
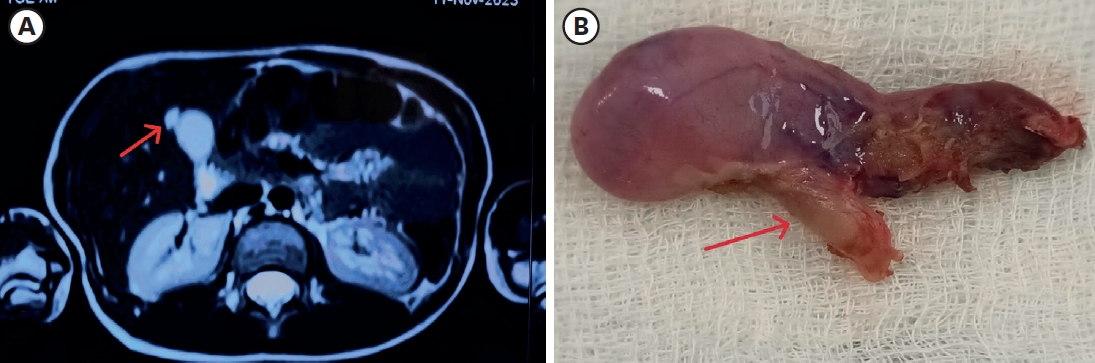
The perforation and subsequent panperitonitis as one of the complications of a Meckel diverticulum is a rare complication, especially in infants. Complication of Meckel diverticulum, preoperative and operative patient's mean age is about 5 years old. A 13-month-old male infant presented at our emergency room with currant jelly stool of about 24 hours duration. Intussusception or bacterial enteritis was initially suspected. Gastrointestinal ultrasonography showed no evidence of intussusception or appendicitis. On the 3rd hospital day, he suddenly showed high fever and irritability. Abdominal CT suggested intraperitoneal and retroperitoneal abscess with air collection due to possible bowel perforation. The final diagnosis of perforation of Meckel diverticulum was made by laparoscopy and biopsy. We report a very rare case with perforation of Meckel diverticulum in infant period.
Citations
Meckel's diverticulum (MD) has various clinical presentations and due to the limitation of imaging studies, pre-operative diagnosis is a challenge in pediatric patients. Recently, laparoscopic exploration has been suggested as a favorable method for the diagnosis and treatment of complicated MD. We investigated the results of laparoscopic-assisted surgery compared with open technique. We retrospectively studied patients who underwent resection of complicated MD at our institute from 1997 to 2010 and compared 11 treated by laparoscopic-assisted diverticulectomy (LD) with 11 treated by open diverticulectomy (OD) for complicated MD. Operation time was not significantly different in the two groups. Hospital stay and time to diet were not significantly different. Two patients were re-admitted due to mechanical ileus in the LD group. None of patients in either group needed re-operation. Considering the possibility of false-positive results with imaging studies and the cosmetic benefit, laparoscopic-assisted surgery is a safe and effective treatment modality to diagnose and treat complicated Meckel's diverticulum.
Citations
The term “Littre's hernia” was originally defined by Reinke in 1841 as “the presence of a Meckel's diverticulum in any hernia sac.” Littre's hernia is a very rare disease, which accounts for less than 1% of all Meckel's diverticula. We report a case of Littre's hernia experienced in a 45 day-old infant.
Citations
Meckel's diverticulum is the most common congenital anomaly of gastrointestinal tract in children. The incidence of complicated Meckel's diverticulum is about 4%. The major complications of Meckel's diverticulum are bleeding, intussusception, obstruction and perforation. The aim of this study was to investigate the clinical manifestations and the role of laparoscopic surgery in complicated Meckel's diverticulum in children. We retrospectively reviewed the medical records of 19 patients with complicated Meckel's diverticulum who underwent operation at Asan Medical Center between Jan. 1990 and Apr. 2007. Male to female ratio was 11:8, and median age was 1 year (1 day-13 years). The most frequent symptom was hematochezia (68%), followed by irritability or abdominal pain (16%), vomiting (11%), and abdominal distension (5%). Two operative procedures were performed; small bowel resection with anastomosis (68%) and diverticulectomy (32%). The operation proven complications of the Meckel's diverticulum were bleeding (68%), intussusception (16%), perforation (11%) and obstruction (5%). Ectopic tissues found by postoperative pathologic examination were gastric (84%) and pancreatic (11%). Hospital stay after laparoscopic operation for bleeding Meckel's was 5 days (median) and average first postoperative feeding was 1.5 days. On the contrary, hospital stay for open surgery was 7 days and first feed was 3 days. In summary, the most common compliation of Meckel's diverticulum in children was bleeding and ectopic gastric tissues were present in 84%. Laparoscopic procedure seemed to be useful for diagnosis as well as for definitive treatment.
Citations
A vitelline duct (VD) anomaly is a relatively common congenital abnormality of the umbilical area. The anomalies include patent vitelline duct (PVD), cyst, fistula or sinus. The incidence is approximately 2% of the populations, but development of symptoms is rare. Recently, we experienced two cases; PVD accompanied by a smallomphalocele and intestinal volvulus due to mesenteric band between Meckel's diverticulum and the mesentery. Thereafter,we evaluated the data of vitelline duct anomalies for 27 years. From 1980 to 2006, 18 cases of VD anomalies were reviewed based on the hospital records retrospectively. There were 15 boys and 3 girls and age ranged from 2 days to 15 years. Among the 18 cases, 15 cases were symptomatic and consisted of Meckel's diverticulum (10 cases), PVD (4 cases) and umbilical polyp (1 case). Three asymptomatic cases of Meckel's diverticulum were found incidentally were and were observed without resection. Ten cases of Meckel's diverticulum were presented with intestinal bleedings (4 cases), intestinal obstructions (5 cases) and perforation (1 case). Wedge resections and segmental resections of ileum were performed in 8 patients and 2 patients, respectively. Postoperative complications were adhesive ileus (1 case) and wound seroma (1 case). Small omphaloceles were accompanied in two of 4 PVD patients. There was 1 small omphalocele case which was accompanied by a prolapse of ileum. In summary, VD anomalies were more common in male and more than half of them were found in patients less than 1 year of age. PVD was diagnosed most frequently in neonates. Meckel's diverticulum presented with intestinal obstruction more frequently than bleeding.
Citations
An 11-year-old girl with history of two previous attacks of acute pancreatitis was admitted to another hospital. On physical examination, she had epigastric tenderness. Laboratory studies included amylase of 657IU/L and lipase of 3131IU/L. Abdominal computed tomography (CT) scan suggested necrosis in 30% of pancreas. To establish the cause of recurrent pancreatitis, endoscopic retrograde cholangiopancreatography (ERCP) was performed after acute pancreatitis subsided. Duodenoscopic view revealed a blind sac covered by normal duodenal mucosa at the second portion of the duodenum. Barium upper gastrointestinal series (UGI) showed a large sac separated from adjacent duodenal lumen by a radiolucent band. Diagnosis of intraluminal duodenal diverticulum (IDD) was made and endoscopic excision was considered. The apex of the diverticulum was incised endoscopically using a needle knife papillotome. At a follow-up endoscopy one day after procedure, bleeding from the incised edge of diverticulum was noted. Despite hemoclipping and injection of hypertonic saline-epinephrine solution by under the endoscopy, hemostasis was unsuccessful. She was transferred to the Kyungpook National University Hospital after resuscitation. Open duodenotomy and excision of the diverticulum were performed. She has recovered well from surgery and remains asymptomatic.
Meckel's diverticulum (MD) occurs in approximately 2 % of the population. The major complications of MD are bleeding, intestinal obstruction, infection and perforation. Perforation is the least common but most serious complication, the incidence od which is about 5-10 %. The causes of perforation are inflammatory diverticulitis and peptic ulceration. the purpose of study is to review the characteristics of perforated MD in children. Six patients with perforated MD who had been operated upon at the Department of Pediatric Surgery, Yeungnam University Hospital from April 1984 to July 2001 were included. Male predominated in a ratio of 5:1 and there were 2 neonates. The chief complaints were abdominal pain and distension. Half of the children showed a past history of bloody stools. The average age was 4 year and 9 months. The mean distance from the ileocecal valve to the diverticulum was 60 cm. Average length of the diverticulum was approximately 3 cm and width was 1.7 cm. The perforation site was the tip of the diverticulum in 3 cases, the base in 2 cases and along the lateral border in one. In two patients, ectopic gastric mucosa was found in the specimen. All of the patients were operated upon with a diagnosis of peritonitis of unknown etiology. In conclusion, when a child shows symptoms of acute abdomen or peritonitis, especially in boys, with the history of bloody stools and episodic abdominal pain, perforated MD should be suspected.
The major complications of Meckel's diverticulum(MD) are bleeding, intestinal obstruction, infection, umbilical fistula and perforation. Although the relative incidences vary between authors, bleeding is the most common complication in children. The aim of our study is to show the symptomatic guideline for the diagnosis of the bleeding MD. Eight cases with bleeding MD which were operated upon at the department of Pediatric Surgery, Yeungnam University Hospital from April 1985 to April 2001 were reviewed. Half of the patients were under 2 years of age and all patients were male. All patients were preoperatively diagnosed by previous history of intestinal bleeding (melena, hematochezia) and 99mTc pertechnetate MD scan. Segmental resection and end-to-end anastomosis was performed in 6 patients and diverticulectomy in 2 patients. Heterotropic gastric mucosa was found in 6 patients. Postoperative complication was not observed in any cases. In conclusion, in any male children with obscure intestinal bleeding, especially less than 2 years of age, bleeding MD must be suspected. It seems to us that 99mTc pertechnetate MD scan is a useful tool to diagnose bleeding MD.
The embryological and anatomical features of urachal anomalies have been well defined. Because of the variable clinical presentation, uniform guideline for evaluation and treatment are lacking. Although urachal remnants are rarely observed clinically, they often give rise to a number of problems such as infection and late malignant changes. Therefore, a total assessment of the disease with a particular focus on embryology, anatomy and clinical symptoms, as well as the most advisable management, is called for. Twenty six patients with urachal remnants were treated at the Department of Pediatric Surgery from August 1980 to June 1998. Of these 26, 9 were classified as patent urachus, 11 as urachal sinus, 4 urachal cyst, 1 urachal diverticulum and 1 alternating sinus. The group consisted of 11 males and 15 females. The age distribution was 20 neonates, 3 infants, 2 preschoolers and 1 adult. Infection was the most frequent complication and Staphylococcus aureus was the predominant causative microorganism. Fistulogram was performed in 4 cases and ultrasound examination disclosed cysts or sinus in 7 cases. Excision was performed in 24 patients and incision and draniage in 2 cases as a primary treatment. There was no postopreative complication or recurrence.
The incidence of Meckel's diverticulum(MD) in general population has been assessed as 2 percent. The major complications of MD are bleeding, perforation, and intestinal obstruction. In spite that the complication rate of Meckel's diverticulum is relatively high(about 4.2% during a lifetime), the preoperative diagnostic rate of complicated MD is very low. Authors investigated the clinical characteristics of complicated MD to improve the diagnostic rate. 16 patients with complicated Meckel's diverticulum who were operated upon at the Department of Pediatric Surgery, Seoul National University Children's Hospital from June 1985 to December 1993 were reviewed. Among the 16 patients with complicated MD, 12 patients(75%) were under 2 year-old and male were predominant(88%). The most common complication was bleeding patients with bleeding MD (8 cases) were diagnosed preoperatively as MD. 8 patients with other complications(perforation : 4 cases, obstruction: 4 cases) could not be suspected as complicated MD except one patient who had previous history of melena. These patients were diagnosed after exploratory laparotomy under the various impression other than MD. Among 12 patients with ulcer related complications such as bleeding and perforation, heterotopic gastric mucosa was found in 11 patients. In conclusion, in any children with unexplained acute abdomen, especially under 2 years old, complicated MD must be included in differential diagnosis. In children with obscure lower gastrointestinal bleeding,99m Tc-pertechnetate scintigraphy is a useful diagnostic tool to rule out bleeding MD.
 First
First Prev
Prev

