

Situs inversus, polysplenia and annular pancreas are unusual anomalies individually, and are extremely rare in combination. A 3 years old boy presented with failure to thrive and symptoms of chronic upper gastrointestinal obstruction. After adequate radiological investigations, he was explored and managed with a duodeno-duodenostomy. and is doing well on a 1 year follow-up. The preoperative radiological assessment is of paramount importance, so as to avoid any intra-operative surprises.
Situs inversus, polysplenia and annular pancreas are unusual anomalies individually, and are extremely rare in combination. A 3 years old boy presented with failure to thrive and symptoms of chronic upper gastrointestinal obstruction. After adequate radiological investigations, he was explored and managed with a duodeno-duodenostomy, and is doing well on a 1 year follow-up. The preoperative radiological assessment is of paramount importance, so as to avoid any intra-operative surprises.
Situs inversus totalis (SIT) is a rare anomaly with mirror imaging of abdominal and thoracic viscera with an overall incidence of 1 in 10,000 normal population. It is usually associated with other cardiac and gastro intestinal anomalies [1]. Poly splenia (PS) is associated with situs inversus in 20%–50% of cases. annular pancreas (AP) is a congenital anomaly with incidence of 1/50,000 births where pancreatic tissue encircles the second part of duodenum leading to partial/complete obstruction [2]. Situs inversus associated with duodenal atresia is reported, however an amalgamation of SIT, AP, and PS is extremely rare.
A 3 years old male child presented with history of recurrent vomiting on and off for 2 years. Vomiting was 1–2 episodes/day, non-projectile, contained food particles, mostly during evening hours. The vomitus was non-bilious in nature. The patient had failure to thrive and the parents noticed upper abdominal distension since last 6 months which usually relieved after vomiting. The patient could tolerate only liquids for the last 1 month. On examination, the patient was pale and underweight for his age (Z score >−3 to <−2). Abdominal examination showed mild distention, the liver was palpable in the left hypochondrium 2 cm below the left costal margin. Heart sounds were heard on right side with no murmurs.
Plain chest and abdominal X-ray showed dextrocardia with higher level of left hemi diaphragm with gastric fundal air on right side (Fig. 1). Two-dimensional echocardiography showed situs inversus, dextrocardia with normal ventricular function with no other cardiac anomaly. Ultrasonography (USG) of abdomen revealed liver on left side with situs inversus and bilobed spleen on right side. Due to obscured gases pancreas was not clearly visualized. The proximal part of superior mesenteric artery and superior mesenteric vein were visualized on color Doppler. USG abdomen of both parents showed situs solitus. Upper gastro intestinal contrast was study done with non-ionic contrast which revealed gastro-esophageal junction and gastric fundus was located on right side of spine with pylorus, duodenum located on left side of spine with grossly distended stomach. Delayed images revealed slow opacification of small bowel (after 2 hours), suggestive of partial duodenal obstruction (Fig. 2). Routine blood investigations, liver and renal function test were within normal limits.

Fig. 1
Plain X-ray of situs inversus.

Fig. 2
Upper gastrointestinal contrast study showing partial duodenal obstruction and situs inversus.
Laparotomy was done under general anaesthesia and explored via left supra umbilical transverse incision. Intra operative findings showed grossly dilated stomach on right side with dilated first and second part of the duodenum, with AP followed by normal caliber third part of duodenum (Fig. 3). The Ileocecal junction was situated to the left of the abdomen and the sigmoid to the right. The liver was situated on left side along with polysplenia on the right. Wide duodeno-duodenostomy was done using 5-0 vicryl® (polyglactin). Tube feeds were started initially via trans-anastomotic tube from day 3 after surgery and gradually increased to full feeds. Oral feeds were started after postoperative day 5 and gradually shifted from liquids to solid food. After 6 months of follow-up, child has no vomiting episodes and had gained adequate weight. Ethical approval has been exempted by our institution, PGIMER ethics committee. Informed consent was taken from the parents for using patient information.
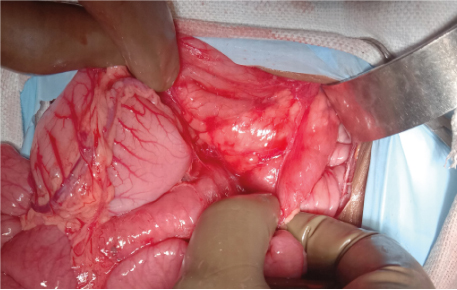
Fig. 3
Intraoperative picture of annular pancreas.
Situs solitus is normal situation of internal organs and mirror transposition of these organs is termed as situs inversus. This may be either partial or total. Our index case was SIT, transposition of both thoracic and abdominal organs. The term “Heterotaxy” is used to describe asymmetrical mispositioning of abdomino-thoracic organs associated with complex cardiac and extra-cardiac midline defects [2].
Situs anomalies have an uncharacteristic symmetry of certain viscera (thoracic and abdomen) and veins. Embryonic lateralization is complex process and is incompletely understood. Molecular lateralization begins as early as the 2nd gestational week. Multifaceted genetic pathways control the normal cilia function and celiogeneis, resulting in proper lateralization of organs [3]. In the setting of abnormal ciliary function random placement of organs occurs along with cardiac defects. The mammalian (or mechanistic) target of rapamycin (mTOR) pathway has recently emerged as an important regulator regarding symmetry breaking. The mTOR pathway governs fundamental processes such as protein translation [4]. These complex interactions indicate that there is some coherence and synchronicity in the organ placements and these are not just sporadic embryological events [2].
Helwig in 1929 coined the term “heterotaxia” for poly-splenia syndrome. Polysplenia syndrome includes 2 or more spleens or a cluster of spleniculi with wide number of abnormalities from simple to complex cardiac anomalies (atrial septal defect, endocardial cushion defects, ventricular septal defects, pulmonary stenosis, double outlet right ventricle, atrioventricular canal defects, rhythm disturbances), vascular anomalies (interruption of hepatic inferior vena cava, bilateral superior vena cava), biliary atresia, preduodenal portal vein, annular or short pancreas and mal rotation [5]. The index case had dextrocardia associated with normal cardiac function, which is otherwise rarely reported.
Splenic abnormalities can be of 3 types. (A) Absence of spleen (asplenia), (B) multiple spleen 2 or more (PS)/cluster of spleniculi and (C) single normal spleen but right sided. In a study with cases of visceral heterotaxy with congenital heart disease of 109 autopsy, spleniculli 58 (53%), polysplenia 46 (42%), and single right-sided spleen in 5 (5%) [6]. Polysplenia, asplenia, and SIT are mainly sporadic but familial cases have been reported [2]. Hence, screening USG of index case parents was done which showed situs solitus.
AP is an infrequent congenital anomaly, usually asymptomatic. Symptomatic patients present during infancy or childhood. However, few cases are reported in adult population [7]. Yigiter et al. [8] reported 22 cases of AP, all presented during infancy and all underwent surgical correction. Talabi et al. [9], reviewed case reports of situs inversus with duodenal atresia in 25 out of which 4 were associated with AP. However, none of them had polysplenia. AP is rarely associated in combination with situs inversus and polysplenia. Very few cases with multiple association are reported in literature (Table 1) [10].
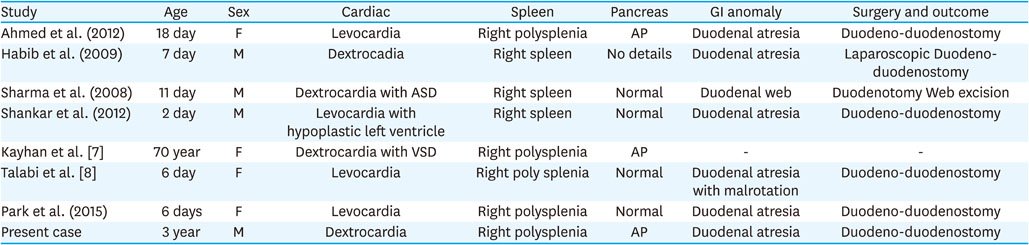
Table 1
Association of situs anomalies, spleen, pancreas, and duodenal obstruction (reports 2000 onwards)
SIT can be diagnosed easily even on plain chest and abdominal X-ray. But one needs to confirm further with echocardiography, USG and sometimes with computed tomography. Magnetic resonance imaging with magnetic resonance cholangiopancreatography may be useful for biliary and pancreatic anomalies. An upper gastrointestinal (GI) series can help in cases with duodenal obstruction [5]. The index case had presented with chronic duodenal obstruction and was diagnosed with an upper GI contrast study, which showed a possibility of duodenal web or a partial duodenal obstruction, which was confirmed as an AP in the operative findings.
To summarize, polysplenia may be associated with SIT occasionally. But this combination with AP presenting as duodenal obstruction is very rare. These patients need thorough preoperative radiological investigations so as to plan correct incision, to avoid intra operative surprises of associated GI anomalies for prognostication. Echocardiography to rule out cardiac anomalies is a must in these cases for safe anaesthesia and uneventful perioperative period.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: P.S., P.N.J.
Data curation: P.S., P.N.J.
Project administration: S.R.
Resources: P.N.J., S.R.
Supervision: P.N.J., S.R.
Writing - original draft: P.S., P.N.J.
Writing - review & editing: P.S., P.N.J.
