ABSTRACT
This review summarizes the epidemiology, diagnosis, and management of pediatric foreign body (FB) ingestion, with particular emphasis on circumstances that may require surgical involvement. Initial evaluation includes history taking, assessment of symptoms, and radiographic imaging to determine the type and location of the ingested object. Plain radiography remains the primary diagnostic modality for detecting radiopaque objects and localizing them within the gastrointestinal tract; however, additional imaging may be needed for radiolucent objects or when complications are suspected. Management depends on the anatomical location and characteristics of the FB. Esophageal FBs generally require urgent endoscopic removal, especially when button batteries, magnets, or sharp objects are involved. After an object has passed into the stomach, many cases can be managed conservatively; however, high-risk objects, including button batteries, multiple magnets, and long or sharp items, may require early removal. FBs beyond the pylorus usually pass spontaneously but require monitoring for complications. Surgical intervention may be necessary when endoscopic removal is not feasible or when complications such as obstruction, perforation, or fistula formation occur. This review outlines location- and object-specific management strategies and identifies situations in which early surgical involvement may improve outcomes in children with FB ingestion.
-
Keywords: Foreign bodies; Child; Gastrointestinal tract; Magnets; Surgery
INTRODUCTION
Foreign body (FB) ingestion is a common clinical problem in children. Mouthing and tasting environmental objects are normal developmental behaviors in early childhood, but they also increase the risk of accidental ingestion [
1]. Most ingested FBs pass spontaneously through the gastrointestinal (GI) tract without complications. However, impaction can cause mucosal injury, bleeding, obstruction, or perforation and may necessitate endoscopic or surgical intervention. The risk of complications and the choice of treatment depend on FB size, type, and location; the interval since ingestion; and the presence of symptoms.
This review summarizes the epidemiology of pediatric FB ingestion and outlines management strategies according to anatomical location and object characteristics, with particular emphasis on surgical indications. Widely adopted international guidelines and key studies are discussed in relation to surgical practice. This manuscript was prepared as a narrative review focused on the practical management of pediatric GI FB ingestion, particularly in situations requiring pediatric surgical consultation or intervention. Relevant publications from 2005 to 2025 were identified through PubMed, KoreaMed, and Google Scholar using combinations of the terms “foreign body,” “foreign body ingestion,” “children,” “pediatric,” “gastrointestinal,” “magnet,” “button battery,” and “surgery.” Publications in English and Korean were reviewed, and the reference lists of selected articles were screened to identify additional relevant studies. Priority was given to international clinical guidelines, review articles, multicenter studies, pediatric surgical case series, and representative Korean studies. The final selection was based on clinical relevance to practical management and pediatric surgical decision-making.
Written informed consent for publication of the photographs and radiographic images was obtained from the patient or the patient's legal guardian.
GENERAL CHARACTERISTICS OF INGESTED FOREIGN BODIES IN CHILDREN
FB ingestion is common in children, particularly during early childhood. The peak incidence is reported between 6 months and 3 years of age, when children explore their environment by mouthing and tasting objects [
1-
3]. According to data from the American Association of Poison Control Centers, 94,051 FB ingestions were recorded in 2019 across all age groups, including 67,186 cases in children younger than 5 years [
3]. National safety surveillance data from Korea also indicate a high burden of FB ingestion and aspiration among young children. In a recent 5-year analysis by the Korea Consumer Agency, the annual number of FB ingestion and aspiration incidents increased each year except in 2021. Among these cases, 5,411 (55.4%) occurred in children aged 1 to 3 years and 2,634 (26.8%) occurred in those aged 4 to 6 years [
4].
The risk of FB ingestion is influenced by environmental and host factors. Lack of supervision, inadequate childproofing, developmental exploration, and behavioral or developmental disorders have been identified as important risk factors [
5]. Pediatric cases are usually accidental, whereas FB ingestion in older children (>5 years) or adults is more often associated with suicidal intent, psychiatric illness, intellectual disability, or secondary gain [
3,
5].
Most pediatric FB ingestions occur unintentionally in the home during routine daily activities [
2,
3,
6]. The types and sizes of ingested objects vary widely and are influenced by regional, cultural, and socioeconomic factors [
2,
6]. Common objects include coins, toy parts, button batteries, magnets, safety pins, fishbones, and other small household items, such as screws or jewelry [
2,
3,
6,
7]. In some Asian and Mediterranean countries with high fish consumption, fishbones are particularly common ingested FBs [
2,
8]. In a Korean tertiary-center cohort of 273 pediatric FB ingestions, coins were the most common objects, followed by button batteries and sharp items; only 3.3% of cases required surgery [
9].
The clinical course of ingested FBs is benign in most cases. Approximately 80% to 90% of FBs that reach the GI tract pass spontaneously without complications, 10% to 20% require endoscopic removal, and about 1% require surgery because of obstruction, perforation, or other complications [
2,
3,
7]. Certain anatomical sites are more prone to FB impaction because of physiological narrowing or angulation, including the upper esophageal sphincter, aortic arch level, lower esophageal sphincter, pylorus, duodenal sweep, ileocecal valve, Meckel diverticulum, and anus [
2,
7]. Recognition of these common impaction sites helps clinicians predict the likely location of an FB, select appropriate imaging studies, and determine whether endoscopic or surgical intervention is required.
INITIAL APPROACH FOR DIAGNOSIS OF FOREIGN BODY INGESTION
Guidelines from the European Society for Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society of Gastrointestinal Endoscopy recommend prompt emergency department evaluation for all children with suspected FB ingestion [
10]. During the initial assessment, the physician should obtain a detailed history from the child, caregivers, or witnesses. Essential information includes the type of FB, the estimated number of objects, and the time of ingestion. In many cases, especially in children younger than 5 years, a history of possible ingestion may be the only specific finding. If respiratory distress, wheezing, or cyanosis is present, airway aspiration should be suspected rather than passage into the GI tract, and urgent airway evaluation is required [
2,
3].
Even when the FB is presumed to have entered the GI tract, associated symptoms should be assessed carefully. Fever, irritability, vomiting, abdominal pain, or poor oral intake may influence the need for urgent endoscopy or surgical consultation [
3,
7]. Underlying conditions should also be reviewed, particularly congenital or acquired GI diseases and any history of abdominal or esophageal surgery that could affect FB passage.
Regardless of the suspected FB type, plain radiography is generally recommended as the initial imaging study. Current international guidelines recommend biplane radiographs of the neck, chest, and abdomen to evaluate the esophagus and GI tract [
7,
10]. Plain radiographs help determine the shape, size, and location of radiopaque objects, such as coins, metallic fragments, and button batteries. They may also show indirect evidence of radiolucent FBs, including bowel gas patterns suggestive of ileus and free intraperitoneal air suggestive of perforation [
2,
3].
If a radiolucent FB is suspected but cannot be identified on plain radiographs, computed tomography (CT) can help detect the object and identify complications, including perforation, abscess, or obstruction [
2,
3]. Magnetic resonance imaging is not useful for localizing ingested metallic FBs and is contraindicated when button battery or magnet ingestion is suspected because of safety concerns. Ultrasound and handheld metal detectors have been investigated as adjunctive tools, but current evidence is insufficient to support their routine use [
2,
6]. Contrast esophagography or fluoroscopic studies may be considered when FB ingestion is strongly suspected but not confirmed, or when stricture is a consideration [
7,
10]. However, these examinations are often unavailable as emergency procedures in many institutions. Importantly, additional diagnostic tests should not delay necessary therapeutic interventions. When a high-risk FB is identified or serious complications are suspected, endoscopic or surgical removal should not be postponed solely to obtain further imaging [
3,
7,
10].
INITIAL MANAGEMENT ACCORDING TO FOREIGN BODY LOCATION
The anatomical location of an ingested FB remains a key determinant of urgency and therapeutic approach. In general, objects lodged in the esophagus require prompt intervention because of the risks of obstruction, mucosal injury, perforation, and aspiration. In contrast, many objects that have passed into the stomach or beyond can be managed expectantly, depending on object type, symptoms, and interval progression.
Esophagus
Esophageal FBs warrant urgent assessment because prolonged impaction increases the risk of local injury and airway compromise. Food bolus impaction is another common indication for urgent pediatric endoscopy, particularly in children with underlying esophageal disorders such as stricture or eosinophilic esophagitis. Symptomatic children with drooling, dysphagia, chest discomfort, vomiting, or respiratory symptoms require prompt removal [
2,
7]. Even in asymptomatic patients, removal within 24 hours is generally recommended for most retained esophageal objects [
6,
7]. Certain high-risk objects, particularly button batteries, sharp objects, and multiple magnets, require emergent intervention.
After an FB has reached the stomach, many blunt and small objects pass spontaneously. Management depends primarily on object type, size, and symptoms [
2,
7]. Coins and other low-risk blunt objects may be observed in asymptomatic children, whereas button batteries, magnets, long or large objects, and sharp objects often require early endoscopic retrieval [
2,
3,
7]. Persistent gastric retention or the development of symptoms should prompt reassessment.
Most FBs that progress beyond the pylorus pass spontaneously without complications [
2,
3]. Observation with caregiver education and selective follow-up imaging is appropriate in asymptomatic children when progression is expected. However, abdominal pain, vomiting, fever, GI bleeding, signs of obstruction or peritonitis, or failure to progress on serial imaging should prompt urgent reevaluation and surgical consultation [
3,
7]. A practical summary of management strategies according to anatomical location is presented in
Table 1.
APPROACH ACCORDING TO THE TYPE AND SHAPE OF FOREIGN BODY
Magnets
Among ingested FBs, magnets are particularly important from a surgical perspective because they carry a high risk of serious complications. Although safety regulations for magnetic toys have improved in some regions, small, powerful magnets remain widely available in products such as imported toys, therapeutic “magnet patches,” and magnetic jewelry. Many of these products contain exposed neodymium rare-earth magnets that are small enough to be swallowed but can generate very strong attractive forces. They are also often sold without adequate warning labels or child-safety precautions [
2,
6,
9].
A survey of members of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHAN) reported 424 pediatric cases of magnet ingestion over a 10-year period, with a marked increase in the most recent year [
7]. In preliminary data, 52% of patients were managed with endoscopic intervention alone, 20% required both endoscopy and surgery, 8% required surgery alone, and only 15% were managed with observation. Among patients who underwent surgery, 41% required repair of perforations or fistulas and 22% required bowel resection [
7].
Several Korean series have highlighted the severity of magnet-related injuries. In a single-center cohort of 273 pediatric GI FB ingestions, magnets accounted for only 4.8% of objects, but 46.2% of magnet cases developed gastric, small-bowel, or colonic perforation or deep ulceration. Most of these children required emergency surgery [
9]. Reviews of domestic surgically treated cases have reported multiple small-bowel perforations, jejuno-jejunal or jejuno-ileal fistulas, and combined gastroduodenal or gastrocolic injuries caused by chains of small rare-earth magnets [
11-
14]. Similar findings have been observed in contemporary multicenter and national series from Asia and Europe, in which approximately 20% to 40% of children with multiple-magnet ingestion ultimately required surgical intervention and a substantial subset required bowel resection or temporary stoma formation for perforation, fistula, or peritonitis [
15-
17].
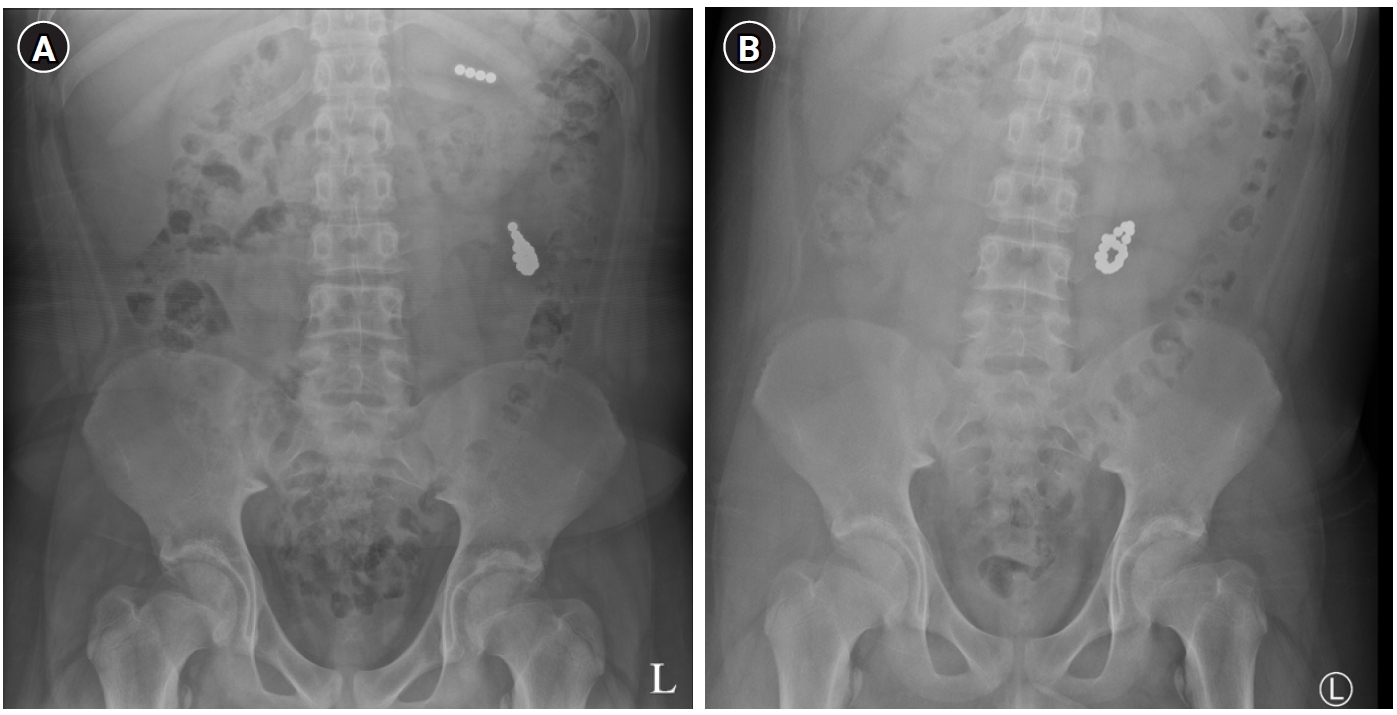
Ingestion of two or more magnets, or a magnet together with a metallic object, can be dangerous regardless of object size. Magnets located in different intestinal segments can attract across adjacent bowel loops and compress the intervening bowel wall, resulting in pressure necrosis, perforation, obstruction, fistula formation, and bleeding (
Figs. 1,
2) [
2,
3,
6]. Deaths associated with magnet ingestion have also been reported, underscoring the importance of prevention and early recognition [
14,
16].
Clinically, many children with magnet ingestion present with nonspecific symptoms, including abdominal pain, vomiting, and irritability, and the exact time of ingestion is often unknown. Plain radiographs are essential for identifying the number and location of ingested magnets. However, distinguishing a single magnet from multiple closely attached magnets can be difficult [
2,
7]. Ultrasound may help identify clustered magnets or fistulous tracts in selected cases [
11,
14], whereas CT may be limited by metallic artifacts [
2,
3].
Current international recommendations suggest that multiple magnets, or a magnet combined with another metallic object, should be removed endoscopically as soon as possible when located in the esophagus or stomach, even in asymptomatic children [
7,
10]. A single magnet in the stomach may be observed with close clinical and radiographic follow-up if the child is asymptomatic. Lack of progression or the development of symptoms should prompt removal. When multiple magnets have passed into the small bowel, the threshold for surgical consultation should be low because endoscopic access is limited and the risk of perforation or fistula is substantial. Serial radiographs should be used to monitor progression. Lack of movement over 24 to 48 hours or the development of severe abdominal pain, vomiting, fever, or peritoneal signs should prompt urgent operative management [
3,
6,
7,
16].
Magnet ingestion therefore requires a more aggressive approach than most other FB ingestions, including early endoscopic removal from the upper GI tract and prompt surgical consultation when magnets have progressed distally or complications are suspected. Recent reviews and practice guidelines consistently emphasize early surgical involvement for suspected multiple-magnet ingestion, even when endoscopic removal is initially attempted [
3,
18].
Button batteries are increasingly used in household electronic devices, and pediatric ingestion remains associated with substantial morbidity, particularly in children younger than 5 years and after ingestion of larger lithium cells [
6,
19,
20].
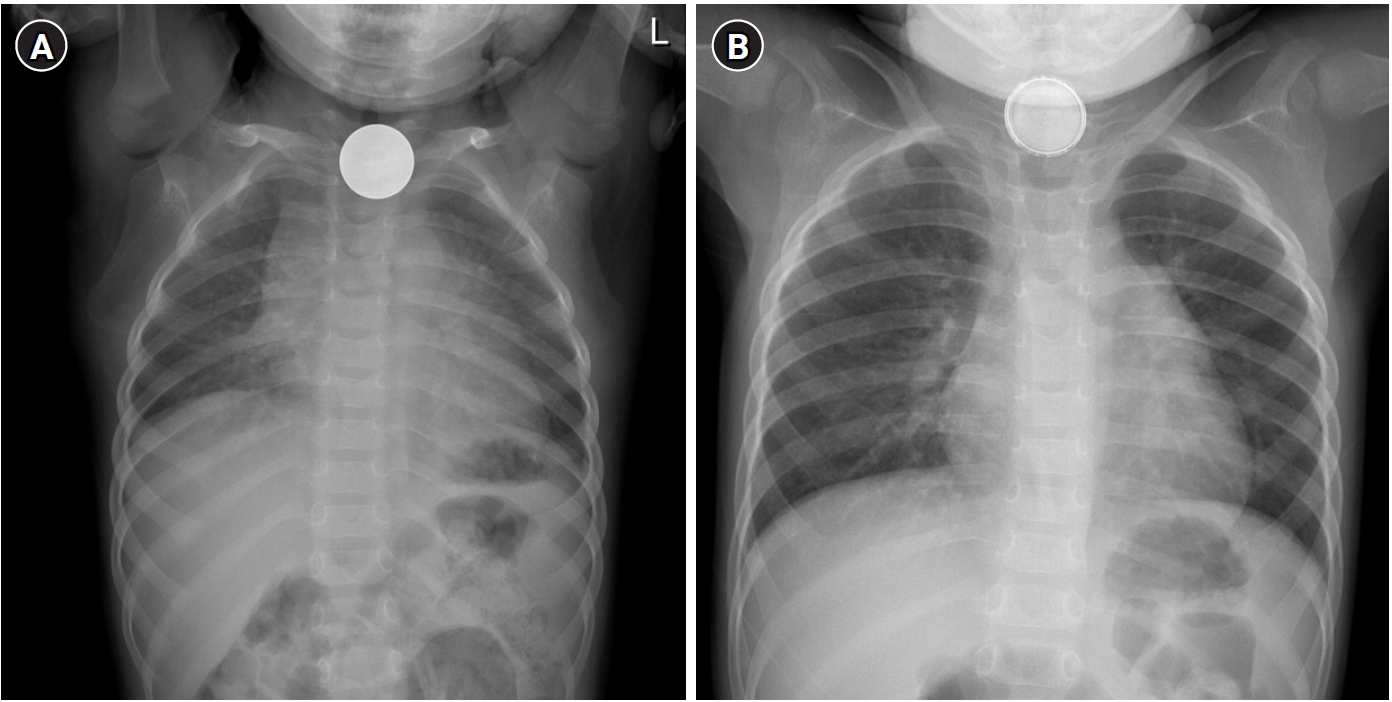
When impacted in the esophagus, button batteries can rapidly cause severe injury through local electrical current generation and alkaline tissue damage, resulting in liquefaction necrosis, perforation, fistula formation, and life-threatening hemorrhage within hours [
2,
6,
7]. Plain radiographs are important for differentiating button batteries from coins. Characteristic findings include the double-ring or halo sign on frontal views and the step-off sign on lateral views (
Fig. 3).
Esophageal button batteries require emergent endoscopic removal, ideally within 2 hours of diagnosis [
7,
10,
19]. Although earlier NASPGHAN and ESPGHAN guidelines remain important foundations, more recent expert consensus places greater emphasis on immediate removal, selected pre-endoscopic mitigation strategies such as honey or sucralfate in appropriate cases, and post-removal surveillance for delayed vascular or fistulous complications [
6,
19,
20]. Evidence supporting these adjunctive measures is based mainly on experimental studies and expert consensus rather than randomized clinical trials, and these measures should not delay urgent endoscopic intervention. Honey should not be administered to infants younger than 12 months because of the risk of infant botulism [
6,
18,
19]. After removal, careful mucosal assessment is required. Additional imaging, such as CT angiography, may be considered when deep ulceration or vascular injury is suspected [
19,
20].
For gastric button batteries in asymptomatic children, management should be individualized. Observation may be appropriate when the battery is small and progressing distally, whereas endoscopic removal should be considered for larger batteries, children younger than 5 years, prolonged gastric retention, or the development of symptoms [
7,
10,
19]. Batteries that have passed beyond the stomach may be followed clinically, but obstruction, perforation, GI bleeding, or failure to progress should prompt urgent surgical consultation.
In children, long or large FBs are less common than coins, food boluses, button batteries, or magnets, but they pose distinct management challenges because they are less likely to pass spontaneously and can cause obstruction or perforation. Typical examples include toothbrushes, chopsticks, skewers, hairpins, and certain toys or tools [
2,
3,
18].
Although definitions vary slightly across studies and guidelines, several practical size thresholds are commonly used because they reflect the likelihood of passage through physiological narrowings of the GI tract. In children younger than 5 years, objects wider than approximately 2.0 to 2.5 cm are less likely to pass the pylorus, whereas objects longer than 5 to 6 cm may fail to negotiate the duodenal sweep or ileocecal valve. In children aged 5 years or older, slightly larger objects may pass spontaneously, but objects longer than 6 to 10 cm or wider than 2.5 cm remain concerning for retention [
2,
3,
7].
Accordingly, international guidelines generally recommend endoscopic retrieval rather than expectant management for long or large FBs identified in the stomach or proximal duodenum, particularly in smaller children [
7,
10]. Retrospective series confirm that most such objects require endoscopic removal, although only a small proportion ultimately require surgery [
18,
21].
If a long or large FB has already entered the small bowel, but the child is asymptomatic and radiographs show steady distal movement, careful observation with serial imaging may be appropriate. However, if serial radiographs show no progression, or if vomiting, abdominal pain, or signs of obstruction develop, early surgical consultation is indicated. Persistent impaction in the small bowel or ileocecal region despite expectant management may ultimately require operative removal, often through limited enterotomy or segmental resection, depending on bowel viability.
Superabsorbent polymers (water beads)
Superabsorbent polymer balls, also known as water beads, are used for hydroponic plant cultivation, decorative purposes, fragrance products, and sensory play. In their dry state, water beads are small (often 2–3 mm in diameter) and visually resemble candy, making them attractive to young children. When exposed to water, they can expand to more than 30 to 60 times their original volume and become much larger and slippery [
6,
7,
22]. Experimental data and recent reviews suggest that some products may expand to more than 100 to 150 times their dry size, particularly in low-osmolar solutions [
3,
6].
Because of their marked swelling capacity, ingested water beads may fail to pass spontaneously and can cause small bowel obstruction. Diagnosis is challenging because water beads are usually radiolucent and may not be visible on plain radiographs; even on CT, they can be difficult to distinguish from surrounding bowel contents in some cases [
6,
18,
22]. Children often present with nonspecific symptoms, including vomiting, abdominal distension, and reduced oral intake, and the ingestion history may not be apparent. In some reports, water bead obstruction has been associated with electrolyte disturbances or neurological symptoms, such as acute hyponatremia with seizure, further complicating the clinical picture. The mechanism is uncertain and may involve severe electrolyte disturbance secondary to obstruction or possible direct acrylamide-related neurotoxicity in selected products [
22,
23].
When small bowel obstruction caused by water beads is suspected, surgical exploration is frequently required. At laparotomy or laparoscopy, the beads may be found impacted in the distal small bowel or ileocecal region. Management options include enterotomy with bead removal or manual fragmentation and milking of the beads toward the colon to facilitate passage. The choice depends on the degree of obstruction, bowel viability, and the surgeon’s judgment [
3,
22]. Although some asymptomatic children who ingest very small beads can be managed conservatively, those with established obstruction almost always require operative intervention [
3,
18].
Given the diagnostic difficulty and potential for severe obstruction or death, prevention through caregiver education and regulation of high-risk products is essential. Recent regulatory efforts in North America and Europe have proposed limiting the expansion capacity and size of water beads marketed for children and, in some jurisdictions, restricting or banning their sale altogether [
6,
18].
The types of sharp or pointed FBs ingested by children vary over time and by region. In earlier decades in Western countries, safety pins used for cloth diapers were common sharp FBs, but their frequency has declined with the widespread adoption of disposable diapers [
7]. Common examples include needles, pins, nails, screws, fishbones, and fragments of glass or plastic [
2,
3,
6]. In Asian and Mediterranean regions where fish consumption is high, fishbones are particularly frequent sharp FBs [
2,
8,
21]. Many sharp objects are radiopaque and readily visible on plain radiographs; however, some plastic or wooden objects may be radiolucent and require additional imaging for detection.
Sharp objects pose a higher risk of mucosal injury, bleeding, and perforation than blunt objects. Historically, management has been influenced by Jackson’s axiom that advancing points puncture whereas trailing points do not. Sharp objects with the pointed end leading are more likely to cause perforation [
5,
24]. Clinical studies and case series have documented complications such as esophageal or gastric perforation, small bowel obstruction, intra-abdominal abscess, and fistula formation after sharp-object ingestion [
3,
19,
25]. In Korean pediatric series, fishbones and glass fragments were associated with a relatively high rate of endoscopic removal, whereas neglected sharp objects occasionally led to mediastinitis or intra-abdominal sepsis [
8,
9].
Guidelines recommend urgent endoscopic removal of sharp objects lodged in the esophagus or stomach, even in asymptomatic patients, because of the high risk of perforation and migration [
7,
10,
19]. In the esophagus, sharp objects are usually removed emergently to prevent catastrophic complications. In the stomach and proximal duodenum, prompt endoscopic retrieval is also advised when feasible, particularly if the object is long or has multiple sharp edges [
3,
6,
7].
Once a sharp object has passed beyond the ligament of Treitz, management remains a topic of debate. Some guidelines suggest that small, smooth, sharp objects may be observed with serial radiographs if the child is asymptomatic and the object is progressing distally [
7,
19]. However, signs of obstruction, localized peritonitis, or lack of progression on imaging should prompt early surgical consultation. Surgical options range from limited enterotomy for object removal to segmental bowel resection in cases of perforation, necrosis, or abscess formation [
3,
25].
Overall, sharp-object ingestion in children requires a lower threshold for endoscopic and surgical intervention than many other FB ingestions. Management should be individualized according to object characteristics, location, and the child’s clinical status.
Coins
Coin ingestion is one of the most common causes of FB ingestion in children, particularly in countries where coins are widely used [
2,
7,
21,
26]. Large cohort studies and national surveillance data consistently show that coins account for a substantial proportion of pediatric FB ingestions presenting to emergency departments and endoscopy units, often among children younger than 5 years [
9,
21]. More than 80% of ingested coins in children pass spontaneously without significant complications, especially when the coin has already reached the stomach and the child is asymptomatic [
2,
3,
18]. However, certain coin sizes and age groups are associated with a higher risk of esophageal impaction or failure to pass.
In children younger than 5 years, coins with a diameter ≥23 mm are more likely to become lodged in the esophagus or fail to progress, which can lead to esophageal ulceration or stricture if removal is delayed [
2,
7,
19]. Current guidelines recommend urgent endoscopic removal of esophageal coins, particularly in symptomatic children, and removal within 24 hours even in asymptomatic cases [
7,
10]. Gastric coins in asymptomatic children may be observed with serial radiographs, and elective removal can be considered if the coin remains in the stomach or if symptoms develop [
3,
18].
In Korea, coins of four main denominations are in circulation, with approximate diameters of 18.0 mm (new 10-won), 21.6 mm (50-won), 24.0 mm (100-won), and 26.5 mm (500-won) [
27]. From a practical standpoint, coins ≥23 mm in diameter, including old 10-won coins, 100-won coins, and 500-won coins, are unlikely to pass the esophagus spontaneously in children younger than 5 years. Therefore, endoscopic removal is generally recommended in this age group when such coins are impacted rather than relying on spontaneous passage [
9]. Clinicians should also remain vigilant for radiographic misinterpretation of button batteries as coins and should carefully evaluate distinguishing signs before selecting a management strategy [
3,
19]. For ease of clinical application, a risk-oriented summary based on object characteristics is provided in
Table 2.
SURGICAL MANAGEMENT FOR PEDIATRIC FOREIGN BODY INGESTION
Absolute indications for surgery in pediatric FB ingestion have not been clearly defined, and management decisions are often individualized according to FB type and location, clinical symptoms, and available endoscopic expertise. As summarized in
Tables 1 and
2, surgical consultation should be considered when spontaneous passage is unlikely or has failed, when endoscopic removal is unsuccessful or infeasible because the FB is beyond the reach of the endoscope, or when evidence of bowel perforation or obstruction makes nonoperative management inappropriate [
2,
3,
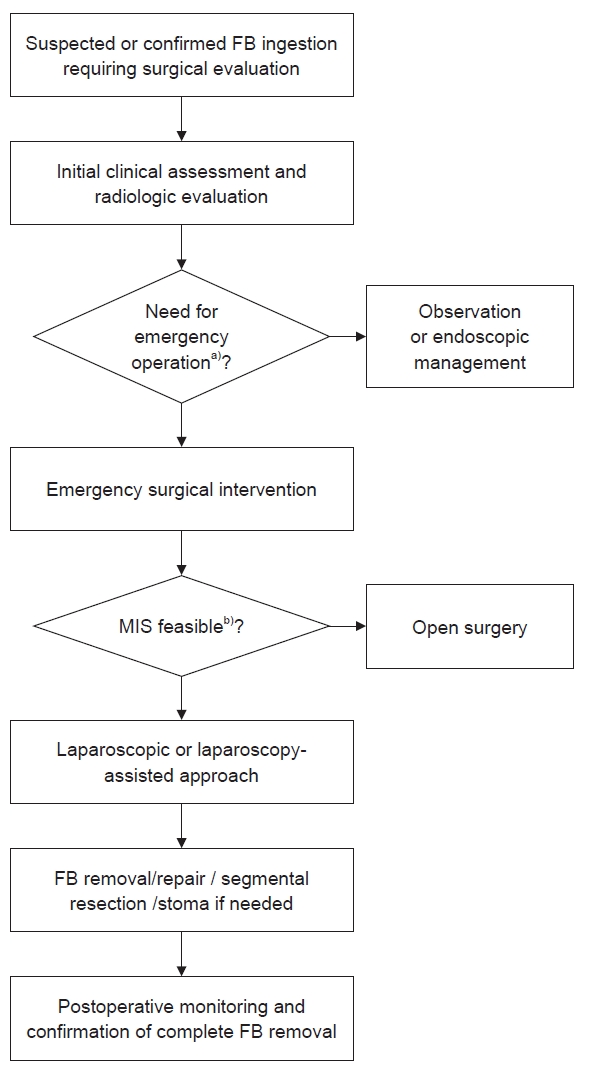
7]. Emergency operation is generally reserved for children with generalized peritonitis, complete mechanical obstruction, hemodynamic instability, or radiological and clinical evidence of bowel perforation or necrosis. In other situations, close inpatient observation with serial examinations and imaging may allow urgent but nonemergent operative planning. In centers where pediatric endoscopy is not readily available, early involvement of pediatric surgeons or transfer to an appropriate referral center should be considered.
No surgical procedure is specific to FB ingestion, and standard GI surgical principles are generally applied. In most cases, two basic approaches are used. The first is gastrotomy or enterotomy at the site of impaction, FB removal, and primary closure of the enterotomy. The second is segmental resection of the affected bowel segment followed by primary anastomosis. The choice between these approaches depends on the location of the FB, the presence and extent of perforation or ischemia, and the patient’s overall condition. Minimally invasive approaches, including laparoscopy or laparoscopy-assisted extracorporeal bowel repair through a small incision, are feasible in selected stable patients and may reduce wound burden, postoperative pain, and recovery time while allowing complete abdominal exploration. Open surgery remains appropriate in patients with diffuse peritonitis, marked bowel distension, hemodynamic instability, or anticipated complex reconstruction.
In cases of multiple-magnet ingestion, magnets may adhere across adjacent bowel loops and form entero-enteric fistulas, leading to perforation, obstruction, or necrosis [
2,
6,
12,
13]. In some situations, the magnets can be removed through the fistula tract itself without creating an additional enterotomy, after which the fistula can then be repaired, or the affected bowel segment can be resected, depending on bowel viability. Sharp objects may require localized repair or limited bowel resection when perforation is identified. Button batteries located beyond endoscopic reach may require operative removal when progression fails or when delayed perforation or fistula formation is suspected. Large bezoars or impacted intraluminal FBs may occasionally require gastrotomy or enterotomy when endoscopic treatment is unsuccessful. Anecdotal techniques, such as transappendiceal extraction of a small FB impacted near the ileocecal valve, have also been described in selected cases [
12], but these are not established standard approaches and should be individualized according to intraoperative findings.
When perforation or obstruction has been present for a prolonged period, the affected bowel may be edematous or ischemic, and multiple perforations may be present. In such cases, segmental resection may be preferable to primary repair. The decision to perform primary anastomosis or temporary stoma formation should follow the same principles used in other emergency GI operations, taking into account hemodynamic stability, the degree of contamination, and the quality of the bowel ends.
Perioperative management generally follows standard protocols for emergency abdominal surgery in children, including appropriate fluid resuscitation, broad-spectrum antibiotics, and careful monitoring for signs of anastomotic failure or ongoing sepsis. Reported postoperative complications include wound infection, ileus, intra-abdominal abscess, anastomotic leak after bowel resection, and the need for reoperation in selected cases, particularly after delayed diagnosis or severe bowel injury [
16,
21]. At the end of the procedure, surgeons should verify that the number and type of removed FBs correspond to those identified on imaging and in the clinical history. Whenever possible, retrieved objects should be documented with photographs or operative notes to facilitate communication with caregivers and consulting services. This documentation may also be useful for medicolegal and preventive purposes. A practical framework for pediatric surgical involvement is summarized in
Fig. 4.
CONCLUSION
Management of pediatric FB ingestion should be tailored to the object’s location and type and to the child’s clinical condition. Most ingested FBs pass spontaneously without complications. However, esophageal button batteries, multiple magnets, long or large objects, and other high-risk FBs require prompt, decisive intervention. FBs that remain in the GI tract for more than approximately 1 week should be followed with radiography to confirm progression or removal.
Although most cases resolve without serious consequences, FB ingestion can occasionally result in severe, life-threatening complications. Continued public education, careful supervision of young children, and improved regulation and design of high-risk consumer products remain important preventive measures. Timely recognition of children who require pediatric surgical consultation is essential to prevent major morbidity.
NOTES
-
Authors’ contributions
Conceptualization: SHK. Data curation: AK. Supervision: SHK. Investigation: AK. Visualization: AK. Writing–original draft: AK. Writing–review & editing: SHK. All authors read and approved the final manuscript.
-
Conflict of interest
None.
-
Funding
None.
-
Data availability
Not applicable.
Fig. 1.Plain radiographs of a 16-year-old boy who swallowed multiple magnets. (A) On the day of admission, magnets were located in two different areas. (B) Two days later, the magnets had become attached. Because no interval movement was observed on subsequent radiographs, emergency surgery was performed.
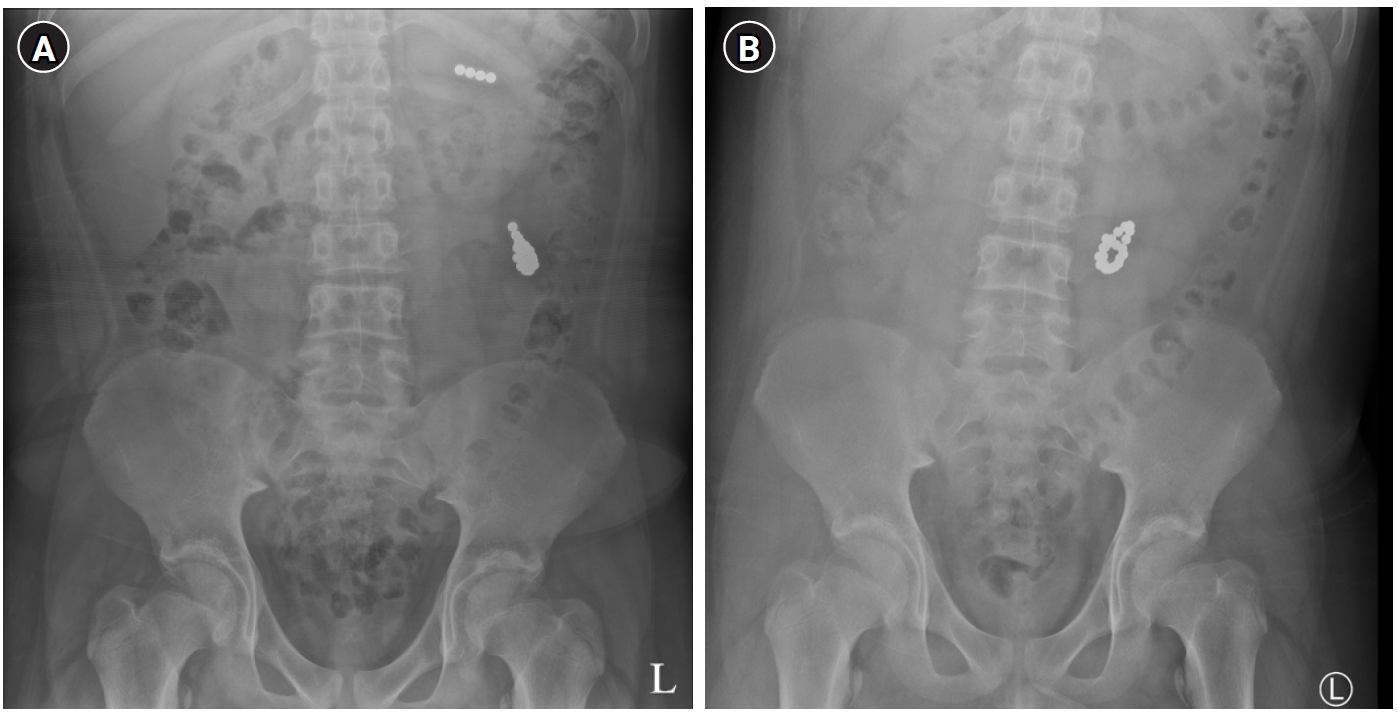
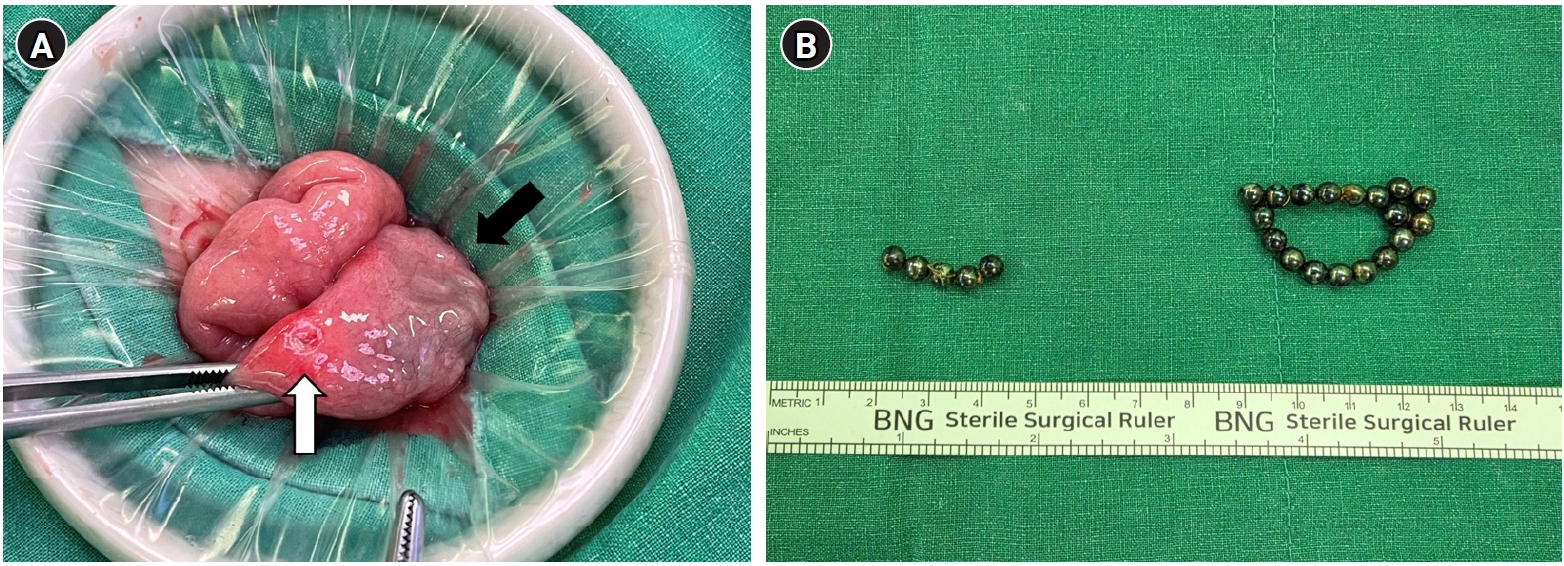
Fig. 2.Intraoperative findings in a 16-year-old boy with multiple-magnet ingestion. (A) After mini-laparotomy, the adherent jejunum and ileum were exteriorized. Magnets were found in the ileum (black arrow), with ulceration also visible (white arrow). (B) The magnets were removed through the ulcer-induced perforation.
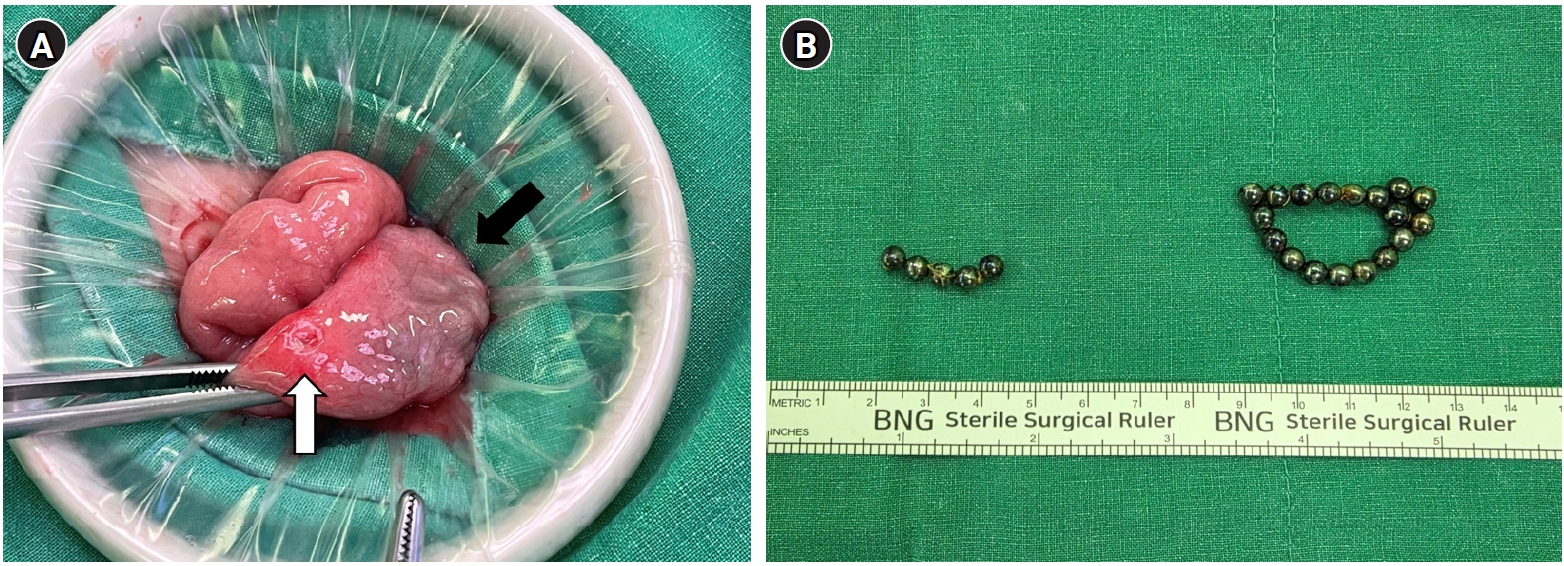
Fig. 3.Comparison of plain radiographs in children with coin and button battery ingestion. (A) Coin in the esophagus. (B) Button battery in the esophagus showing the “double-ring sign,” which differentiates it from a coin.
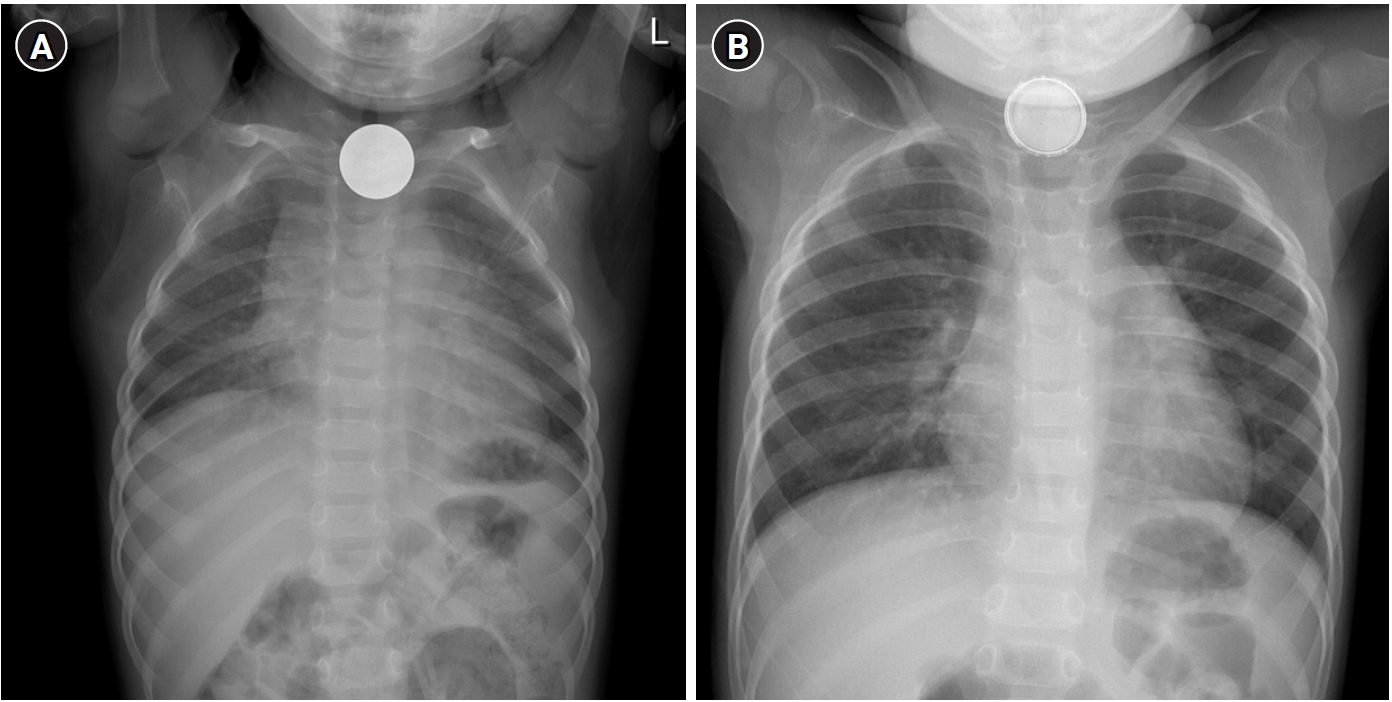
Fig. 4.Practical surgical decision-making algorithm for pediatric gastrointestinal FB ingestion. MIS, minimally invasive surgery; FB, foreign body. a)Emergency indications: peritonitis, perforation, complete obstruction, hemodynamic instability, or suspected bowel necrosis. b)Consider in stable patients with localized pathology and limited contamination.
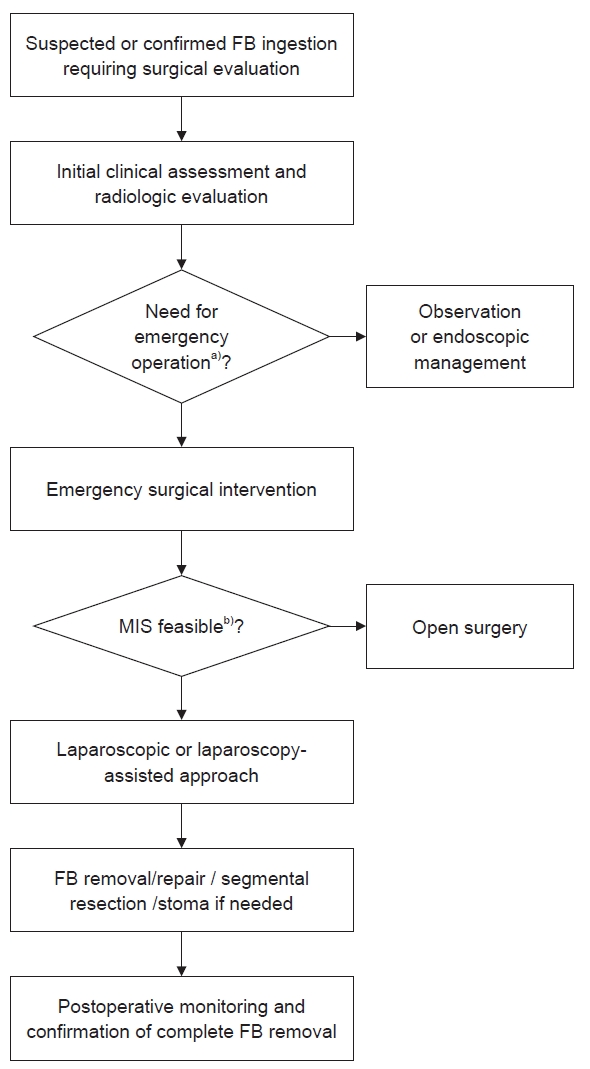
Table 1.Location-based practical summary of recommended management strategies for pediatric foreign body ingestion
Table 1.
|
Location |
Emergent removal (within 2 hr) |
Urgent removal (within 24 hr) |
Observation acceptable |
When to involve pediatric surgery |
|
Esophagus |
• Button battery (<2 hr) |
• Blunt object (e.g., coin) if asymptomatic |
• Rare |
• Failed endoscopic removal |
|
• Sharp or pointed object |
• Magnets |
• Evidence of perforation |
|
• Airway compromise/secretion intolerance |
|
• Suspected vascular injury |
|
Stomach |
- |
• Symptomatic button battery |
• Small blunt object (e.g., coin) if asymptomatic |
• Failed endoscopic removal |
|
• ≥20 mm battery in children <5 yr (if retained 24–48 hr) |
• Asymptomatic single magnet with close follow-up |
• Signs of obstruction or peritonitis |
|
• Multiple magnets |
|
|
|
• Sharp or pointed object |
|
|
|
• Long or large object |
|
|
|
Small bowel (distal to pylorus) |
- |
• High-risk object with symptoms |
• Most blunt objects |
• Lack of progression on serial imaging (e.g., 24–48 hr for magnets) |
|
• Asymptomatic single magnet with serial radiographs |
• Persistent non-progression over several days (sharp objects) |
|
• Small bowel obstruction or peritoneal signs |
|
Colon |
- |
- |
• Most objects |
• Rare, symptomatic cases only |
Table 2.Object-based risk-oriented practical summary for surgical decision-making in pediatric foreign body ingestion
Table 2.
|
Object type |
Key pathophysiologic risk |
Core timing principle |
When to involve pediatric surgery |
|
Button battery |
• Rapid alkaline necrosis, fistula formation, vascular erosion |
• Esophagus → remove within 2 hr |
• Deep ulceration or necrosis after removal |
|
• Stomach → remove if symptomatic or ≥20 mm in children <5 yr |
• Suspected tracheoesophageal or aorto-esophageal fistula |
|
• Distal battery with symptoms |
|
Multiple magnets |
• Pressure necrosis, entero-enteric fistula, perforation |
• Early removal if reachable in upper gastrointestinal tract |
• Beyond stomach with no progression on serial imaging (24–48 hr) |
|
• Abdominal pain, fever, obstruction |
|
Single magnet |
• Usually benign unless combined with metallic object |
• Observation with serial radiographs if asymptomatic |
• Combined with metallic object |
|
• Development of symptoms or lack of progression |
|
Sharp or pointed object |
• Increased risk of perforation |
• Remove within 24 hr if reachable |
• No progression on serial imaging |
|
• Clinical signs of perforation |
|
Long or large object |
• Pyloric or ileocecal impaction |
• Remove if located in stomach |
• Failure to progress |
|
• Obstruction or peritonitis |
|
Coins (blunt object) |
• Usually benign |
• Remove from esophagus within 24 hr |
• Rare, symptomatic cases |
|
• Observe in stomach |
|
Superabsorbent polymers (water beads) |
• Expansion → small bowel obstruction |
• Remove if reachable in upper gastrointestinal tract |
• Small bowel obstruction |
|
• Radiolucent obstruction requiring exploration |
REFERENCES
- 1. McMahon K, Conners GP, Mohseni M. Pediatric foreign body ingestion. In: StatPearls [Internet]. StatPearls Publishing; c2025 [cited 2025 Sep 9]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430915/
- 2. Lee JH. Foreign body ingestion in children. Clin Endosc 2018;51:129-36.
- 3. Demiroren K. Management of gastrointestinal foreign bodies with brief review of the guidelines. Pediatr Gastroenterol Hepatol Nutr 2023;26:1-14.
- 4. Korea Consumer Agency. Analysis of child safety accident trends in 2023 [Internet]. Korea Consumer Agency; c2024 [cited 2025 Sep 29]. Available from: https://www.isafe.go.kr/children/selectBbsNttView.do?bbsNo=101&nttNo=48569&key=506
- 5. Telford JJ. Management of ingested foreign bodies. Can J Gastroenterol 2005;19:599-601.
- 6. Manfredi MA, Alvarez RP, Arai K, et al. Global insights on the diagnosis, management, and prevention of pediatric ingestions: a report from the FISPGHAN expert panel. JPGN Rep 2025;6:274-87.
- 7. Kramer RE, Lerner DG, Lin T, et al. Management of ingested foreign bodies in children: a clinical report of the NASPGHAN Endoscopy Committee. J Pediatr Gastroenterol Nutr 2015;60:562-74.
- 8. Lim CW, Park MH, Do HJ, et al. Factors associated with removal of impacted fishbone in children, suspected ingestion. Pediatr Gastroenterol Hepatol Nutr 2016;19:168-74.
- 9. Choi E, Lee HG, Choi SJ, Chung SY. Clinical analysis of foreign bodies in gastrointestinal tract in children. J Korean Assoc Pediatr Surg 2014;20:12-6.
- 10. Thomson M, Tringali A, Dumonceau JM, et al. Paediatric gastrointestinal endoscopy: European Society for Paediatric Gastroenterology Hepatology and Nutrition and European Society of Gastrointestinal Endoscopy guidelines. J Pediatr Gastroenterol Nutr 2017;64:133-53.
- 11. Jeon J, Lee K, Ahn SM, et al. A case of small bowel fistulas caused by multiple magnet ingestion: usefulness of ultrasonography. J Korean Soc Ultrasound Med 2013;32:294-7.
- 12. Kim SH. Gastrointestinal complications caused by ingestion of magnets in children. J Pusan Natl Univ Hosp 2016;39:229-38.
- 13. Nam SH. Underestimated risks of rare-earth magnet ingestion in children: when does it need surgery? Pediatr Emerg Med J 2016;3:43-7.
- 14. Song GJ, Yun JH, Jung HI, et al. Gastrointestinal perforation caused by neodymium magnet toys: a dangerous foreign body with super-strength. Adv Pediatr Surg 2020;26:83-7.
- 15. Wang K, Zhang D, Li X, et al. Multicenter investigation of pediatric gastrointestinal tract magnets ingestion in China. BMC Pediatr 2020;20:95.
- 16. Kwon HJ, Park J. Surgical removal of ingested magnets in children: a retrospective clinical analysis of 16 patients and review of the literature. Medicine (Baltimore) 2025;104:e42903.
- 17. Neville JJ, Lyttle MD, Messahel S, et al. Magnet ingestion in children in the United Kingdom: a national prospective observational surveillance study. Arch Dis Child 2025;110:778-85.
- 18. Sims JK, Li R, Lovvorn HN. Digestive foreign bodies in children: old problems, new complexities. Adv Surg 2025;59:325-39.
- 19. Oliva S, Romano C, De Angelis P, et al. Foreign body and caustic ingestions in children: a clinical practice guideline. Dig Liver Dis 2020;52:1266-81.
- 20. Eyring JB, Hemeyer BM, Walker S, et al. Button battery ingestion: exploring socioeconomic risk factors. Otolaryngol Head Neck Surg 2025;173:96-105.
- 21. Di Siena A, Melli P, Rodofile F, et al. Foreign body ingestion in children: a 16-year experience. Pediatr Gastroenterol Hepatol Nutr 2025;28:215-23.
- 22. Lee NR, Shin HB, Jeong YJ, Kim SJ. Small bowel obstruction by water beads in a 12-month-old girl presenting with acute hyponatremia with seizure. Pediatr Emerg Med J 2019;6:86-91.
- 23. Haugen A, Friedman E, Duff I. Intestinal obstruction and neurotoxicity associated with water bead ingestion. Pediatrics 2025;155:e2023065575.
- 24. Jackson CL. Foreign bodies in the esophagus. Am J Surg 1957;93:308-12.
- 25. Goh BK, Chow PK, Quah HM, et al. Perforation of the gastrointestinal tract secondary to ingestion of foreign bodies. World J Surg 2006;30:372-7.
- 26. Hong SJ, Kim C, Lee DW, et al. Foreign body ingestion trends in children in the Daegu-Kyungpook Province, Korea before and during the COVID-19 period: a repeated cross-sectional study. Transl Pediatr 2023;12:1364-72.
- 27. Bank of Korea. History of Korean coins [Internet]. Bank of Korea; c2025 [cited 2025 Dec 7]. Available from: https://www.bok.or.kr/portal/main/contents.do?menuNo=200369