

A choledochal cyst (CC) is an abnormal dilatation of the bile duct that is known to be a precursor of cholangiocarcinoma (CCA). Biliary intraepithelial neoplasia (BilIN) is a premalignant lesion that is considered to be found during the carcinogenesis of CCA. While BilINs are frequently identified in adult populations during pathology, there has been no report of them in the pediatric population. We first report a case of BilIN incidentally diagnosed from a CC in a 7-year-old child. This case suggests that BilIN should not be overlooked in children, especially those with risk factors such as anomalous pancreaticobiliary ductal union. Also, it supports the importance of early and complete resection of CC and its impact on preventing neoplastic changes in the biliary system.
A choledochal cyst (CC) is an abnormal dilatation of the bile duct that is known to be a precursor of cholangiocarcinoma (CCA). Biliary intraepithelial neoplasia (BilIN) is a premalignant lesion that is considered to be found during the carcinogenesis of CCA. While BilINs are frequently identified in adult populations during pathology, there has been no report of them in the pediatric population. We first report a case of BilIN incidentally diagnosed from a CC in a 7-year-old child. This case suggests that BilIN should not be overlooked in children, especially those with risk factors such as anomalous pancreaticobiliary ductal union. Also, it supports the importance of early and complete resection of CC and its impact on preventing neoplastic changes in the biliary system.
Biliary intraepithelial neoplasia (BilIN) is premalignant lesion that is considered a precursor of cholangiocarcinoma (CCA) [1, 2]. It is a lesion of predominantly flat, micropapillary or pseudopapillary architecture in situ lesion that develops CCA through multistep carcinogenesis [2]. Choledochal cyst (CC) is abnormal dilatation of the bile duct that is mainly diagnosed in patients in their 1st decade (60%) and is known as one of the predisposing factors of CCA. Katabi et al. [3] reported that BilINs were identified in 10 CCs from 36 patients, and all lesions except 1 case showed metaplasia (range of age: 11–67 years old) [3]. But there has been no report from pediatric patients under 10 years of age. Herein, we present the case of BilIN diagnosed from CC of a 7-year-old child for the first time.
A 7-year-old girl visited the pediatric department of Asan Medical Center for endoscopic retrograde cholangiopancreatography (ERCP) to remove a distal common bile duct (CBD) stone. She was previously healthy and visited a nearby hospital due to abdominal pain and vomiting lasting for 13 days, and jaundice progressed the day before hospital visit. Computed tomography (CT) revealed tortuous dilatation of the extrahepatic bile duct abruptly narrowed in the distal CBD level with several distal CBD stones and anomalous pancreaticobiliary ductal union (APBDU, P-C type). The common channel was measured as 1.9 cm in length. These findings suggested type I CC related to APBDU. Secondary cholecystitis, cholangitis, and pancreatitis were additionally found (Fig. 1A). The same findings were confirmed on magnetic resonance imaging (Fig. 1B). After failure of the first ERCP at the previous hospital, she kept non per oral for one week, but symptoms and lab findings were never relieved (Table 1). So, she was determined to transfer to Asan Medical Center. ERCP was performed. Both pancreatic and CBD were successfully cannulated, and a 10 Fr. Endoscopic retrograde biliary drainage stent was retained in the bile duct for remnant stone excretion. No residual stone was found in follow-up CT in 3 days post ERCP (Fig. 2). Serum levels of liver enzymes, bilirubin, and amylase/lipase decreased to the normal range. Two months later, robotic CC excision and Roux-en-Y hepaticojejunostomy were performed. Severe adhesion and fibrosis around the CC reflecting chronic inflammation were noted. Type I CC was identified, and CBD was resected proximally above the cystic duct and distally at the upper border of the pancreas head. The patient recovered without acute complications. In ultrasonography of post-operative day (POD) 7, no abnormal finding was observed except a small fluid collection around hepaticojejunostomy. She was discharged on POD 9. In the permanent biopsy, edematous mucosal change of gallbladder (GB) and cystic duct was observed, but the diameter of the cystic duct was within the normal range (0.4 cm). In microscopic findings, papillary hyperplasia was identified. The resected CC was 2 cm in length and 2 cm in the widest circumference. It was pathologically confirmed as a CC, accompanying fibrosis and wall thickening changes of CBD, and low-grade BilIN was identified from the resected CC (Figs. 3 and 4). Papillary hyperplasia in GB suggests chronic inflammation in the biliary system due to CC such as BilIN. There was no involvement in the cystic duct and GB as in Type VI.
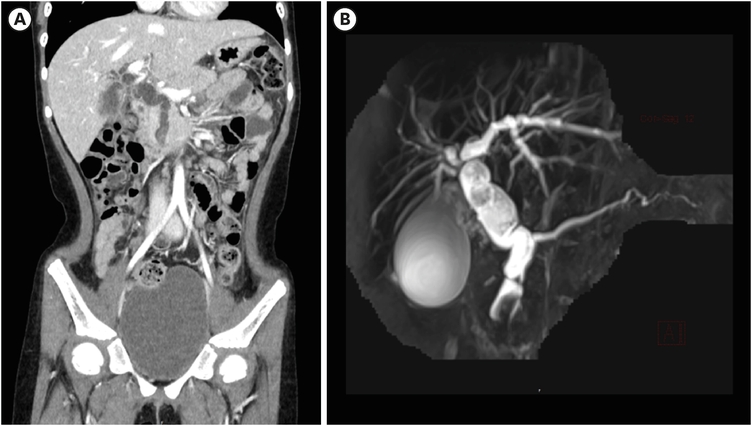
Fig. 1
CT and MRCP at initial diagnosis. (A) Contrast-enhance CT was performed, and it revealed severe dilatation of extrahepatic bile duct with wall thickening and narrowing in the distal CBD level. Also, mild dilatation of both proximal intrahepatic bile ducts were observed. Several distal CBD stones were found. (B) In MRCP, anomalous pancreaticobiliary ductal union (1.9 cm in length, C-P type) was observed.
CT, computed tomography; MRCP, magnetic resonance cholangiopancreatography; CBD, common bile duct.

Table 1
Changes in serum liver and pancreatic enzyme before and after ERCP

Fig. 2
Computed tomography follow-up after endoscopic retrograde biliary drainage insertion. (A) 3 days and (B) 7 days post procedure. Improved bile duct dilatation was observed.
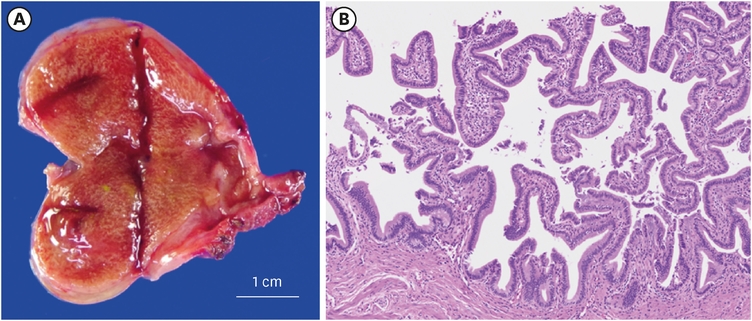
Fig. 3
Papillary hyperplasia of gallbladder. (A) Diffuse mucosal thickening of entire gallbladder and cystic duct. (B) Representative microscopic image of papillary hyperplasia (hematoxylin and eosin staining, ×100).
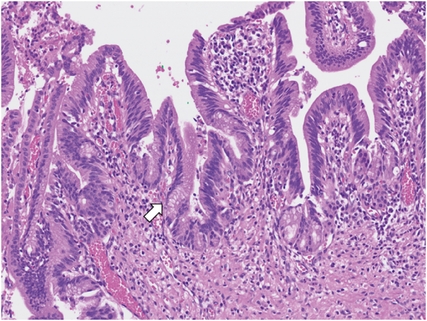
Fig. 4
Representative microscopic image of low grade biliary intraepithelial neoplasia (arrow) (hematoxylin and eosin staining, ×200).
CC is rare disease of the bile duct, with an incidence of 1 in 100, 000 to 150,000, but it occurs more frequently in Asia with incidence of one in 1,000 [4]. Although mainly diagnosed in children, it presents in 20% to 30% of patients older than 20 years. It manifests as cystic dilatation of biliary tract, predominantly in the CBD but may arise from any parts of the bile duct [3]. Alonso-Lej first classified CC based on anatomic location, the conformation, and extent of the cystic lesion in 1959, and later Todani modified the classification system that we currently use [5, 6]. Type I is most common (75%–85%), followed by type IV (13%), type III (4%) and type II (3%), and type V (1%).
There is no clear explanation for the development of CC. There are a few etiologies that explain the pathogenesis [4]. Congenital weakness of the bile duct wall derived from abnormal epithelial proliferation of the embryonic duct is one, and obstruction of the bile duct during development is another. APBDU is one of the major causes obstructing CBD and inducing the reflux of pancreatic juice into CBD. It induces chronic damage of the ductal wall by chronic cholangitis and cystic dilatation of the CBD following secondary inflammation, increased cellular proliferation, and fibrosis. APBDU is a predisposing factor promoting not only the progression but also the aggravation of CC. In previous reports, APBDU is found in 64%–97% of patients with CC [4, 7]. Park et al. [4] reported that APBDU coexisted in 73.5% of CC patients in Korea. Also, they revealed that in patients with APBDU, CC progressed earlier, and inflammation of the bile duct and periductal structures was severe.
Moreover, CC is associated with malignancy of the biliary system, including the gall bladder and bile duct. It was reported that a tumor was identified in 26% of patients with CC [8]. Adenocarcinoma is most common, but adenosquamous carcinoma, squamous cell carcinoma, and rhabdomyosarcoma were also reported. The incidence increased as patients’ age got higher. It was less than 1% in patients younger than 10 years of age, 6.8% between 10 to 20 years, and 15% in patients older than 30 years old [9]. Newsome reviewed the Surveillance, Epidemiology, and End Results Program (SEER 18) database between 1973 to 2013 and identified 7 children diagnosed with CCA developed from CC [10]. SEER is a public use data registry that collects cancer incidence and survival data from NIH (National Cancer Institute) and is based on 18 registries in the US representing 28% of the US population. The youngest patient was 11 years old. It is because carcinoma of the biliary system occurs as a result of sequential carcinogenesis from metaplasia, BilIN to carcinoma. BilIN is associated with 10% to 45% of bile duct carcinoma. Katabi reported that CC is associated with a high incidence of BilIN (28.5%) and carcinoma (14.3%) and suggested that stepwise neoplastic change from metaplasia and BilIN was observed in CC [3]. In that, BilIN, a proliferative and cytologically atypical lesion of the bile duct, is considered a precursor of CCA. Therefore, it is crucial to confirm the presence of BilIN during pathologic reading along with CCA diagnosis. However, there is no previous report on the age of onset of BilIN in children, and our patient being 7 years old means that she may develop CCA earlier than other CC patients. The co-existence of APBDU contributes to the inflammation of the bile duct and promotes neoplastic changes, emphasizing the importance of early and complete resection of CC, even in children. A multicenter study conducted by Lee and colleagues on CC in the adult population concluded that complete cyst excision reduces carcinogenesis in the biliary system [1].
This case is the first to present BilIN diagnosed in a child, suggesting that the presence of BilIN should not be overlooked in children, especially those with risk factors such as APBDU. Surveillance for CCA at an earlier age is necessary for this population. Currently, no established consensus on treatment guidelines for BilIN exist. However, previous studies have reported that resection of the lesion is the more commonly employed approach [11]. To gain a better understanding of the clinical implications of BilIN in pediatric patients, it is essential to conduct future large-scale studies that can identify its risk factors and establish long-term follow-up. This will help to verify the clinical significance of BilIN and guide its management in children.
This case highlights the importance of early and complete resection of CC and its impact on preventing neoplastic changes in the biliary system. Furthermore, in the high-risk group of BilIN, it is currently deemed essential to verify the presence of BilIN at the resection margin and ensure complete resection.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: G.S., N.J.M.
Data curation: G.S.
Formal analysis: G.S., L.Y.I.
Supervision: N.J.M.
Visualization: G.S., L.Y.I.
Writing - original draft: G.S.
Writing - review & editing: G.S., H.S., K.H., P.J., N.J.M.
