ABSTRACT
A case of congenital ectopic scrotum in neonatal period is described. The ectopic scrotum was located in the right inguinal area and the left hemiscrotum was found in normal location and each hemi-scrotum contained their testis. The neonate also had imperforate anus as low anorectal malformation with spinal abnormalities (hemi-sacrum and hemi-pelvis), right knee flexion contracture and right club foot. The embryological explanation in the literature of ectopic scrotum and its associated anomalies is discussed.
-
Keywords: Ectopic; Scrotum; Sacral agenesis; Anorectal malformations
INTRODUCTION
Congenital scrotal disorders, which includes ectopic scrotum, are unusual anomalies. The etiology of ectopic scrotum is not clear. The ectopic scrotal location is variable and it may be associated with various anomalies. We present a case of congenital scrotal ectopia with associated musculo-skeletal anomalies and imperforate anus.
CASE REPORT
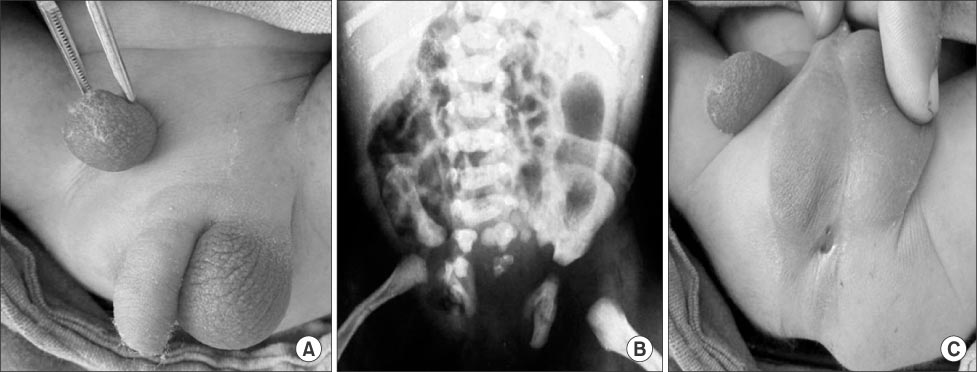
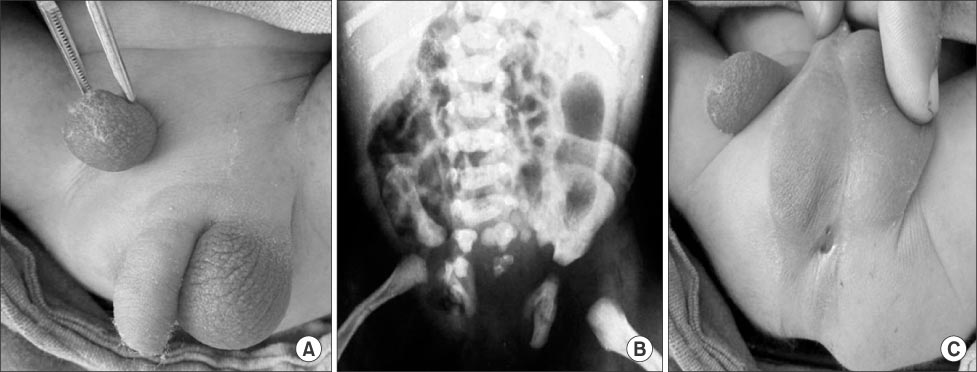
A two-day-old male neonate was admitted with us for ectopic scrotum and imperforate anus. There was no family history of any similar congenital anomaly. Physical examination showed an ectopic scrotum in the right inguinal area. The opposite left side hemiscrotum was normotopic and both testes were located in each hemiscrotum. Scrotal raphe was moderately developed. The phallus was normal in gross. He also had low anorectal malformation in the form of a perineal fistula and a flexion contracture of right knee (arthrogryoposis) and ipsilateral club foot (talipes equino varus) as musculoskeletal anomalies (
Fig. 1).
Plain radiography of the spine revealed hemisacrum and hemipelvis (
Fig. 1). Abdominal sonography showed a normal upper urinary tract.
He made an uneventful recovery after V-Y anoplasty for the low anorectal malformation. Excision of the right ectopic scrotum and implantation of the right testis into the native scrotum is planned at a later stage.
DISCUSSION
Congenital scrotal disorders are rare anomalies and can be divided into four groups: peno-scrotal transposition, bifid scrotum, ectopic and accessory scrotum [
1]. Ectopic scrotum can be found in the inguinal, supra-inguinal, infra-inguinal, perineal locations or medial thigh [
2].
The embryology of scrotal development and its associated anomalies are poorly understood. Scrotal development begins at 4 weeks' gestation with the formation of paired labio-scrotal swellings lateral to the cloacal membrane, flanking the genital tubercle which elongates to form the penis. After 12 weeks, these swellings migrate infero-medially towards each other and fuse to form the scrotum. Simultaneously, at around the 5th week, gubernaculums develops as a condensation of mesenchymatous tissue extending from the mesonephros to the abdominal wall. The inferior gubernaculum inserts into the labio-scrotal swellings to descend the testis [
3].
Any defect in distal gubernacular formation, due to its anatomical and chronological association with scrotal development, can therefore prevent the migration of labio-scrotal swellings resulting in unilateral scrotal ectopia. This misdirected gubernacular attachment also leads to the testes being positioned in the ectopic scrotum in most cases. Surgical treatment of ectopic scrotum involves scrotal transposition and orchiopexy.
The causes which can lead to gubernacular defects can be mechanical, genetic, chromosomal or teratogenic. As proposed by Stephens [
4], a mechanical pressure effect on the developing fetus can explain the perineal anomalies in our case, including the anorectal malformation. Such pressure can occur in pregnancy-related complications like oligohydramnios and breech presentation. This along with a local disproportion in the size of the fetus and chorionic sac at around 6 to 8 weeks can lead to an abnormal flexed limb posture. In this position, the contralateral heel can press upon the region of the developing scrotum. Signs of compression can also be evident in the foot in the form of club foot deformity, as in our case.
Failure of normal embryogenesis seems unlikely in this case in the absence of any associated genito-urinary anomalies like hypospadias, diphallia, penile torsion, or renal agenesis. Genetic defects more commonly account for femoral ectopic scrotum and their association with systemic anomalies involving distant sites as lip, palate and maxilla.
However, the association of lower spine agenesis in the form of hemi-sacrum and hemi-pelvis may represent the perturbation of adjacent structures by single dysmorphogenic event acting during late blastogenesis, rather than a random association or counter compression anomalies. If this embryologic insult is considered to occur at the mid-posterior axis mesoderm, the range of anomalies as seen in the case reported can well form a part of the caudal regression syndrome, representing polytopic field defects [
5].
The above set of abnormalities thus can be explained from three different but seemingly related associations. Our patient fulfils features of both VACTERL (vertebral, anal, cardiac, tracheoesophageal, renal, and limb anomalies) association and caudal regression syndromes which occur due to insults during early pregnancy. However, fetal akinesia due to fetal abnormalities or maternal disorders can lead to arthrogryposis (which may have joint contractures and club foot) and may lead to development of contractures which can lead to abnormal developments by counter compression mechanisms. Thus the primary event leading to this set of abnormalities is still uncertain [
3,
4,
5].
The explanation of such conglomeration of disorders requires more data from fetal embryology and may prove useful in defining the embryogenesis of these complex disorders in future.
NOTES
-
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1. Sule JD, Skoog SJ, Tank ES. Perineal lipoma and the accessory labioscrotal fold: an etiological relationship. J Urol 1994;151:475-477.
- 2. Lamm DL, Kaplan GW. Accessory and ectopic scrota. Urology 1977;9:149-153.
- 3. Spears T, Franco I, Reda EF, Hernandez-Graulau J, Levitt SB. Accessory and ectopic scrotum with VATER association. Urology 1992;40:343-345.
- 4. Stephens FD. Embryology of the cloaca and embryogenesis of anorectal malformations. Birth Defects Orig Artic Ser 1988;24:177-209.
- 5. Sen KK, Patel M. Caudal regression syndrome. Med J Armed Forces India 2007;63:178-179.
Fig. 1(A-C) Photographs show ectopic scrotum in the inguinal region with low anorectal malformation with sacral agenesis.
Citations
Citations to this article as recorded by

- Isolated Supra‐Inguinal Ectopic Scrotum in an Infant: A Case Report
Kamal Nain Rattan, Sargam Devi, Neha Choudhary, Pragati Yadav, Jasbir Singh
Journal of Paediatrics and Child Health.2026;[Epub] CrossRef - ARM in ARM? Investigating the co-occurrence of anorectal malformations and labioscrotal anomalies
Patrick G. G. Sharman, Maria Randazzo, Ian Jones, Ingo Jester
Pediatric Surgery International.2026;[Epub] CrossRef - Ectopic Scrotum with Undescended Testis
Dinesh Kumar Barolia, Aditya Pratap Singh, Sunil Kumar Mehra, Vinita Chaturvedi, Gurudatt Raipuria
Medical Journal of Dr. D.Y. Patil Vidyapeeth.2021; 14(1): 64. CrossRef - One stage rotation flap scrotoplasty and orchidopexy for the correction of ectopic scrotum: A case report
Irfan Wahyudi, Isaac Ardianson Deswanto, Gerhard Reinaldi Situmorang, Arry Rodjani
Urology Case Reports.2019; 25: 100886. CrossRef