Division of Pediatric Surgery, Department of Surgery, Chonbuk National University Hospital, Chonbuk National University Medical School, Jeonju, Korea.
Copyright © 2016 by the Korean Association of Pediatric Surgeons
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.


KTS, Klippel-Trenaunay-Weber syndrome; Rt., right; Lt., left; GSV, great saphenous vein; SSV, small saphenous vein; PV, popliteal vein; CEAP, Clinical-Etiology-Anatomy-Pathology classification.
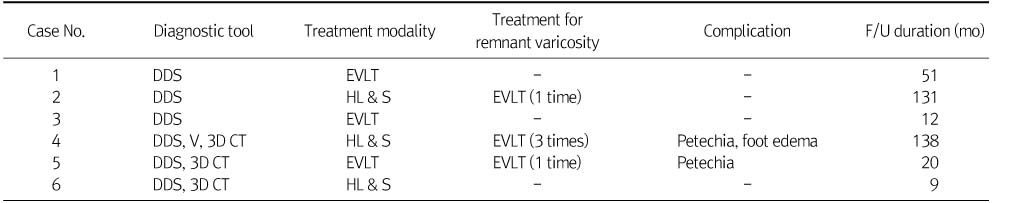
DDS, duplex Doppler scan; V, venography; 3D, three-dimensional; EVLT, endo-venous laser therapy; HL & S, high ligation and stripping; F/U, follow-up.
KTS, Klippel-Trenaunay-Weber syndrome; Rt., right; Lt., left; GSV, great saphenous vein; SSV, small saphenous vein; PV, popliteal vein; CEAP, Clinical-Etiology-Anatomy-Pathology classification.
DDS, duplex Doppler scan; V, venography; 3D, three-dimensional; EVLT, endo-venous laser therapy; HL & S, high ligation and stripping; F/U, follow-up.