

Caecal duplication cysts (DCs) are rare anomalies and presentation varies according to size, site, the mucosal lining of the cyst, and age of the patient. The rarity of the condition and varied clinical presentation makes it difficult to diagnose preoperatively. A high index of suspicion and intraoperative examination of the whole bowel is essential to localize intraluminal DC. We herein describe a case of an intraluminal caecal DC in an infant along with its presentation, management, and review of pertinent literature.
Caecal duplication cysts (DCs) are rare anomalies and presentation varies according to size, site, the mucosal lining of the cyst, and age of the patient. The rarity of the condition and varied clinical presentation makes it difficult to diagnose preoperatively. A high index of suspicion and intraoperative examination of the whole bowel is essential to localize intraluminal DC. We herein describe a case of an intraluminal caecal DC in an infant along with its presentation, management, and review of pertinent literature.
Intestinal duplication cysts (DCs) are well-known anomalies and the majority are found in the ileum. There are only a few cases of caecal DCs reported in the literature. Intestinal DCs usually are extraluminal on the mesenteric side but intraluminal cysts are also described [1]. The majority present with abdominal pain, obstruction, abdominal mass, and a few may present with complications like perforation and bleeding [2]. The presentation with acute abdomen does not allow detailed investigations and so, most of the time it is an intraoperative surprise. We herein describe a case of an intraluminal caecal DC in an infant.
A 40-days old female infant was brought to our emergency room with complaints of progressively increasing abdominal distension for 10 days associated with bilious vomiting. The child was born at term via normal vaginal delivery, cried immediately after birth, and had a normal perinatal course. On initial examination, the baby was lethargic, dehydrated with pulse rate of 164/min, blood pressure of 64/42 mm Hg. The abdomen was grossly distended with shiny abdominal skin, dilated veins, and visible bowel peristalsis. Blood investigations were suggestive of elevated sodium (158 meq/L), low potassium (3.4 meq/L) and elevated urea (60 mg/dL) which were suggestive of dehydration. An abdominal X-ray showed dilated small bowel loops with multiple air-fluid levels (Fig. 1). After adequate resuscitation, the baby was taken up for emergency surgery in view of persistently high bilious aspirates with band obstruction, volvulus as our main differentials. On exploratory laparotomy, the whole small bowel was dilated till ileo-caecal junction. On careful palpation, a 3.5×3.5 cm firm mass was palpable in the caecum causing the luminal obstruction (Fig. 2A). The ileo-caecal segment was resected and ileo-ascending colon anastomosis was done. The cut section of the specimen showed a 3×3 cm cyst in the caecum with mucoid content (Fig. 2B). The postoperative period was uneventful and the child was discharged on the seventh day. Histopathology of the resected specimen was suggestive of enteric DC lined by columnar epithelium with ulcerated mucosa. At 1-year follow-up, the child had no complaints and is gaining weight adequately.

Fig. 1
Abdominal X-ray showing grossly dilated small bowel loops with paucity of rectal gas.
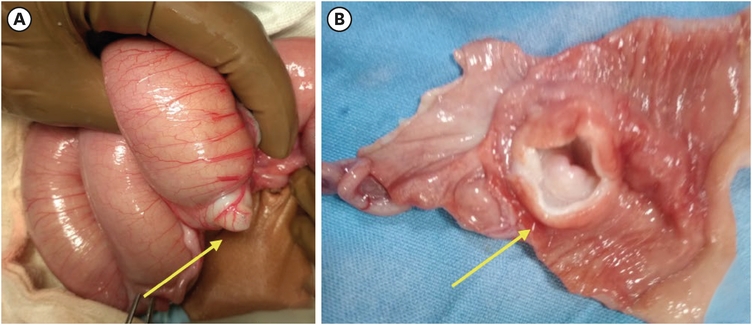
Fig. 2
A 3×3 cm firm intraluminal cyst in the caecum at the ileo-caecal junction (A) and cut section of the intraluminal cyst (B).
Intestinal obstruction is a common emergency encountered by a pediatric surgeon. The common causes in infancy include adhesion band obstruction, malrotation with volvulus, intussusception, and mesenteric cyst. However, DC is an infrequent cause of obstruction in an infant and it always comes lower down in the differential diagnosis.
Gastrointestinal DCs are fairly well-known congenital anomalies having an overall incidence of 1 in 4,500 births and vary in size, location, and presentation [3]. While colonic DCs are noted in 3% to 20% of cases, caecal DCs are extremely rare comprising 0.4% of all gastrointestinal duplications [4].
DC characteristically contains a well-defined smooth muscle layer, gastrointestinal mucosal lining, and shares a common blood supply with its parent bowel. Caecal DC’s are commonly cystic in nature and while, most of them are extraluminal, on the mesenteric side of the bowel, they may also be intraluminal as in our patient. Most of them (80%) present in the first 2 years of life and few may also be antenatally detected. Though majority present with subacute intestinal obstruction, few may also have abdominal pain, mass or bleeding similar to the DCs at other sites of gastrointestinal tract [2]. De Biagi et al. [5] reported a 2-month-old female baby with caecal duplication who presented with ceco-colic intussusception.
The accurate diagnosis of this entity requires a high index of suspicion and appropriate preoperative imaging. The radiological investigations commonly used are X-ray, ultrasonography (USG), contrast studies, and computed tomography (CT) scan. The USG is the investigation of choice and it shows a characteristic “double-wall” sign i.e., an echogenic inner mucosal layer and a hypoechoic outer muscular layer. A contrast study demonstrates a submucosal mass with mass effect extending into the lumen of the gastrointestinal tract. CT scan is not used routinely but can give relevant information when the diagnosis is not clear. Nuclear scanning can be used in cases presenting with bleeding where there is a suspicion of the presence of heterotopic gastric mucosa [6].
In the index case, only X-ray was performed preoperatively which revealed features of obstruction and as she presented in acute obstruction, the child was taken for emergency exploration after adequate resuscitation. In infants presenting with acute surgical abdomen, many a time the preoperative diagnosis is not clear and during surgical exploration, the surgeon should look for all the possible differential diagnoses if pathology is not obvious. The careful inspection and palpation of the whole small and large intestine is essential to diagnose or exclude the cause. Intraluminal pathology is difficult to diagnose unless it is obvious.
Many surgical procedures have been described to manage the caecal DC to preserve the ileo-caecal valve viz enucleation, marsupialization, or simple drainage of the cyst along the antimesenteric border with mucosal stripping and plication along the common wall [7]. Rattan et al. [8] performed resection with end-to-end anastomosis for ileal, caecal, and colonic DCs and cyst excision and mucosal stripping for gastric and duodenal cysts. The most commonly performed procedure is the resection of the involved segment of the bowel with end-to-end anastomosis as was done in the index patient. Clinically, our patient did not show any evidence of impaired absorption or reduced intestinal transit at 1-year follow-up.
In conclusion, caecal DC is a rare anomaly in an infant and mostly presents as an intraoperative surprise. Careful inspection and palpation of the whole intestine is the key to diagnose intraluminal DC. Resection of the ileo-caecal segment with anastomosis is safe and is the treatment of choice.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: S.S., R.M.
Data curation: R.M.
Supervision: S.S.
Writing - original draft: R.M.
Writing - review & editing: S.S., M.P., S.R.
