with the top two centers managing 47.6% of all cases (Fig. 1).
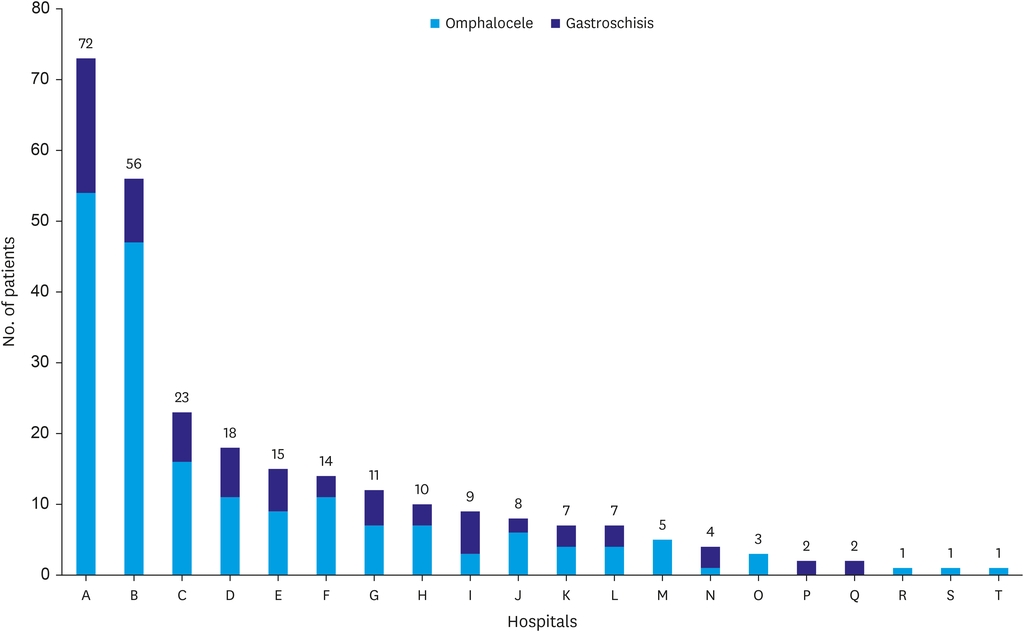
Fig. 1
Hospital distribution of gastroschisis and omphalocele cases. This figure illustrates the distribution of gastroschisis and omphalocele cases among 20 hospitals labeled from A to T. Each bar represents the total number of patients treated for omphalocele (blue) and gastroschisis (orange) at each hospital over the 10-year study period. Hospitals are ordered by the number of total cases they handled, with the largest volumes shown first.
The estimated prevalence rates of gastroschisis and omphalocele among live births in Korea showed notable differences. The prevalence at birth of omphalocele slightly increased over the study period, whereas the prevalence at birth of gastroschisis remained relatively stable. Specifically, the total prevalence rate for gastroschisis was 2.15 per 100,000 live births, and for omphalocele, it was 5.08 per 100,000 live births (Fig. 2, Table 1).
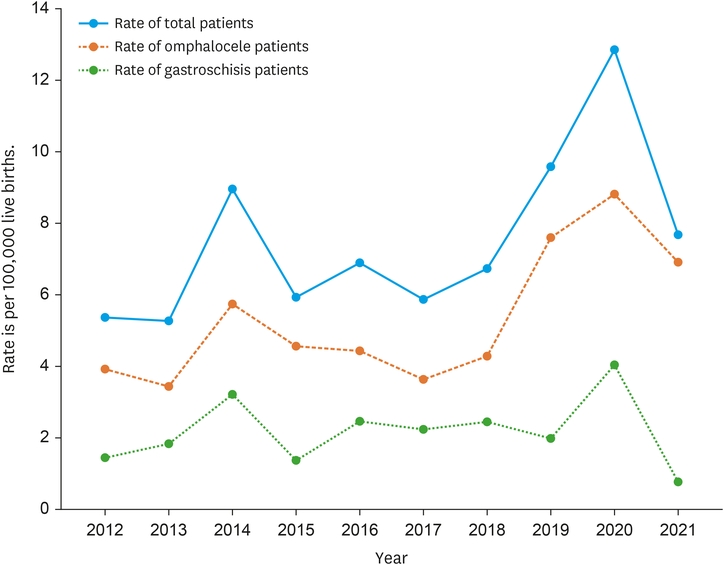
Fig. 2
Annual rate of gastroschisis and omphalocele per 100,000 live births. The graph displays the annual prevalence rates at birth of gastroschisis and omphalocele from 2012 to 2021. The blue line represents the rate of total patients, the orange line the rate of omphalocele patients and the green line the rate of gastroschisis patients, helping to illustrate trends over the study period.
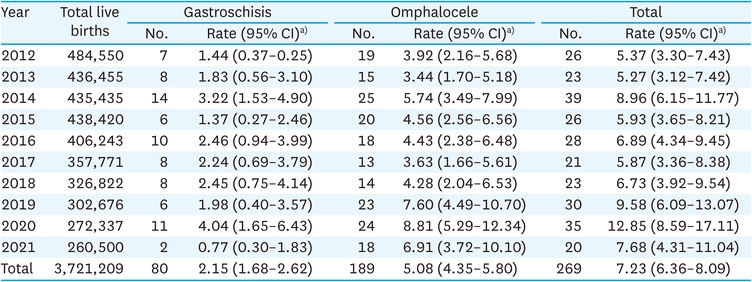
Table 1
Estimated prevalence at birth of gastroschisis and omphalocele among live births in Korea from national survey by the Korean Association of Pediatric Surgeons
The patient demographics and characteristics highlighted several key differences between gastroschisis and omphalocele cases (Table 2). Both conditions had a similar male-to-female ratio (0.95), but there were significant differences in birth weight and head circumference. Infants with gastroschisis had a lower mean birth weight (2,463.90±505.50 g) compared to those with omphalocele (2,757.65±761.24 g) and a smaller mean head circumference (31.97±1.86 cm vs. 32.78±2.64 cm). The mean maternal and paternal ages were significantly younger in the gastroschisis group compared to the omphalocele group. The frequency of associated anomalies was significantly higher in omphalocele cases compared to gastroschisis cases. Specifically, cardiovascular anomalies were more prevalent in omphalocele patients. Other anomalies such as gastrointestinal, genitourinary, musculoskeletal, chromosomal, and unspecified syndromes were also observed but with less statistical significance (Table 2).
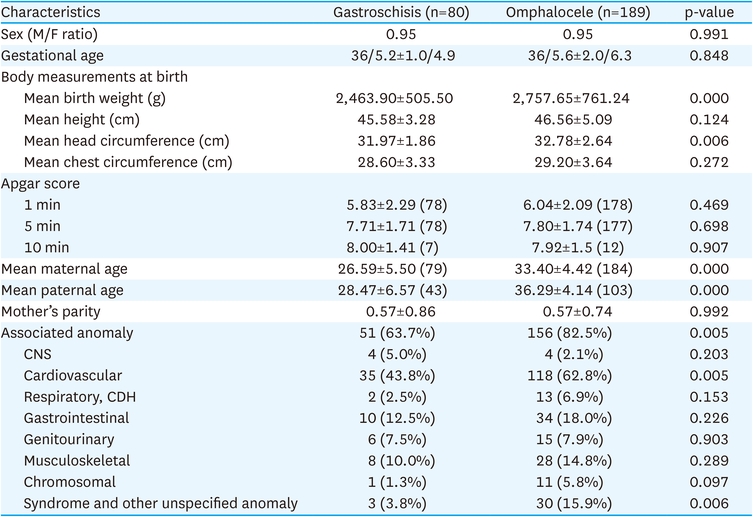
Table 2
Patients demographics and characteristics
Antenatal diagnosis via ultrasound was high for both conditions, with 93.7% of gastroschisis cases and 86.4% of omphalocele cases being diagnosed before birth. Antenatal counselling was performed in 45 (60.8%) patients in gastroschisis and 83 (52.2%) patients in omphalocele (Table 3).
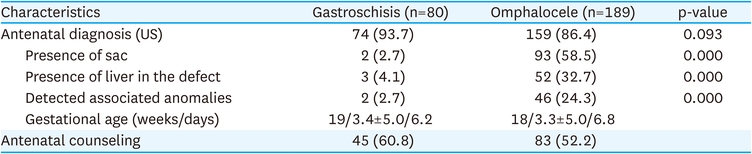
Table 3
Antenatal findings of gastroschisis and omphalocele patients from the national survey by the Korean Association of Pediatric Surgeons
When comparing associated anomalies diagnosed in the prenatal period with the associated anomalies diagnosed after birth, 43 (89.6%) of 48 patients diagnosed with associated anomalies in the prenatal period were found to have associated anomalies after birth, and 48 (24.9%) of 193 patients diagnosed with no associated anomalies in the prenatal period were found to have no associated anomalies after birth. As a result, the diagnosis of associated anomalies in prenatal period was confirmed to have high sensitivity but low specificity (Table 4).

Table 4
Comparison of associated anomalies diagnosed in the prenatal and the postnatal period of gastroschisis and omphalocele patients
There was a significant difference in the place of birth, with 96.3% of gastroschisis patients being born in the hospital where they received treatment compared to 84.1% of omphalocele patients (p=0.006). The mode of delivery did not differ significantly between the two groups, with planned and emergency C-sections and vaginal deliveries being relatively similar (Table 5).
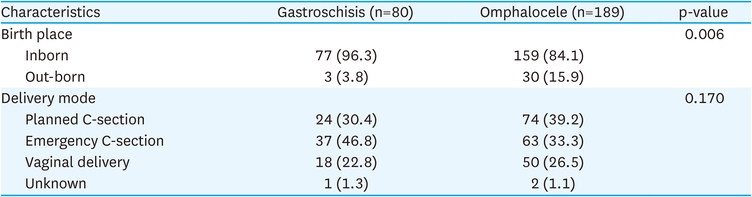
Table 5
Obstetric delivery outcomes for gastroschisis and omphalocele patients
Gastroschisis was an abdominal wall defect, located right side to a normal umbilicus, and not involving the umbilical ring. The herniated viscera were often covered by exudate but never by membranes and the status of bowel was normal in 22 (27.5%) patients and abnormal in 54 (67.5%). In gastroschisis, the organs of eviscerated contents were 78 (97.5%) in intestine, 8 (10.0%) in gonad, and 7 (8.6%) in liver (Table 6).
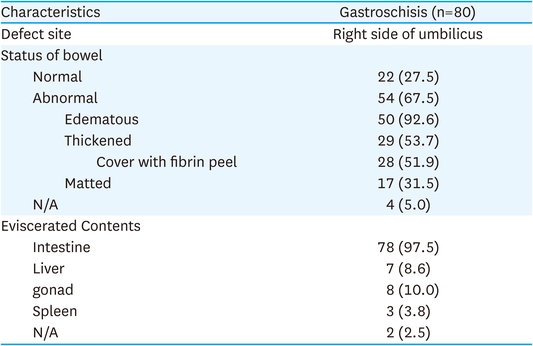
Table 6
Clinical characteristics of patients with gastroschisis
Omphalocele was an abdominal wall defect limited to an open umbilical ring. The viscera was herniated into the base of the umbilical cord and was covered by membranes or remnants of membranes that could be called sac in all patients. During the investigation period, there were 22 (11.6%) patients where sac was ruptured in omphalocele. In omphalocele, the organs of the content in the sac were 153 (81.0%) in intestine, 96 (50.8%) in liver, and 8 (4.2%) in spleen (Table 7).
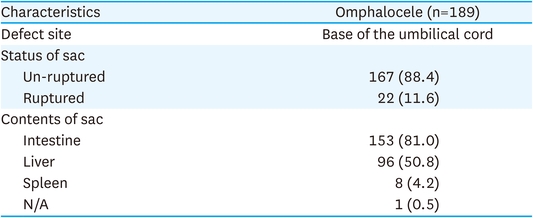
Table 7
Clinical characteristics of patients with omphalocele
In this study, the treatment approaches for 80 patients with gastroschisis included primary closure and staged closure techniques. Comparing both treatment approaches, 42 patients underwent staged closure, 36 underwent primary closure, and 2 were not applicable. For the primary closure techniques, fascial closure was performed on 34 patients, with 19 undergoing manual stretching of the abdominal wall and 11 having cosmetic umbilicoplasty. Skin closure was performed on 2 patients. The majority of procedures were conducted in the operating room (33 cases), while 3 were done in the delivery room. For the staged closure techniques, regarding the use of a prostatic silo, 39 patients utilized it with variations such as the Alexis wound protector (18 cases), Ioban surgical drape (6 cases), Pharm elastic/silicone sheeting (6 cases), Dacron-reinforced silastic (4 cases), saline bag (2 cases), and 3 were not applicable. Three patients did not use the prosthetic silo. For cases where a prosthetic silo was used, reduction was performed using various methods such as long clamps suspended by umbilical tape (11 cases), running sutures back and forth (9 cases), umbilical cord clamps (5 cases), ties (2 cases), and other methods (2 cases). Secondary surgeries were necessary for some patients. One patient who underwent primary closure required a second surgery involving fascial closure. For 21 patients who underwent staged closure, the second surgery included additional procedures such as fascial closure (15 cases), cosmetic umbilicoplasty (7 cases), skin flaps with grafting (2 cases), re-application of the silo (2 cases), skin suturing with undermining (2 cases), and an operation for ileal perforation with subsequent loop ileostomy (1 case) (Fig. 3).
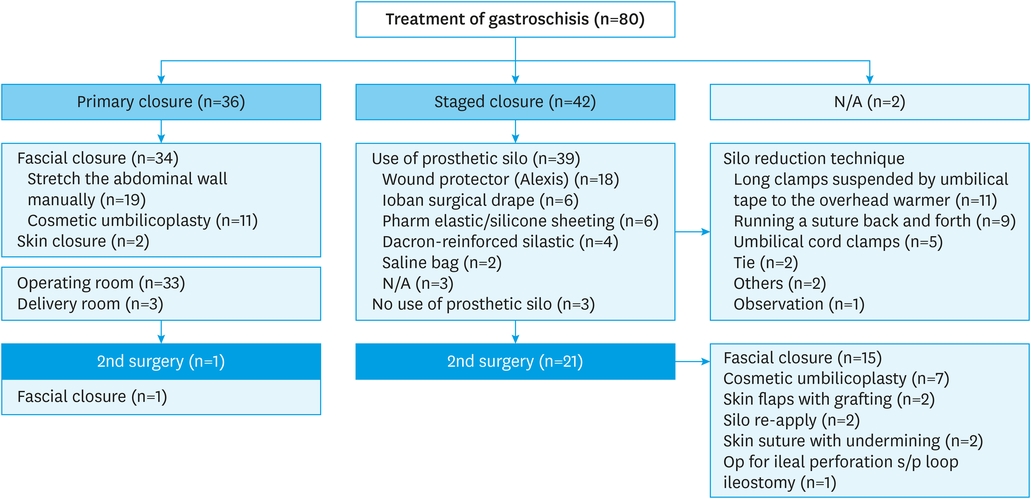
Fig. 3
Treatment approaches for gastroschisis patients. This detailed chart outlines the treatment methods for 80 patients with gastroschisis, comparing primary closure and staged closure techniques. It includes specifics such as the use of prosthetic silo types and second surgeries performed, highlighting the different surgical interventions and their frequencies.
N/A, not applicable.
The study analyzed treatment methods for 189 patients with omphalocele, including primary closure, staged closure, and non-operative approaches. Of the total patients, 159 underwent primary closure, 14 underwent staged closure, 13 received non-operative treatment, and 3 were not applicable. For primary closure techniques, fascial closure was performed in 152 patients, with 67 undergoing manual stretching of the abdominal wall and 104 receiving cosmetic umbilicoplasty. Additionally, 4 patients had absorbable mesh, and 3 had Gore-Tex. Fascial closure was not performed in 7 patients; of these, 3 had skin closure only, 2 used absorbable mesh, and 3 were not applicable. In the staged closure group, various types of prosthetic silos were used: Pharm Elastic/silicone sheeting in 6 cases, the Alexis wound protector in 2 cases, Duoderm on the sac in 1 case, and 5 were not applicable. Additionally, 9 patients died before the operation, and 4 did not undergo surgery. After the first-line treatment, including primary closure and staged closure, secondary surgeries were required for 15 patients, including fascial closure in 13 cases, cosmetic umbilicoplasty in 5 cases, absorbable mesh in 2 cases, an operation for jejunal atresia in 1 case, and an operation for wound dehiscence in 1 case. Initial management involved different painting methods, with 55 cases using a solution of 0.25% mercurochrome, Silvadene, and 0.5% silver nitrate, 23 cases using Betadine, and 18 cases using other methods (Fig. 4).
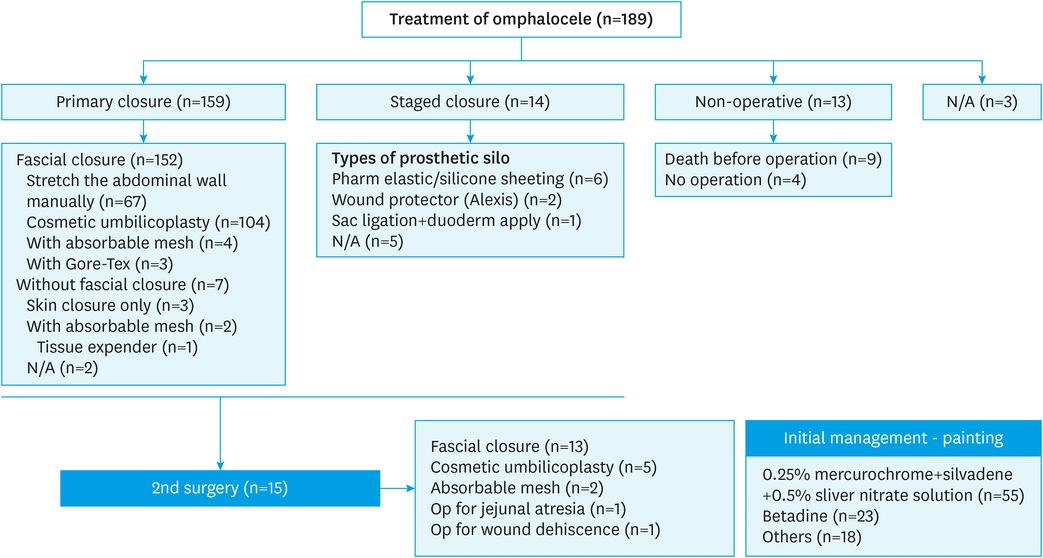
Fig. 4
Treatment approaches for omphalocele patients. This figure summarizes the treatment strategies for 189 omphalocele patients, distinguishing between primary closure, staged closure, non-operative approaches, and detailing second surgery interventions. It also notes the initial management techniques used, providing a comprehensive view of therapeutic approaches.
N/A, not applicable.
The study analyzed the clinical characteristics of 80 patients with gastroschisis and 189 patients with omphalocele. Key findings include: The time from birth to operation was significantly different between the two groups, with gastroschisis patients having an average of 3.5±6.3 days and omphalocele patients having an average of 56.5±129.0 days. Similarly, the time to start feeding was significantly longer for gastroschisis patients at 16.5±11.9 days compared to 6.6±5.8 days for omphalocele patients. The length of hospital stay was not significantly different between the two groups, with gastroschisis patients having an average stay of 45.6±52.5 days and omphalocele patients having an average stay of 37.5±52.6 days. The follow-up duration was also similar, with gastroschisis patients having an average of 782.6±756.9 days and omphalocele patients having an average of 800.3±740.9 days (Table 8).

Table 8
Clinical characteristics of patients with gastroschisis and omphalocele
The survival rate for patients with gastroschisis is 0.897. For patients with omphalocele, the survival rate is 0.871. The difference in survival rates between gastroschisis and omphalocele is not statistically significant, with a p-value of 0.857 (Fig. 5).
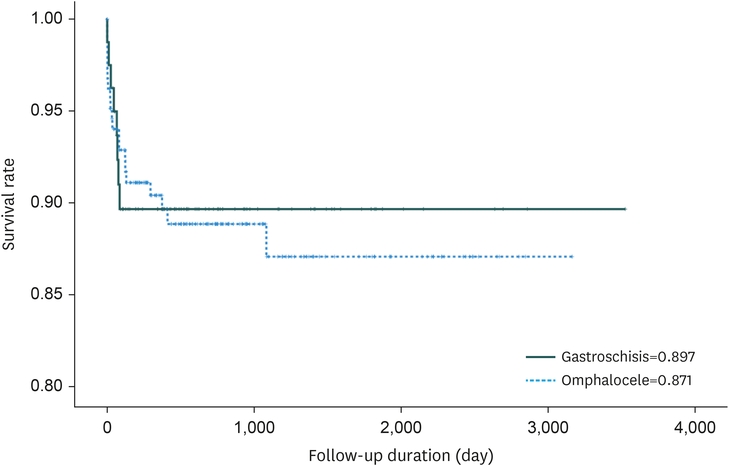
Fig. 5
Survival rates for gastroschisis and omphalocele patients. The bar graph compares the survival rates of gastroschisis and omphalocele patients, with gastroschisis shown in black (89.7%) and omphalocele in blue (87.1%). This visual representation aids in understanding the slight but not statistically significant, differences in survival outcomes between the two conditions (p=0.857).
The study presents comprehensive data on the incidence, clinical characteristics, and outcomes of gastroschisis and omphalocele in Korea over a ten-year period. This retrospective analysis, based on data collected from 20 pediatric surgical centers, highlights several key findings that contribute to our understanding of these congenital abdominal wall defects. When compared with international data, several noteworthy similarities and differences emerge, shedding light on the global landscape of these congenital anomalies.
The study reveals that the prevalence rates of gastroschisis and omphalocele among live births in Korea are 2.15 per 100,000 and 5.08 per 100,000, respectively. The data shows a higher prevalence at birth of omphalocele compared to gastroschisis, a pattern also observed in other regions [1, 3, 4, 5]. However, in other regions, there was a pattern where the incidence of gastroschisis was higher compared to omphalocele [6, 7, 8, 9, 10, 11, 12]. The study revealed a slight increase in the prevalence at birth of omphalocele and a stable prevalence at birth of gastroschisis in Korea over the decade. These rates are inconsistent with global trends reported in previous studies, which indicate that while the incidence of gastroschisis has been increasing in many countries, the prevalence at birth of omphalocele has remained relatively stable [4, 11].
The characteristics of gastroschisis and omphalocele in Korea mirrors global trends, with gastroschisis being more common in younger mothers and associated with fewer additional anomalies compared to omphalocele. Studies from other studies support this, indicating that gastroschisis typically presents in younger mothers and with lower birth weights compared to omphalocele [1, 4, 8, 11]. Conversely, omphalocele is often linked with older maternal age and a higher prevalence at birth of associated anomalies, such as cardiac defects and chromosomal abnormalities, consistent with findings from our study [1, 4, 8, 11].
In our study, the mean parity of mothers of infants with gastroschisis or umbilical aneurysm was approximately 0.57, indicating a relatively higher number of nulliparous mothers in the cohort (Table 2). These data differ from the broader observation in various studies that younger, non-parietal women were more often associated with the development of gastroschisis than with omphalocele [4, 8, 13].
The sex ratio of abdominal wall defects, specifically gastroschisis and omphalocele, provides insight into their epidemiological characteristics. In the provided demographic data from Table 2 of your study, both conditions showed an almost equal male to female ratio (M/F ratio=0.95). This balanced gender distribution suggests no significant sex predilection for these congenital anomalies in the population studied, and other studies have found similar findings [1, 4, 7].
The study underscores significant differences in the clinical characteristics between gastroschisis and omphalocele patients. Infants with gastroschisis had a lower mean birth weight and smaller head circumference compared to those with omphalocele. This is consistent with previous literature that associates gastroschisis with low birth weight and smaller head size, which are critical factors influencing neonatal outcomes [3].
The prevalence at birth and nature of associated anomalies in abdominal wall defects like omphalocele and gastroschisis are critical for understanding the clinical outcomes and guiding prenatal counseling and postnatal care strategies. In our study, the frequency of associated anomalies was significantly higher in omphalocele cases (82.5%) compared to gastroschisis (63.7%), with cardiovascular anomalies particularly more prevalent in omphalocele patients. Other studies are consistent with our findings of a high prevalence at birth of associated malformations, especially cardiovascular disease, in umbilical herniation, suggesting a pattern in which umbilical herniation is often part of a more complex syndrome presentation compared to gastric dissection [4, 12, 13]. In contrast, gastroschisis is typically an isolated defect, though it can still be associated with gastrointestinal complications [7, 12].
The prenatal diagnosis rates for gastroschisis and omphalocele are notably high, with gastroschisis diagnosed in 93.7% of cases and omphalocele in 86.4%. This reflects the efficacy of current antenatal ultrasound techniques in detecting these abdominal wall defects (Table 3). The data from this study indicate that while prenatal diagnosis of associated anomalies was confirmed postnatally in 43 out of 48 cases (89.6%), only 48 out of 193 cases (24.9%) that were not diagnosed with anomalies prenatally were found to be anomaly-free after birth (Table 4). This suggests a high sensitivity but low specificity in prenatal anomaly detection, which is consistent with broader trends observed in abdominal wall defects. Studies such as those conducted in Japan and reported by Watanabe et al. [14] also highlight the role of advanced prenatal screening, which has increasingly allowed for detailed assessment of not just the primary defect but also associated anomalies, impacting surgical planning and parental counseling [4]. In Japan, the antenatal detection rates have been significant, with similarly high sensitivity noted. The approach there also emphasizes the utility of detailed prenatal screening in improving postnatal outcomes [4]. The high sensitivity of anomaly detection in prenatal screenings for gastroschisis and omphalocele supports their utility in clinical practice. However, the challenge remains to enhance specificity to reduce the psychological and financial burden of false positives. Continual advancements in imaging technology and diagnostic protocols are essential to refine these outcomes.
Antenatal diagnosis of gastroschisis and omphalocele through ultrasound was notably high, with gastroschisis cases diagnosed at 93.7% and omphalocele cases at 86.4%. This high rate of detection allows for significant prenatal counseling, which was received by 60.8% of gastroschisis patients and 52.2% of omphalocele patients as shown in Table 3. The role of antenatal counseling in managing abdominal wall defects is pivotal as it helps in preparing parents for the outcomes and managing their expectations regarding the condition of their child. According to a study from New Zealand, effective parental counseling can impact parental perceptions of the defect and assist in guiding pregnancy management [12]. This includes preparing the parents for potential surgeries and the associated care that will be required postnatally [15].
The place of birth for patients with gastroschisis and omphalocele shows a significant difference. In this study, a notably higher proportion of gastroschisis patients (96.3%) were born in the hospital where they were treated compared to omphalocele patients (84.1%) (Table 5). This difference could reflect the urgency and the need for immediate postnatal care associated with gastroschisis, which often presents more acutely and requires rapid surgical intervention post-delivery. The mode of delivery, involving planned and emergency C-sections along with vaginal deliveries, showed no significant difference between the gastroschisis and omphalocele groups in this study (Table 5). This suggests that the decision on the mode of delivery might be influenced more by obstetric considerations rather than the type of abdominal wall defect. Consistent with this, literature suggests that the mode of delivery for abdominal wall defects should be guided by standard obstetric indications rather than the presence of the defect itself [7, 8, 12, 14].
The study details various treatment approaches for gastroschisis and omphalocele, including primary and staged closure techniques. The findings indicate that primary closure is more commonly performed in gastroschisis patients, while staged closure is often necessary for more complex cases or when primary closure is not feasible. Both gastroschisis and omphalocele treatments highlight a complex interplay between surgical techniques and the condition's severity. Primary closure often aims for immediate resolution, whereas staged closure prepares the anatomy for a more gradual recovery, potentially reducing immediate post-operative complications. The literature supports these approaches, emphasizing that while primary closure is ideal, the condition of the neonate and the defect's size often necessitate a staged approach to avoid complications like abdominal compartment syndrome, which is consistent with findings in advanced treatments such as vacuum-assisted closure (VAC) for complex cases where traditional methods fail [12, 15, 16, 17].
The study analyzing 80 patients with gastroschisis and 189 patients with omphalocele revealed significant differences in the time from birth to operation and the time to start feeding between the two groups, although the length of hospital stay and follow-up duration were similar for both conditions. The significantly shorter time from birth to operation for gastroschisis patients (average 3.5 days) compared to omphalocele patients (average 56.5 days) highlights the urgency and clinical necessity of early surgical intervention in gastroschisis. This urgency is often due to the exposed viscera in gastroschisis, which can lead to rapid fluid loss, temperature instability, and increased risk of infection and damage to the bowel [7]. On the other hand, the delay in operation for omphalocele could be attributed to the protective sac covering the herniated organs, which reduces the immediate postnatal risks and allows for more detailed preoperative planning and stabilization [7].
Gastroschisis patients experienced a significantly longer delay in starting feeding (average 16.5 days) compared to omphalocele patients (average 6.6 days). This is consistent with the nature of gastroschisis, where bowel exposure can often lead to complications such as bowel edema, atresia, or necrosis, delaying the initiation of enteral nutrition [12, 14]. Omphalocele patients, generally having their bowel covered and protected, can often commence feeding earlier, reflecting fewer immediate postnatal complications affecting the gastrointestinal tract [12, 14].
The length of hospital stays did not significantly differ between the groups, suggesting that while the initial conditions and interventions vary, the overall burden of care post-operation may converge, particularly when considering long-term monitoring and care for potential complications. Although not statistically significant, the hospitalization period was long in gastroschisis, which was similar to the findings seen in other studies [7, 12].
The survival rates for gastroschisis (89.7%) and omphalocele (87.1%) patients, as illustrated in Fig. 5, show no significant differences between the two conditions when optimal surgical and neonatal care are provided. Studies from Japan and other countries also demonstrate comparable survival outcomes, highlighting that advancements in prenatal diagnostics and postnatal care have significantly improved survival rates over the years for both conditions [4, 11].
In conclusion, this study provides valuable insights into the management and outcomes of gastroschisis and omphalocele in Korea. The findings underscore the importance of early diagnosis, centralized care, and tailored surgical approaches to improve patient outcomes. Future research should focus on long-term follow-up and the development of standardized treatment protocols to further enhance the care and prognosis of infants with these challenging congenital defects.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
