ABSTRACT
Benign cystic mesothelioma (BCM) is a rare intra-abdominal tumor and is particularly uncommon in pediatric patients. Its nonspecific clinical and radiological features often make preoperative diagnosis challenging. We report the case of a 4-year-old girl who presented with acute abdominal pain and vomiting. Computed tomography revealed a large, multiloculated cystic mass occupying the lower abdomen, which was initially suspected to be a lymphatic malformation. During laparoscopic exploration, a hemorrhagic, multiloculated cystic mass with hemoperitoneum was identified and completely resected with preservation of the right ovary. Histopathological examination confirmed BCM, showing predominant clusters of epithelioid cells interspersed with cyst-like spaces on hematoxylin and eosin staining. The patient recovered uneventfully and had no recurrence during 30 months of follow-up. This case describes an unusual presentation of BCM as an acute abdomen complicated by hemoperitoneum in a child and emphasizes the importance of surgical exploration and histopathological evaluation in establishing the diagnosis.
-
Keywords: Benign cystic mesothelioma; Pediatric; Pediatric tumor; Case reports
INTRODUCTION
Among intra-abdominal cystic lesions, benign cystic mesothelioma (BCM) of the peritoneum is a rare tumor that arises from the peritoneal mesothelium lining the serous cavity. Its clinical symptoms are nonspecific, and definitive diagnosis requires histological confirmation. Although BCM is classified as benign, it may show locally aggressive behavior and carry a high local recurrence rate. To date, no evidence-based treatment strategy has been established for BCM. Here, we report a rare case of intra-abdominal BCM in a 4-year-old girl and emphasize the importance of considering BCM in the differential diagnosis of cystic abdominal lesions in children.
CASE REPORT
Ethics statement
Written informed consent for publication of this case report and the accompanying images was obtained from the patient’s parent. This case report was prepared in accordance with the principles of the Declaration of Helsinki and the CARE guidelines.
Patient information
A 4-year-old girl presented to the emergency department with abdominal pain, abdominal distension, and vomiting that had persisted for 5 days. She had initially been treated for enterocolitis at a local clinic. Although the vomiting had subsided 2 days before presentation, her oral intake remained poor.
Clinical and diagnostic findings
The patient appeared lethargic and was crying because of persistent periumbilical pain. Physical examination revealed a soft but distended abdomen, with a firm mass palpable in the right abdomen. She was hemodynamically stable. Initial laboratory evaluation was unremarkable except for an elevated erythrocyte sedimentation rate of 58 mm/hr. Contrast-enhanced computed tomography (CT) demonstrated a large, multiloculated cystic mass measuring approximately 10×12 cm, occupying nearly the entire lower abdomen and pelvic cavity (
Fig. 1). The mass showed no enhancement after intravenous contrast administration and had no communication with the abdominal viscera. Based on these findings, an intra-abdominal lymphatic malformation originating from the omentum or peritoneum was suspected.
Emergency surgery was performed because of persistent abdominal pain, progressive distension, and suspected intra-abdominal bleeding. Laparoscopic exploration was performed using two 5-mm trocars placed at the umbilicus and left lower quadrant and one 3-mm trocar placed in the suprapubic area. Intraoperatively, bloody ascites was identified, along with a hemorrhagic cystic mass measuring approximately 15×15 cm and showing no communication with adjacent viscera. Extracorporeal aspiration of the mass was attempted but was ineffective because of internal septations and organized blood clot. After intracorporeal decompression and shrinkage of the tumor, the mass was found to be attached to the right ovary. Careful dissection enabled complete resection with ovarian preservation, and the specimen was retrieved using an endoscopic bag (
Fig. 2). The left ovary was intact, and no bowel or omental abnormalities were observed.
The patient resumed oral intake on the first postoperative day and was discharged on postoperative day 4 without complications. The pathological diagnosis was benign multicystic mesothelioma of the peritoneum (
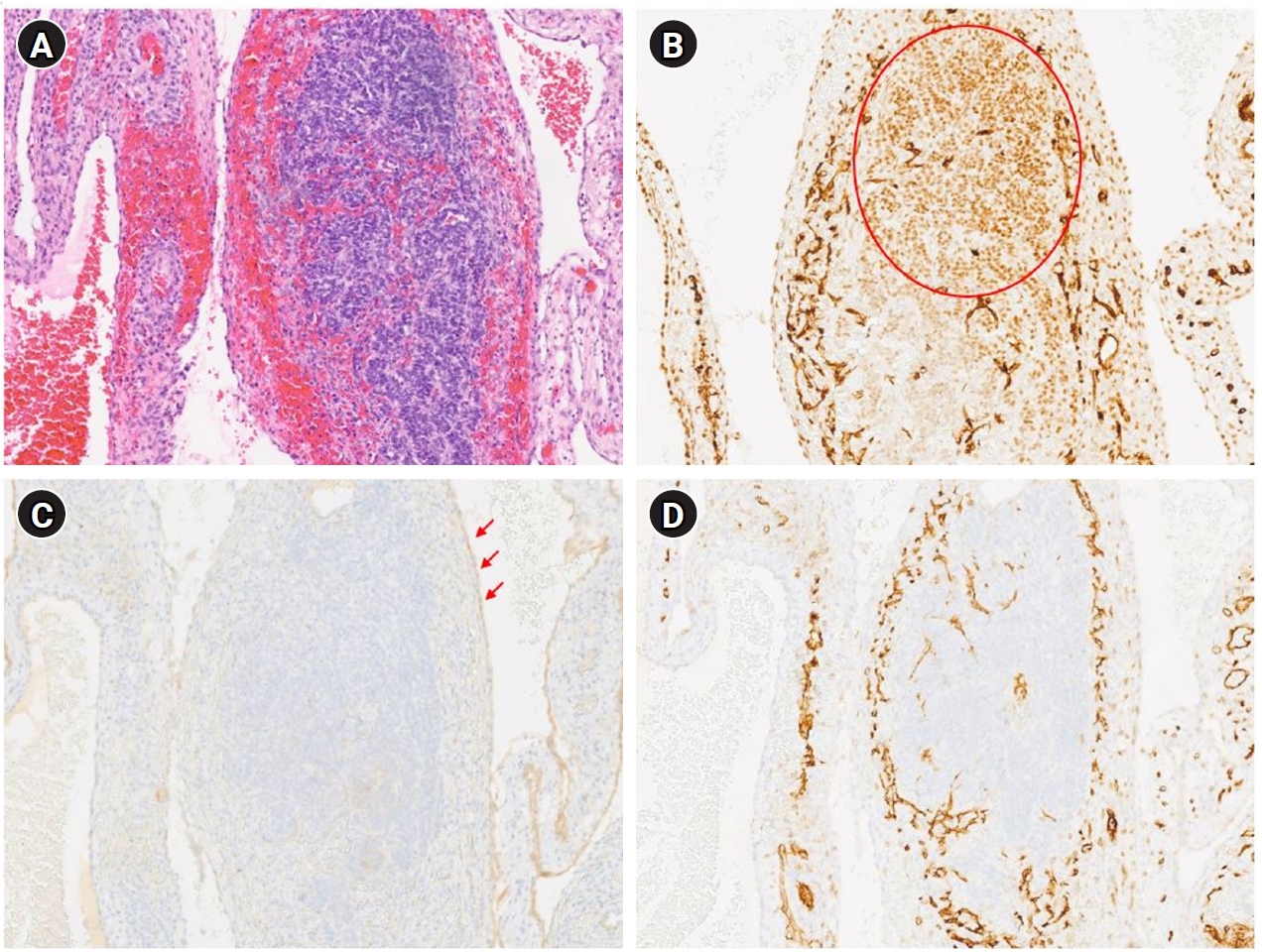
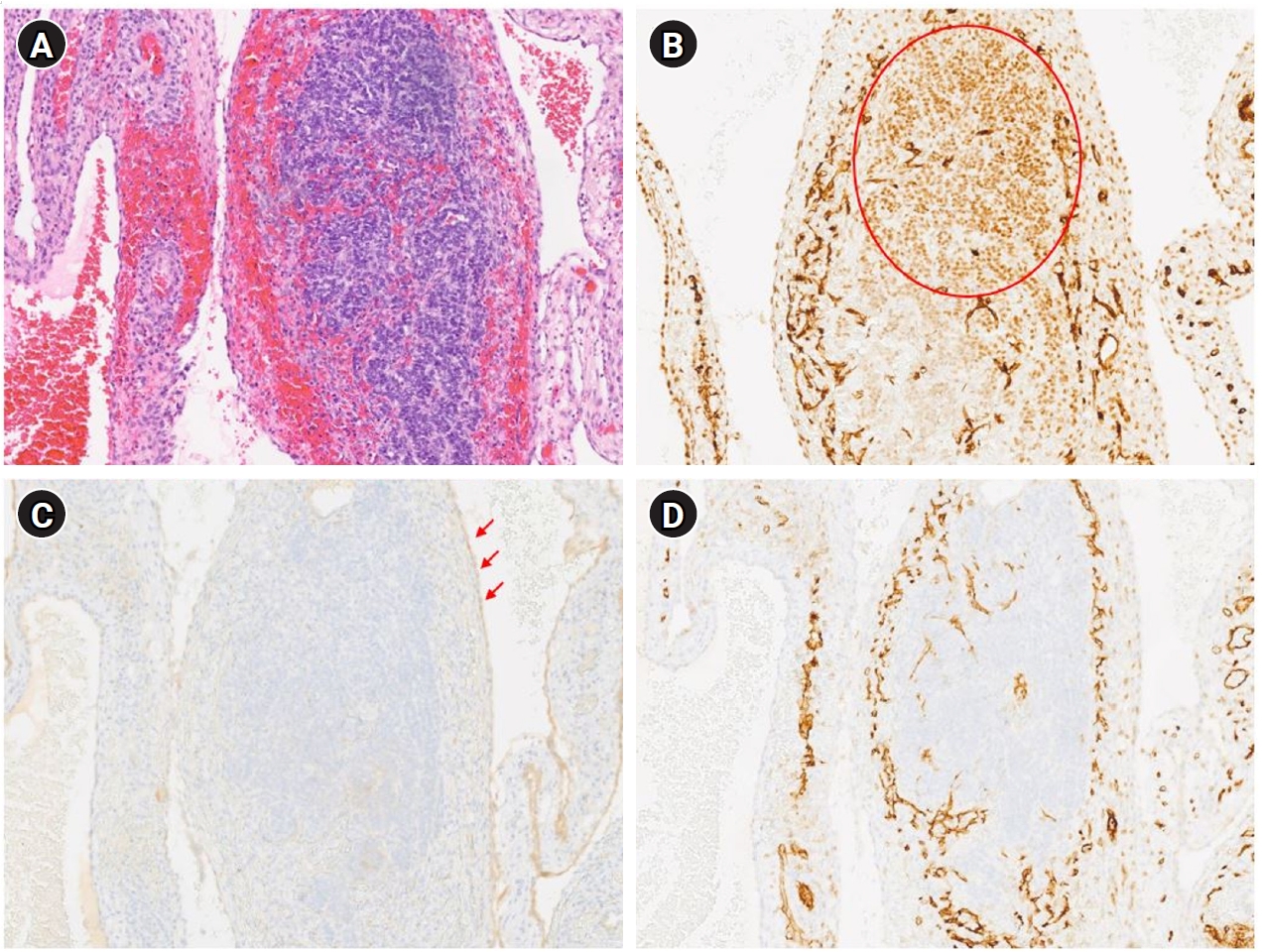
Fig. 3). Immunohistochemically, the epithelioid cells were positive for WT1 (Wilms tumor 1), supporting mesothelial origin. Calretinin showed focal weak positivity in the outer lining mesothelial cells but was negative in the mural nodules. D2-40 (podoplanin) and CD31 (cluster of differentiation 31) were negative. Overall, the immunoprofile supported the diagnosis of BCM. The patient had an uneventful postoperative course and underwent surveillance ultrasonography every 6 months. At 30 months postoperatively, she had no functional deficits and showed no evidence of recurrence.
DISCUSSION
In pediatric patients with intra-abdominal cystic lesions, the most common initial differential diagnoses include lymphatic malformation, omental or mesenteric cyst, mature cystic teratoma, peritoneal inclusion cyst, and bowel duplication cyst. Preoperatively and intraoperatively, our initial impression was that the lesion represented a lymphatic malformation because it appeared as a multiseptated cystic mass attached to the ovary without communication with other intra-abdominal structures. However, subsequent histopathological examination confirmed the diagnosis of BCM.
BCM is a rare disease that arises from mesothelial cells lining the body’s serous cavities. It predominantly affects women, with approximately 80% of cases occurring in women around 37 years of age [
1,
2]. Fewer than 200 cases have been reported in the literature [
3]. BCM is especially rare in pediatric patients, with only a few cases reported [
4]. Pediatric mesothelioma also appears to differ from adult mesothelioma, with fewer male patients, a predominance of peritoneal primary tumors, and less aggressive behavior, particularly in patients with peritoneal primary disease [
5]. Most patients remain asymptomatic until the lesion becomes large enough to compress surrounding structures. Initial symptoms include vague abdominal discomfort, tenderness, a palpable mass, and abdominal distension. Because the tumor often involves the pelvic peritoneum, it may affect structures such as the rectum, bladder, or uterus, leading to symptoms such as such as urinary disturbances, bowel obstruction, or dyspareunia in adult patients. Ultrasonography usually reveals multiloculated, anechoic cystic structures. CT shows a low-attenuation, thin-walled, multicystic mass and is useful for defining the lesion’s extent and location. Magnetic resonance imaging is considered the most informative imaging modality; cystic areas appear hyperintense on T2-weighted images, and contrast enhancement is often seen in the septa after gadolinium administration.
Diseases that should be considered in the differential diagnosis of BCM include cystic lymphatic malformation, peritoneal inclusion cyst, malignant mesothelioma, and peritoneal serous tumors. Cystic lymphatic malformation is common in children and is characterized by thin-walled, multilocular cystic masses, often arising in the mesentery. Pathologically, these lesions show cysts lined by endothelial cells, with positivity for D2-40 and CD31 and negativity for mesothelial markers. Imaging findings may be similar to those of BCM, but chylous fluid and endothelial lining can help distinguish cystic lymphatic malformation [
6]. Peritoneal inclusion cysts typically occur in adolescent females with a history of prior abdominal surgery or inflammation [
7]. Malignant lesions in the differential diagnosis include malignant mesothelioma and peritoneal serous tumors. Malignant mesothelioma is rare in children and presents with diffuse peritoneal thickening, ascites, and a mass. Pathological findings include invasive growth, cytological atypia, and increased mitotic activity; immunohistochemistry may show loss of BRCA1-associated protein 1 or methylthioadenosine phosphorylase [
8].
Histologically, BCM is composed of a monolayer of squamous or cuboidal epithelial cells. Diagnosis is supported by positive immunohistochemical staining for mesothelial markers, such as calretinin, WT1, cytokeratin 5/6, AE1/AE3, D2-40, human mesothelial cell 1, mesothelin, and thrombomodulin [
9,
10]. However, expression of these markers may vary depending on the morphological and proliferative state of the lesion. In the present case, immunohistochemistry demonstrated heterogeneous staining patterns. Although the mural nodules were negative for calretinin, the attenuated mesothelial cells lining the outer surface showed focal weak positivity. This finding suggested mesothelial origin despite the absence of diffuse calretinin expression. Previous studies have reported that the sensitivity of calretinin in mesothelial lesions is not absolute, ranging from approximately 90% to 95%, and may be reduced in certain histological contexts, including reactive or proliferative changes [
11]. Therefore, despite the lack of diffuse calretinin expression, the lesion was considered to be of mesothelial origin and was diagnosed as BCM.
Although BCM is classified as benign, it has a high propensity for local recurrence, and malignant transformation has been suspected in rare cases [
12,
13]. Given this high recurrence rate, complete surgical resection remains the mainstay of treatment. Long-term surveillance is essential, even in pediatric patients, because of the potential for recurrence. For patients with recurrence, some authors have suggested cytoreductive surgery (CRS) combined with hyperthermic intraperitoneal chemotherapy (HIPEC) as a therapeutic option [
5]. Malekzadeh et al. [
14] reported various complications in pediatric patients with peritoneal mesothelioma who underwent CRS and HIPEC with cisplatin, including pancreatitis, acute tubular necrosis, hyperbilirubinemia, bilateral pleural effusions, pneumothorax, and two cases each of anemia and coagulopathy. Although data on CRS and HIPEC for benign mesothelioma remain limited, several studies have documented their use in patients with malignant mesothelioma, with recurrence rates ranging from 42% to 57% [
5,
14-
17]. The efficacy of CRS and HIPEC in pediatric BCM appears to be limited. Given the high risk of recurrence associated with BCM, close postoperative surveillance is recommended.
This case demonstrates an unusual and potentially misleading presentation of benign multicystic peritoneal mesothelioma as an acute abdomen complicated by hemorrhage. Despite its generally indolent nature, this entity should be included in the differential diagnosis of pediatric intra-abdominal cystic masses. Because imaging alone is often insufficient for definitive diagnosis, a cautious and well-planned surgical approach is warranted, with histopathological examination serving as the diagnostic standard. Given the potential for recurrence, careful long-term follow-up is recommended.
NOTES
-
Authors’ contributions
Conceptualization: SHN. Data curation: JP, HYP, SHN. Formal analysis: JP. Methodology: JP. Visualization: HYP. Supervision: SHN. Writing–original draft: JP. Writing–review & editing: JP, SHN. All authors read and approved the final manuscript.
-
Conflict of interest
So-Hyun Nam is an editor-in-chief of this journal, but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflict of interest relevant to this article was reported.
-
Funding
None.
-
Data availability
Not applicable.
Fig. 1.Abdominal computed tomography scan showing a large, multiseptated hypodense mass in the lower abdomen.

Fig. 2.Intraoperative laparoscopic findings. (A) Large multicystic mass containing hemorrhagic contents. (B) Hemorrhagic ascites. (C) Mass attached to the right ovary. (D) Complete excision of the mass with ovarian preservation.
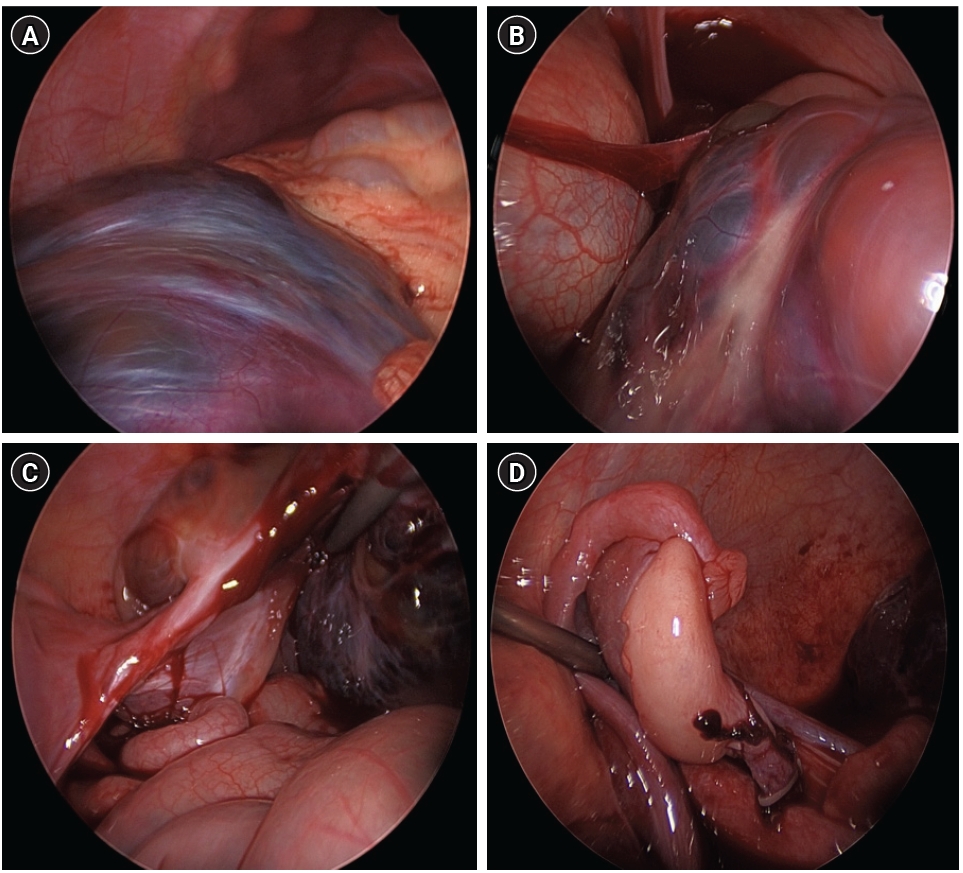
Fig. 3.Histopathological and immunohistochemical findings of the tumor. (A) H&E staining (×100) shows predominant clusters of epithelioid cells interspersed with cyst-like spaces. (B–D) Immunohistochemically (×100), the epithelioid cells show positive reactivity for WT1 (circle) (B), whereas calretinin shows focal weak positivity in the outer lining mesothelial cells (arrows) (C) but is negative in the mural nodules. (D) The cells are also negative for CD31; positive staining is observed only in the adjacent vascular endothelium.
REFERENCES
- 1. Noiret B, Renaud F, Piessen G, Eveno C. Multicystic peritoneal mesothelioma: a systematic review of the literature. Pleura Peritoneum 2019;4:20190024.
- 2. Alvir I, Bevanda B, Danolic D, et al. Benign multicystic peritoneal mesothelioma mimicking gynecologic pathology. Acta Clin Croat 2021;60:323-5.
- 3. Hassine HB, Touati M, Bouchrika A, Boughanmi F, Korbi I, Noomen F. Benign multicystic peritoneal mesothelioma (BMPM) as a rare cause of abdominal pain: a case report and review of the literature. Int J Surg Case Rep 2025;131:111448.
- 4. Hirayama Y, Higashidate N, Nakaya K, Iinuma Y. Benign cystic mesothelioma of the peritoneum arising at the greater omentum in a 14-year-old boy. Surg Case Rep 2025;11:24-0085.
- 5. Orbach D, Andre N, Brecht IB, et al. Mesothelioma in children and adolescents: the European Cooperative Study Group for Pediatric Rare Tumors (EXPeRT) contribution. Eur J Cancer 2020;140:63-70.
- 6. Li J, Luo L, Liu Y, Li W, Wei X. Mesenteric lymphangioma in childhood: a case report and narrative literature review. Front Oncol 2025;15:1541445.
- 7. Amesse LS, Gibbs P, Hardy J, Jones KR, Pfaff-Amesse T. Peritoneal inclusion cysts in adolescent females: a clinicopathological characterization of four cases. J Pediatr Adolesc Gynecol 2009;22:41-8.
- 8. Ettinger DS, Wood DE, Stevenson J, et al. Mesothelioma: peritoneal, version 2.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2023;21:961-79.
- 9. Khurram MS, Shaikh H, Khan U, et al. Benign multicystic peritoneal mesothelioma: a rare condition in an uncommon gender. Case Rep Pathol 2017;2017:9752908.
- 10. Weiss SW, Tavassoli FA. Multicystic mesothelioma: an analysis of pathologic findings and biologic behavior in 37 cases. Am J Surg Pathol 1988;12:737-46.
- 11. Ordonez NG. Value of calretinin immunostaining in diagnostic pathology: a review and update. Appl Immunohistochem Mol Morphol 2014;22:401-15.
- 12. Myers DJ, Babiker HM. Benign mesothelioma. In: StatPearls [Internet]. StatPearls Publishing; c2024 [cited 2026 Mar 27]. Available from: https://pubmed.ncbi.nlm.nih.gov/30285380/
- 13. Durell J, Dagash H, Eradi B, Nour S. Pediatric benign cystic peritoneal mesothelioma. J Pediatr Adolesc Gynecol 2016;29:e33-4.
- 14. Malekzadeh P, Good M, Hughes MS. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) with cisplatin in pediatric patients with peritoneal mesothelioma: a single institution experience and long term follow up. Int J Hyperthermia 2021;38:326-31.
- 15. Vermersch S, Arnaud A, Orbach D, et al. Multicystic and diffuse malignant peritoneal mesothelioma in children. Pediatr Blood Cancer 2020;67:e28286.
- 16. Zmora O, Hayes-Jordan A, Nissan A, et al. Cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC) for disseminated intra-abdominal malignancies in children-a single-institution experience. J Pediatr Surg 2018;53:1381-6.
- 17. Scalabre A, Philippe-Chomette P, Passot G, et al. Cytoreductive surgery and hyperthermic intraperitoneal perfusion with chemotherapy in children with peritoneal tumor spread: a French nationwide study over 14 years. Pediatr Blood Cancer 2018;65:e26934.
Citations
Citations to this article as recorded by