ABSTRACT
-
Purpose
Enteric duplication cysts (EDCs) are rare congenital anomalies of the gastrointestinal tract. This study aimed to delineate the clinical, anatomical, and pathological spectrum of EDCs based on a 40-year single-center experience.
-
Methods
A retrospective review was conducted of 45 pediatric patients who underwent surgical treatment for EDCs at a single institution between 1985 and 2023. Clinical records, imaging studies, and pathological reports were analyzed.
-
Results
The study included 28 males and 17 females, with a median age at surgery of 4.7 months. Most patients (75.6%) underwent surgery before 2 years of age. The ileum was the most common location (57.8%), followed by the jejunum (11.1%) and ileocecal valve (11.1%). Vomiting (46.7%) was the most common presenting symptom. Emergency surgery was required in 28.9% of cases because of complications such as volvulus or intussusception. Preoperative imaging using ultrasonography (US) and/or computed tomography resulted in a correct diagnosis in 34 of 45 patients (75.6%), with EDCs correctly identified in 30 patients (66.7%), frequently based on the characteristic “double wall sign” observed on US. Histopathological examination identified heterotopic gastric mucosa in 61.4% of evaluable cases. Postoperative outcomes were generally favorable, with a median hospital stay of 7.5 days.
-
Conclusion
EDCs are rare congenital anomalies that are primarily diagnosed during early childhood. The ileum is the most frequent site of involvement, and clinical presentation is often related to acute complications. Prompt and complete surgical excision remains the definitive treatment and leads to favorable short-term postoperative outcomes, with no recurrence observed during the available follow-up period.
-
Keywords: Cysts; Gastrointestinal tract; Children; Gastric mucosa; Ultrasound
INTRODUCTION
Enteric duplication cysts (EDCs), also referred to as alimentary tract duplications, are rare congenital anomalies of the gastrointestinal (GI) tract. These lesions can occur anywhere from the tongue to the anus but are most commonly located in the small intestine [
1,
2]. The reported incidence of EDCs ranges from 1 in 4,500 to 1 in 18,000 live births, making them an important, although uncommon, condition in pediatric surgery [
3,
4]. The term “alimentary tract duplication” was formally established by Ladd [
5] in 1937 to unify a variety of previously described malformations.
Pathologically, enteric duplications must satisfy three essential criteria proposed by Gross et al. [
6] in the 1950s: the presence of a well-developed smooth muscle coat, an epithelial lining representing a portion of GI mucosa, and a close anatomical association with the adjacent alimentary tract, often with a shared blood supply. EDCs most commonly present as noncommunicating spherical cystic lesions, although tubular forms that communicate with the adjacent bowel lumen have also been described [
2].
EDCs predominantly affect infants and young children, with approximately 80% of cases diagnosed before 2 years of age [
7]. Clinical presentation is highly variable and nonspecific and depends largely on lesion size, anatomical location, and the presence of ectopic tissue within the cyst [
1]. Common manifestations include vomiting, abdominal distension, and a palpable abdominal mass, typically reflecting mass effect or partial bowel obstruction. However, many patients present acutely with surgical emergencies such as intestinal obstruction, intussusception, or volvulus [
4,
8].
Because of the rarity of EDCs, most published literature consists of case reports or small case series. Large, long-term single-center studies provide valuable information regarding the natural history, evolving diagnostic approaches, and contemporary surgical management of these lesions, including minimally invasive techniques [
9].
In this study, we retrospectively analyzed 45 pediatric patients with EDCs treated at a single institution over a 40-year period. Through this large institutional experience, we sought to characterize the clinical, anatomical, and pathological spectrum of EDCs and provide comprehensive data to support the optimal management of this rare and challenging congenital anomaly.
METHODS
Ethics statement
This study was approved by the Institutional Review Board of Keimyung University Dongsan Hospital, and the requirement for informed consent was waived because of the retrospective study design (No. 2025-12-078).
Study design and patient population
This retrospective study reviewed pediatric patients diagnosed with EDCs who underwent surgical treatment between June 1985 and June 2023. Surgically treated enteric duplications arising along the GI tract were included in the analysis. Anal canal duplications were excluded because they are considered distinct perineal duplication anomalies rather than true alimentary tract duplications. A total of 45 patients met the inclusion criteria and were included in the study.
Data collection
Clinical records were reviewed for demographic characteristics, age at presentation and surgery, presenting symptoms, and prenatal detection history. Diagnostic evaluation included plain abdominal radiography, ultrasonography (US), and computed tomography (CT), and the corresponding preoperative radiological impressions were recorded. Operative notes were reviewed to identify intraoperative findings, including lesion location, lesion size, and operative time. Postoperative outcomes and complications were also assessed. Emergency surgery was defined as surgery performed for acute complications, including bowel obstruction, volvulus, intussusception, or perforation.
Imaging evaluation
Imaging studies were reviewed to evaluate the diagnostic work-up. US and CT were used selectively according to the clinical presentation; some patients underwent only US, others underwent only CT, and some received both examinations. Imaging findings and preoperative radiological impressions were compared with the intraoperative diagnosis.
Pathological analysis
All resected specimens were examined by experienced pathologists. The epithelial lining of each duplication cyst was evaluated, including the presence of heterotopic mucosa and other epithelial variants described in the pathology reports.
Outcomes
The primary outcomes were clinical presentation, anatomical distribution, operative indications, surgical management, and pathological characteristics of enteric duplications. Secondary outcomes included postoperative complications and short-term postoperative results. Long-term follow-up data were unavailable for most patients.
RESULTS
Demographics and clinical presentation
A total of 45 children underwent surgical treatment for EDCs, including 28 males and 17 females. The median age at surgery was 4.7 months (range, 2 days–127.2 months), and 34 patients (75.6%) underwent surgery before 2 years of age (
Table 1). Prenatal US identified duplication cysts in eight patients. Of these, four underwent elective surgery before 1 year of age according to institutional protocols for complication prevention. Surgery was delayed until 1 year of age in one patient at the parents’ request. Two patients were diagnosed incidentally during evaluations for enteritis, and subsequent history-taking revealed a previously reported prenatal diagnosis that had not been followed up. The remaining patient became symptomatic before the planned elective intervention. The surgical approach, including minimally invasive surgery, was determined primarily by surgeon preference. With advances in surgical techniques, laparoscopic approaches became more common after 2009 and were used in the majority of recent cases. The most common presenting symptom was vomiting (46.7%), followed by abdominal pain (26.7%) and abdominal distension; GI bleeding was rare.
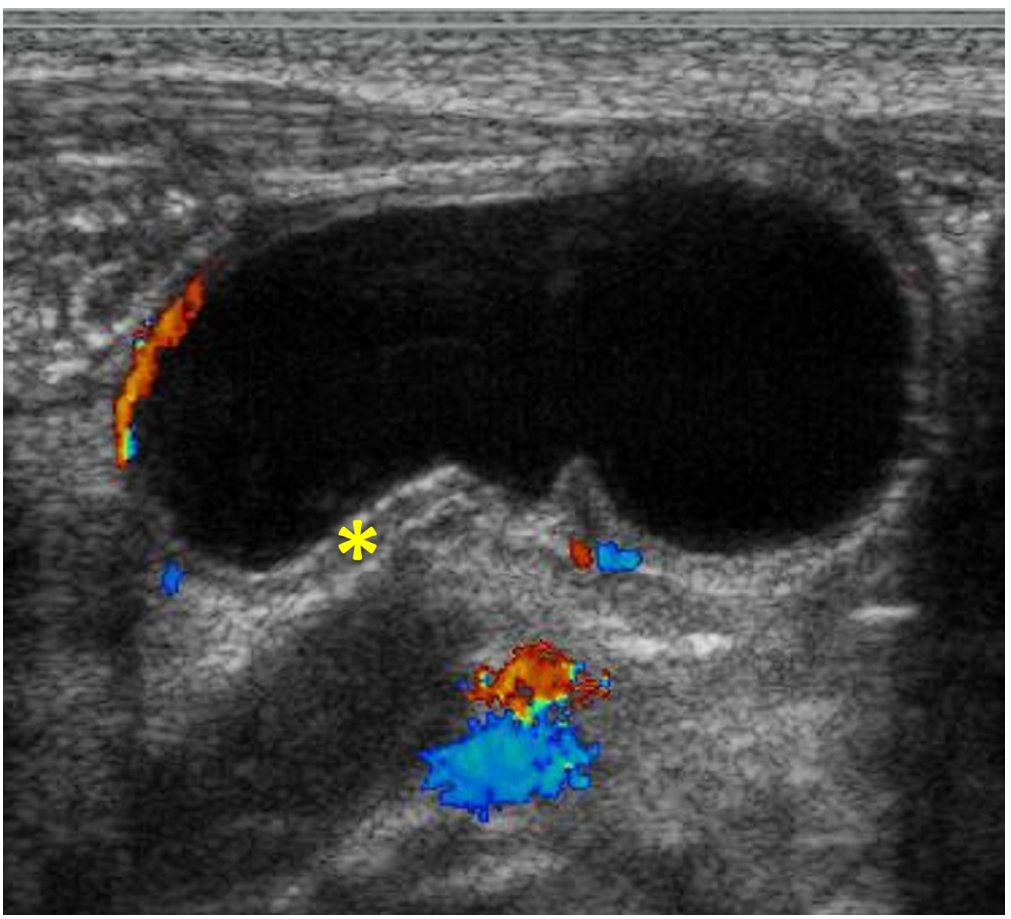
US was performed in 34 patients (75.6%), whereas CT was obtained in 15 patients; some patients underwent both studies. The most consistent finding was a cystic mass showing the double wall sign, which consists of an echogenic inner lining and a peripheral hypoechoic muscular rim (
Fig. 1). Among the 34 patients who underwent US, 28 (82.4%) were correctly identified as having a duplication cyst on US alone. Of the 11 patients who did not undergo US, two were correctly diagnosed preoperatively based on CT findings. Overall, preoperative imaging with US and/or CT contributed to the correct surgical diagnosis in 34 of 45 patients (75.6%): EDCs were directly identified in 30 patients (66.7%), and intussusception with a visible lead point was diagnosed in four patients, in whom EDC was subsequently confirmed intraoperatively as the lead point. These imaging modalities yielded variable preoperative impressions, often suggesting obstructive or cystic abdominal lesions rather than definitively identifying duplication cysts. Nevertheless, imaging findings were useful for surgical planning.
The ileum was the most common site of duplication, identified in 26 cases (57.8%). Jejunal and ileocecal duplications were each identified in five cases (11.1%). Less frequent locations included the stomach, colon, duodenum, and appendix. Most lesions showed cystic morphology (43 cases), whereas tubular duplications were identified in two cases. Communication with the adjacent bowel was identified in four cases. These communicating duplications were managed by segmental bowel resection that included the shared bowel segment.
Operative management
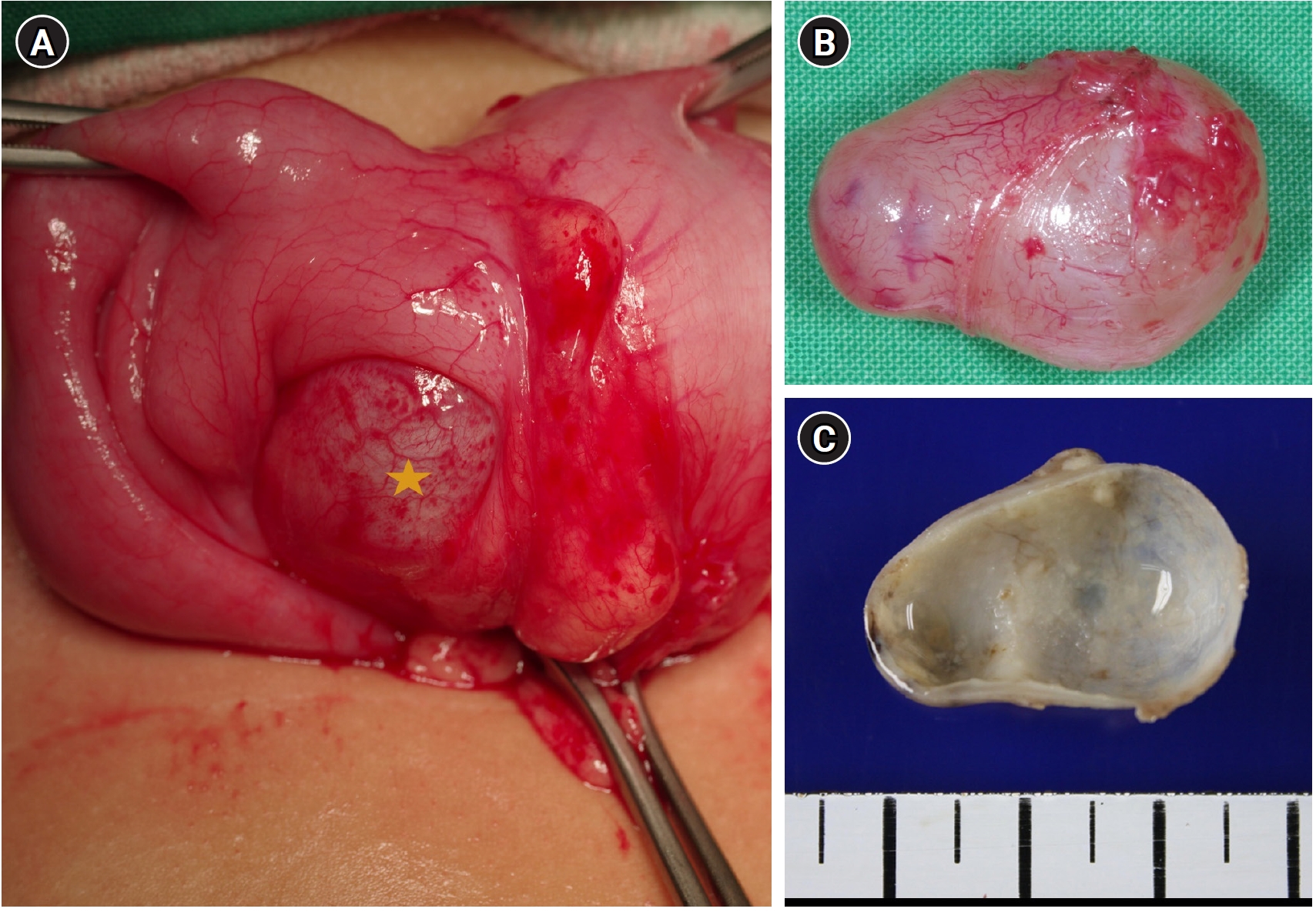
The most frequently performed procedures were small-bowel segmental resection with primary anastomosis (18 cases, some requiring adjunct procedures) and ileocecal or ileo-ascending colon resection (15 cases). Bowel-preserving procedures were performed in 12 cases, including enucleation or cyst excision in nine cases and wedge resection in three cases (
Fig. 2). Emergency surgery was required in 13 patients (28.9%) because of acute complications, including volvulus in three patients, intussusception in three, bowel obstruction in five, and perforation in two. Among the perforation cases, a jejunal tubular duplication measuring 5.8 cm in maximum dimension perforated in a 6-day-old neonate, and a 2.5-cm colonic duplication perforated in a 40-month-old child.
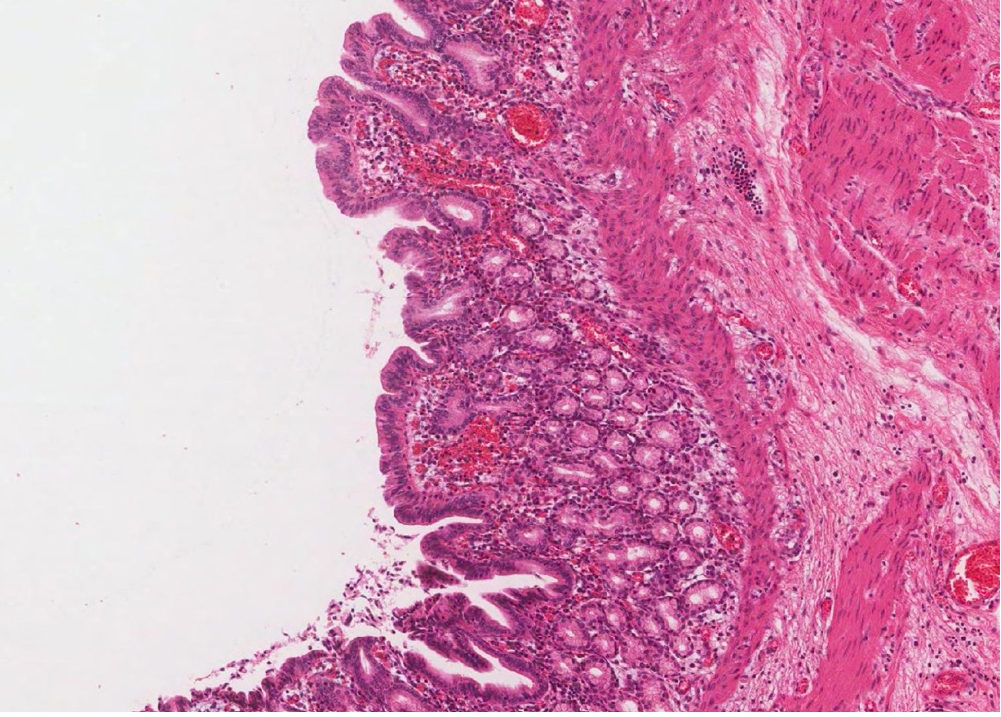
Histopathological examination was performed in 44 of 45 resected specimens; the epithelial subtype could not be determined in one case because archived slides were unavailable. Among the 44 evaluable cases, heterotopic gastric mucosa was identified in 27 cases (61.4%) (
Fig. 3), intestinal-type epithelium in nine cases (20.5%), and respiratory-type epithelium in three cases (6.8%). Five lesions (11.4%) lacked an identifiable epithelial lining. Despite the high prevalence of gastric mucosa, only one patient presented with GI bleeding.
Postoperative complications included wound infection in two patients. The median postoperative hospital stay was 7.5 days (range, 2–23 days). No recurrence of duplication cysts was identified during the available follow-up period, although follow-up duration was limited in many patients.
DISCUSSION
This 40-year single-center experience provides valuable long-term data on the characteristics and management of EDCs in children. Consistent with international literature, EDCs in our cohort were predominantly diagnosed during infancy, with 75.6% of cases presenting before 2 years of age, emphasizing their congenital origin and potential for early symptoms [
1,
3,
4,
10]. The male predominance in this cohort (male-to-female ratio, 1.6:1) is also consistent with the slight male predominance reported in general series of alimentary tract duplications.
Our findings confirm that the ileum (57.8%) is the most frequent site of EDCs, followed by the jejunum (11.1%) and ileocecal valve (11.1%). This predilection for the distal small bowel suggests a specific, although unconfirmed, vulnerability during midgut development [
2,
11]. The most common presenting symptoms, including vomiting (46.7%) and abdominal pain (26.7%), illustrate the mechanical effects of these space-occupying lesions.
A key finding of this series was the high rate of complications requiring emergency surgery, which occurred in 28.9% of patients with EDCs. Bowel obstruction was the most common indication for emergency surgery (5 cases), followed by volvulus and intussusception (3 cases each) and perforation (2 cases). These findings underscore the need for a high index of clinical suspicion for EDCs in infants presenting with acute abdominal symptoms, because duplication cysts can serve as pathological lead points for intussusception or precipitate bowel volvulus [
8]. The need for prompt surgical intervention in these emergency settings further highlights the importance of preoperative diagnosis.
The frequent use of US in this cohort (75.6%) reflects its noninvasive nature and effectiveness in identifying the characteristic double wall sign of cystic lesions in the pediatric abdomen [
1,
2,
4]. Among the 34 patients who underwent US, 28 (82.4%) were correctly identified as having a duplication cyst, underscoring the high diagnostic accuracy of this modality when the double wall sign is recognized. The increasing rate of prenatal US diagnosis in recent decades, as suggested by our series in which 7 of 8 prenatally detected cases underwent surgery after 2000, mirrors global trends and facilitates planned delivery and timely postnatal management.
Pathologically, the strong predominance of cystic morphology in this series is consistent with previous reports. The presence of heterotopic gastric mucosa in 27 of 44 evaluable EDCs (61.4%) is clinically relevant. Ectopic gastric mucosa can cause peptic ulceration and potentially life-threatening hemorrhage or perforation because of acid secretion [
12]. Notably, only one patient with gastric mucosa presented with GI bleeding in our series, suggesting that the clinical manifestations of ectopic mucosa may not always correlate directly with its presence or that acid production was insufficient in other cases. The low incidence of bleeding despite the frequent presence of gastric mucosa may reflect limited acid secretion, small mucosal volume, or early surgical removal before ulceration developed. Nonetheless, the potential for malignant transformation, although extremely rare, supports complete excision [
10].
The surgical approach, including ileo-ascending colon resection and small-bowel resection, was determined by the lesion location and degree of involvement of the adjacent bowel. For most cystic duplications, complete excision with segmental bowel resection remains the standard of care because it fully removes the shared wall and any ectopic mucosa. However, when the cyst is well defined and easily separable from the bowel wall, bowel-preserving procedures such as enucleation or wedge resection are viable alternatives [
9], as demonstrated in 12 cases (26.7%) in our series. Overall, postoperative outcomes were favorable, with low morbidity. These results demonstrate that, despite the complexity of these congenital anomalies, excellent outcomes can be achieved over a long period at a specialized pediatric surgical center.
This study has several limitations. Its retrospective, single-center design may have introduced selection bias. In addition, the 40-year study period spans substantial changes in diagnostic modalities and surgical techniques, which may have influenced management strategies and limited direct comparisons across eras. Information on prenatal detection was based partly on retrospective parental reports, limiting precise evaluation of its influence on surgical timing. However, the relatively large number of patients accrued over this extended period is a significant strength and provides valuable data on a rare condition.
In conclusion, this 40-year retrospective analysis of EDCs in children confirms that EDCs are rare congenital anomalies that primarily present within the first 2 years of life. The ileum is the most common site, and clinical presentation is often related tocomplications such as bowel obstruction, volvulus, and intussusception, which require emergency surgical intervention in a substantial proportion of patients. Cystic morphology predominates, and the presence of heterotopic gastric mucosa requires careful pathological evaluation. US is the key diagnostic modality. Prompt and complete surgical excision remains the definitive treatment and is associated with favorable short-term postoperative outcomes, with no recurrence observed during the available follow-up period in this specialized setting. This extensive single-center experience provides substantial evidence supporting proactive management strategies to prevent life-threatening complications associated with EDCs.
NOTES
-
Authors’ contributions
Conceptualization: YJK, EJ. Data curation: YJK, EJ. Formal analysis: YJK, EJ. Investigation: YJK, EJ. Methodology: EJ. Project administration: YJK, EJ. Visualization: YJK, EJ. Writing–original draft: YJK, EJ. Writing–review & editing: EJ. All authors read and approved the final manuscript.
-
Conflict of interest
None.
-
Funding
None.
-
Data availability
Data of this research is available from the corresponding author upon reasonable request.
Fig. 1.Abdominal ultrasonography showing a well-defined cystic lesion. The image demonstrates the characteristic double wall sign, or muscular rim sign, indicated by the asterisk. This sign consists of an inner hyperechoic layer representing the mucosa and submucosa and an outer hypoechoic layer representing the smooth muscle propria. This characteristic finding is valuable for the preoperative diagnosis of enteric duplication cysts.
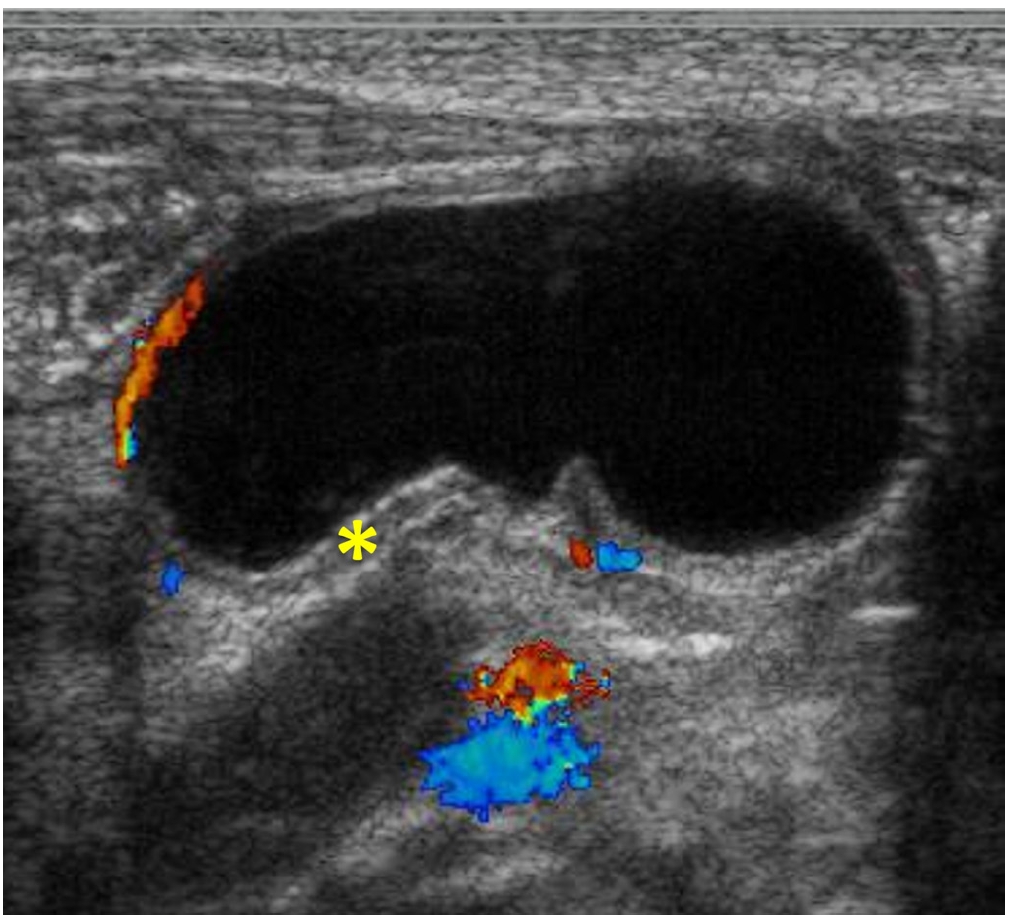
Fig. 2.Intraoperative and macroscopic findings of the duplication cyst. (A) An ileocecal duplication cyst, indicated by the star, is located on the mesenteric side of the ileocecal valve. (B) Surgical view after enucleation of the cyst. (C) Cross-sectional view of the resected specimen showing the internal structure of the cyst.
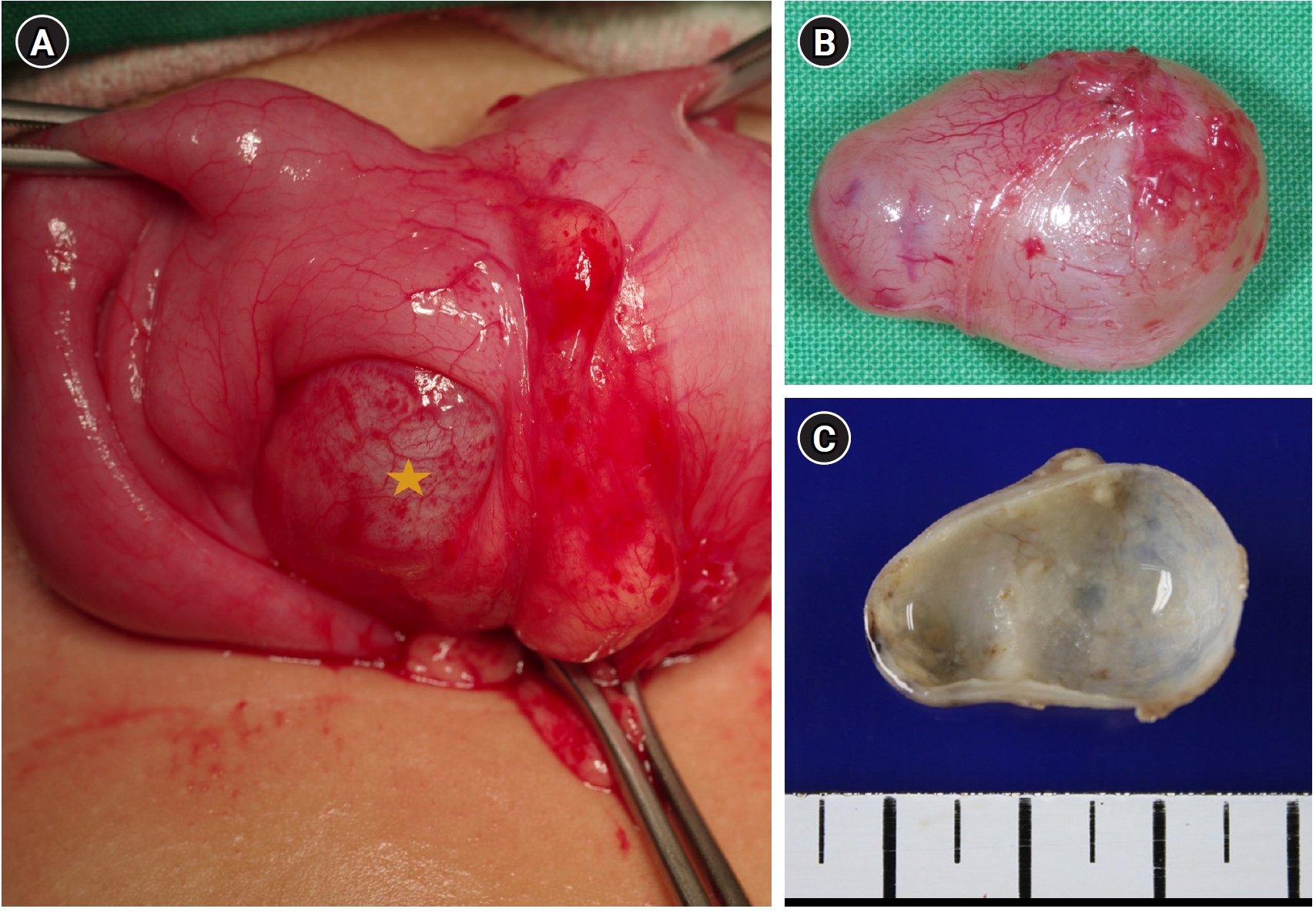
Fig. 3.Histopathological findings of the duplication cyst (H&E stain, ×100). Microscopic examination shows a cyst wall lined with gastric mucosa, characterized by foveolar epithelium and underlying gastric glands. Adjacent to the mucosa, a well-developed, distinct layer of smooth muscle, the muscularis propria, is observed, confirming the diagnosis of a true alimentary tract duplication cyst. Prominent vascular congestion and focal inflammatory cell infiltration are noted within the lamina propria.
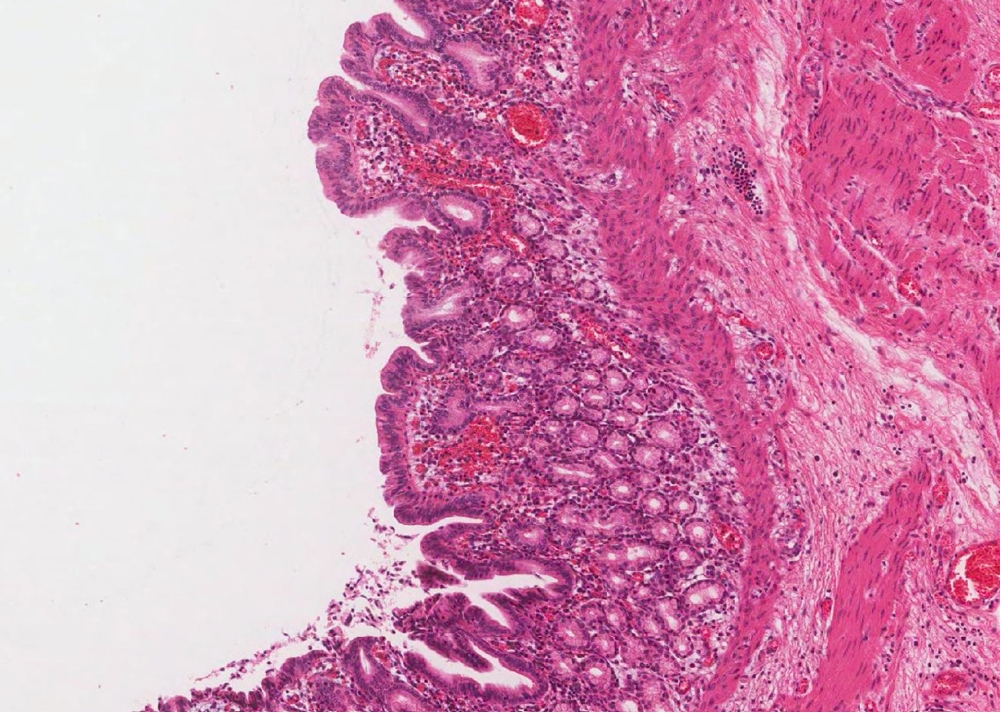
Table 1.Demographic and clinical characteristics of patients with enteric duplication cysts (n=45)
Table 1.
|
Characteristic |
Value |
|
Sex |
|
|
Male |
28 (62.2) |
|
Female |
17 (37.8) |
|
Age at surgery |
|
|
Median (range) (mo) |
4.7 (0.1–127.2) |
|
<1 yr |
27 (60.0) |
|
1–2 yr |
7 (15.6) |
|
>2 yr |
11 (24.4) |
|
Anatomic location |
|
|
Ileum |
26 (57.8) |
|
Jejunum |
5 (11.1) |
|
Ileocecal valve |
5 (11.1) |
|
Stomach |
3 (6.7) |
|
Colon/cecum |
3 (6.7) |
|
Duodenum |
2 (4.4) |
|
Appendix |
1 (2.2) |
|
Pathological feature |
|
|
Morphology (cystic/tubular) |
43/2 |
|
Luminal communication (noncommunicating/communicating) |
41/4 |
|
Size, maximum dimension (cm) |
3.5 (1.2–7.5) |
|
Presence of ectopic gastric mucosa |
27/44 (61.4) |
|
Clinical presentation |
|
|
Emergency surgery |
13 (28.9) |
|
Elective surgery |
32 (71.1) |
REFERENCES
- 1. Xiang L, Lan J, Chen B, Li P, Guo C. Clinical characteristics of gastrointestinal tract duplications in children: a single-institution series review. Medicine (Baltimore) 2019;98:e17682.
- 2. Losefsky Q. A comprehensive review of enteric duplication cysts, their pathophysiology, presentation, and treatment. J Clin Exp Gastroenterol 2022;1:1-4.
- 3. Kim DY, Kim SC, Kim IK. Gastrointestinal duplications in childhood. J Korean Assoc Pediatr Surg 2001;7:26-30.
- 4. Holcomb GW, Murphy JP, St. Peter SD, editors. Holcomb and Ashcraft's pediatric surgery. 7th ed. Elsevier; 2020.
- 5. Ladd WE. Duplications of the alimentary tract. Southern Med J 1937;30:363-71.
- 6. Gross RE, Holcomb GW, Farber S. Duplications of the alimentary tract. Pediatrics 1952;9:448-68.
- 7. Holcomb GW, Gheissari A, O'Neill JA, Shorter NA, Bishop HC. Surgical management of alimentary tract duplications. Ann Surg 1989;209:167-74.
- 8. Gebreziher YT, Tadesse FM, Gebremedin DM, Gebre BT. Enteric duplication cyst with segmental gut volvulus in an infant: a case report. Sage Open Pediatr 2025;12:30502225251325619.
- 9. Patino Mayer J, Bettolli M. Alimentary tract duplications in newborns and children: diagnostic aspects and the role of laparoscopic treatment. World J Gastroenterol 2014;20:14263-71.
- 10. Ma H, Xiao W, Li J, Li Y. Clinical and pathological analysis of malignancies arising from alimentary tract duplications. Surg Oncol 2012;21:324-30.
- 11. Sharma S, Yadav AK, Mandal AK, Zaheer S, Yadav DK, Samie A. Enteric duplication cysts in children: a clinicopathological dilemma. J Clin Diagn Res 2015;9:EC08-11.
- 12. Mehrotra B, Mehrotra S, Kapoor AK, et al. Colonic duplication cyst with gastric heterotopia haemorrhage and mucosal ulceration: a case report. J Med Sci Clin Res 2023;11:100-2.