ABSTRACT
A ciliated foregut cyst is a rare developmental anomaly. It develops from the primitive foregut. It is usually located supra-diaphragmatically. Its localization in the gallbladder is very infrequent and has been sparsely reported. We report a rare case of a ciliated cyst of the gallbladder in an 11-year-old female, who presented with complaints of upper abdominal pain for 2 months. She was suspected to have gallbladder duplication or gallbladder diverticulum on imaging. The histopathology reported this anomaly as a ciliated foregut cyst. The ciliated cyst of the gallbladder is a benign congenital lesion. Abdominal ultrasonogram and computed tomography/magnetic resonance imaging are suggestive of a cystic lesion of the gallbladder. The definitive diagnosis is by histopathological examination. This is a rare clinicopathological condition in the pediatric age group. The recommended treatment is laparoscopic cholecystectomy. The role of conservative management has not been established due to the rarity of the condition.
-
Keywords: Ciliated foregut cyst; Laparoscopic cholecystectomy; Gallbladder diverticulum; Gall bladder duplication
INTRODUCTION
A ciliated foregut cyst (CFC) of the gallbladder is a rare developmental anomaly with only a handful of cases reported to date. This is the second pediatric case reported in the literature, as accessed by the authors. Several hypotheses exist regarding the origin of CFCs; however, the exact mechanism of their development is still obscure. They are thought to develop due to faulty selective cellular differentiation [
1]. It originates from various sites of the primitive foregut such as the oropharynx, broncho-pulmonary tract, esophagus, stomach, duodenum, liver, bile ducts, and pancreas. The ciliated cyst is usually supra-diaphragmatic and located in the bronchial tree, esophagus, and mediastinum. It can rarely have an infra diaphragmatic location, usually in the liver and occasionally the pancreas. However, its location in the gallbladder is exceptionally rare. To our knowledge, only 16 cases have been described in the literature to date.
CASE REPORT
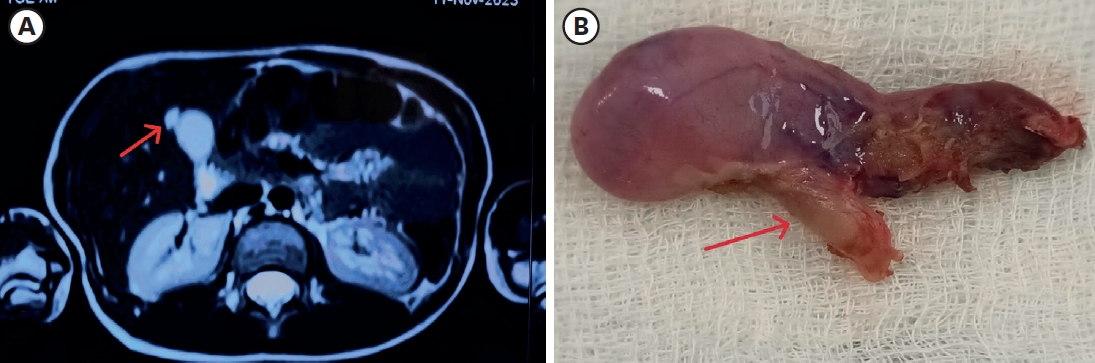
A 11-year-old girl, presented with dull aching pain in the right hypochondrium, along with decreased appetite for 2 months. There was no history of bilious vomiting, yellow discoloration of skin or sclerae, pruritis, or similar complaints in the family. The child had attained age-appropriate milestones, and her scholastic abilities were good. Her general physical examination and systemic examination were normal. Magnetic resonance cholangiopancreatography revealed a cystic lesion seen in continuity with the anterior wall of the gallbladder 1.4×0.5 cm showed focal outpouching measuring 9×5 mm arising from the right anterolateral wall of the body of the gallbladder, suggestive of gallbladder diverticulum (
Fig. 1A).
Complete hemogram was within normal limits (hemoglobin: 11.2 gm%, total leucocyte count: 12,000/mm
3, differential leucocyte count: polymorphs 55%, lymphocytes 39%, monocytes 4%, eosinophils 2%, platelets 180,000/mm
3). Liver function test and kidney function test did not reveal any significant derangement. Laparoscopic cholecystectomy was performed. Intraoperatively, the cyst was noted to be attached to the fundus of the gallbladder and was not adherent to the liver or the biliary tract. On gross examination, the gallbladder measured 7×2.5×1.5 cm (
Fig. 1B). A cyst of size 1×1 cm was noted attached to the fundus of the gallbladder.
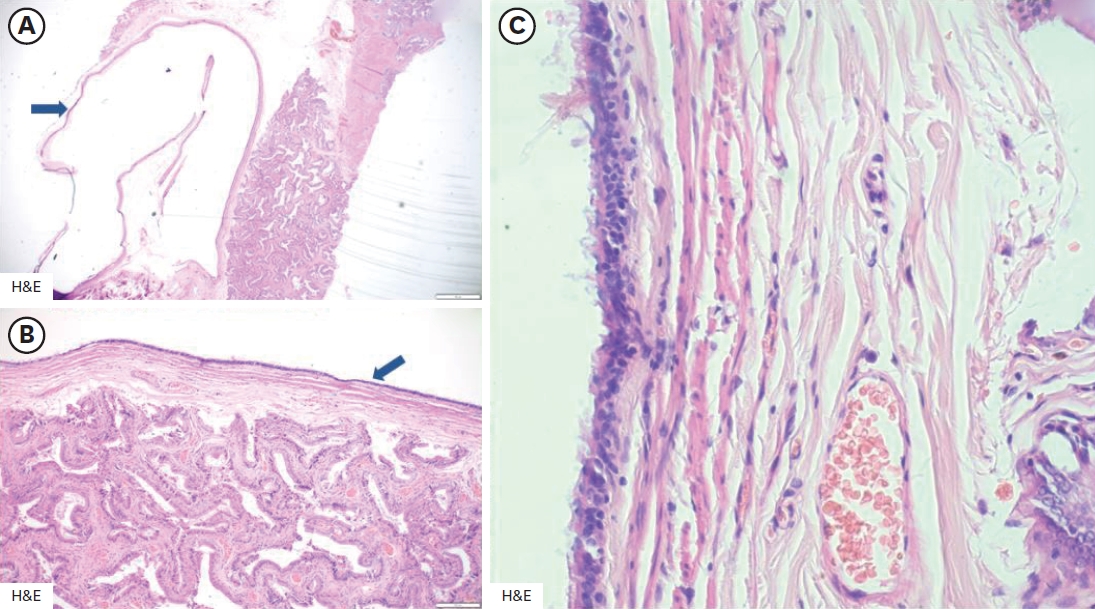
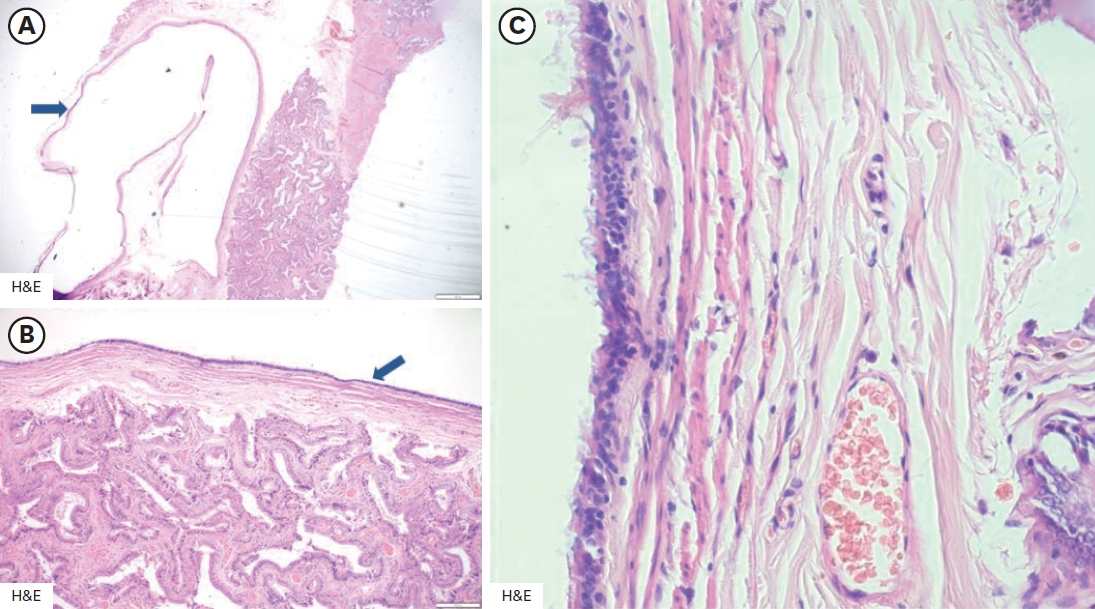
The cyst was unilocular and filled with thick mucoid material. The wall of the cyst was thin with a smooth glistening inner surface. The mucosal surface of the gallbladder was velvety and bile-stained. Microscopically, the cyst was located in the sub-serosa. The cyst wall was lined by a single layer of ciliated tall columnar pseudostratified epithelium resting on a smooth muscle layer (
Fig. 2). There was no metaplasia, dysplasia, or malignancy present in the lining epithelium. A diagnosis of a ciliated foregut cyst of the gallbladder was made. The postoperative course of the patient was uneventful. She was discharged on postoperative day 2 and is presently doing well at 6 months follow-up.
Approval from institutional ethics committee taken and consent from patient and parents taken for participation. Consent from patient and parents taken for publication.
DISCUSSION
Cystic lesions of the gallbladder are rare and they can be congenital, acquired, or neoplastic [
2]. Kakitsubata et al. [
3] in 1995, described the first case of a gallbladder cyst with cylindrical ciliated epithelium and described it as the “Epithelial cyst of the gallbladder.” The term “Ciliated foregut cyst of the gallbladder” was coined by Nam et al. [
4].
The ciliated foregut cyst is a benign lesion that develops from the primitive foregut [
5]. Several hypotheses describe the pathogenesis of these ciliated cysts [
6]. Faulty selective cellular differentiation is probably the cause of this rare anomaly [
1].
CFCs can be either supra-diaphragmatic or infra-diaphragmatic. They originate from various sites of the primitive foregut such as the oropharynx, broncho-pulmonary tract, esophagus, stomach, duodenum, liver, bile ducts, and pancreas. The majority of CFCs are supra-diaphragmatic and are located in the bronchial tree, esophagus, and mediastinum. Rarely, they may be present in the infra-diaphragmatically, usually in the liver and occasionally the pancreas. However, its location in the gallbladder is exceptionally rare.
Only 16 cases (out of which only 1 pediatric case of a 9-year-old male child) have been reported. It is predominantly reported in females with an incidence of female to male being 2:1. The condition has been commonly described in the 4th to the 7th decade. The most frequent location reported is the neck of the gallbladder. The most frequent clinical symptom is pain which was noted in 6 patients. In 5 cases, the discovery of the gallbladder cyst was incidental.
In the review of the literature of the reported cases, all patients underwent radiologic exams preoperatively. In the majority of cases, it was reported as a cystic lesion. In the remaining, it was reported as gallbladder stones, acute cholecystitis, diverticula, or duplication of the gallbladder. In our patient, the gallbladder lesion was mistakenly interpreted as a diverticulum of the gallbladder.
In all the reported cases, the cyst was unilocular. In most cases, the cyst content was mucoid (9 patients) while gelatinous in 2 patients, dark brown in 2 others, and milky in one patient. In our case, it was mucoid content.
Histopathologically, the cystic lesion is characterized by a thin wall covered with a ciliated pseudostratified mucus-secreting epithelium, which lays on connective tissue containing smooth muscular fibers. There is no communication between the cyst and the gallbladder lumen.
In imaging techniques, abdominal ultrasound was the most commonly performed study. Although it is not very specific, the ciliated cyst was mostly reported as an anechogenic and sometimes as a hyperechogenic lesion. When the lesion is hyperechogenic, it should be suspected to be a neoplastic lesion [
7], especially when the size of the cyst exceeds 1 cm. In this scenario, an abdominal magnetic resonance imaging (MRI) is useful for detailed review. The ciliated cyst is often reported as a hyperintense lesion in the T1 and T2 phases of MRI, however, sometimes the cyst can appear hypointense in the T1 phase. This in turn depends on the viscosity of the cyst content and the presence or absence of calcium and cholesterol crystals.
Although, Tunçyürek et al. [
7] proposed close surveillance when the cyst is silent, elective laparoscopic cholecystectomy is a standard treatment protocol since the distinction between benign and malignant lesions is difficult on imaging techniques and malignant metaplasia and epidermoid carcinoma have been observed in hepatic ciliated cysts [
8].
To the best knowledge of the authors, this is the 2nd case of a ciliated foregut cyst of the gallbladder in a child.
The ciliated foregut cyst of the gallbladder is a rare congenital cyst. The preoperative diagnosis is still difficult to establish with radiologic imaging. The definitive diagnosis is established by histopathological analysis. The recommended current treatment is laparoscopic cholecystectomy. The role of conservative management has not been established due to the rarity of this case and the possibility of malignant degeneration. Hence awareness of this entity is important for both pediatric surgeons and radiologists to suspect it preoperatively.
NOTES
-
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
-
Author Contributions
Conceptualization: P.N.J.; Data curation: R.S.B.L., S.J.; Formal analysis: R.S.B.L., G.K.; Investigation: P.N.J., R.S.B.L.; Methodology: R.S.B.L.; Supervision: P.N.J.; Writing - original draft: R.S.B.L., P.N.J.; Writing - review & editing: R.S.B.L., P.N.J., S.J., S.S., G.K., K.R.P., M.J.K.
Fig. 1.(A) Illustration showing a diverticulum originating from the right anterolateral wall of the gallbladder body, indicative of gallbladder diverticulosis. (B) Laparoscopic cholecystectomy specimen showing a cyst (1×1 cm) attached to the fundus of the gallbladder, which measured 7×2.5×1.5 cm and was not adherent to surrounding structures.
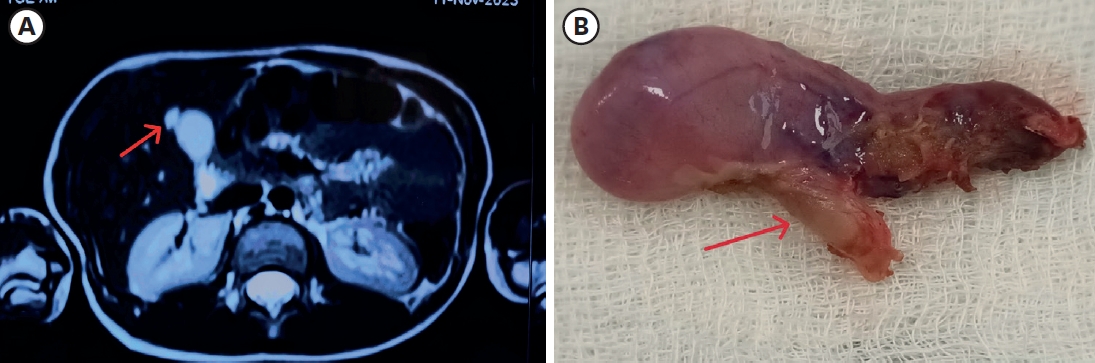
Fig. 2.
(A) H&E stain showing a unilocular cyst filled with thick mucoid material, with a smooth, glistening inner surface. (B) H&E stain at higher magnification demonstrating the cyst wall lined by a single layer of ciliated tall columnar epithelium. (C) H&E stain highlighting the pseudostratified ciliated epithelium over a smooth muscle layer, with no areas of metaplasia, dysplasia, or malignancy.
H&E, hematoxylin and eosin.
REFERENCES
- 1. Lee MJ, Salinas J, Varikatthas W, Alsnih G. A rare gallbladder ciliated foregut cyst in chronic cholecystitis. Int J Surg Case Rep 2016;20:155-8.
- 2. Robertson HE, Ferguson WJ. The diverticula (Luschka’s crypts) of the gallbladder. Arch Pathol (Chic) 1945;40:312-33.
- 3. Kakitsubata Y, Kakitsubata S, Marutsuka K, Watanabe K. Epithelial cyst of the gallbladder demonstrated by ultrasonography: case report. Radiat Med 1995;13:309-10.
- 4. Nam ES, Lee HI, Kim DH, Choi CS, Kim YB, Kim JS, et al. Ciliated foregut cyst of the gallbladder: a case report and review of the literature. Pathol Int 2000;50:427-30.
- 5. Sadler TW, Langman J. Langman’s medical embryology. 8th ed. Philadelphia (PA): Lippincott Williams &Wilkins; 2005.
- 6. Cureton RJ, Newcombe JF. Multilocular cyst of the gall-bladder. Br J Surg 1961;48:577-80.
- 7. Tunçyürek Ö, Nart D, Yaman B, Buyukcoban E. A ciliated foregut cyst in a gallbladder: the smallest recorded. Jpn J Radiol 2013;31:412-8.
- 8. Oida T, Mimatsu K, Kawasaki A, Kuboi Y, Kanou H, Amano S. Laparoscopic excision for an enlarged ciliated hepatic foregut cyst as a minimally invasive procedure. J Laparoendosc Adv Surg Tech A 2009;19:203-6.
Citations
Citations to this article as recorded by