

Fournier’s gangrene is a life-threatening necrotizing fasciitis of genitalia and perineum. It is an exceedingly rare disease in infants and presents a diagnostic and therapeutic challenge for pediatric surgeons. Risk factors for Fournier’s gangrene in children include low birth weight, premature birth, trauma, burns, immunocompromising conditions, and sepsis. We report a very rare case of Fournier’s gangrene in a female infant. A 1-month-old girl visited the emergency room with a fever (39.2°C) and skin discoloration in the suprapubic area. The skin color change spread rapidly from the genitalia and inguinal area to the abdominal wall and flank. Ultrasonography and computed tomography demonstrated air bubbles in the subcutaneous layer of the suprapubic and inguinal areas, which strongly indicated Fournier’s gangrene. An emergency operation was performed; a low transverse incision was made in the suprapubic area to open subcutaneous tissue from skin to fascia and curettage and irrigation were performed. Necrotizing fasciitis improved dramatically after surgical treatment. The baby is now in good condition and has grown normally after discharge from the hospital. Clinical suspicion of Fournier’s gangrene and quick decision to surgery contributed to good prognosis. This report would be helpful to clinicians in diagnosing and treating infant patients with Fournier’s gangrene.
Fournier’s gangrene is a life-threatening necrotizing fasciitis of genitalia and perineum. It is an exceedingly rare disease in infants and presents a diagnostic and therapeutic challenge for pediatric surgeons. Risk factors for Fournier’s gangrene in children include low birth weight, premature birth, trauma, burns, immunocompromising conditions, and sepsis. We report a very rare case of Fournier’s gangrene in a female infant. A 1-month-old girl visited the emergency room with a fever (39.2°C) and skin discoloration in the suprapubic area. The skin color change spread rapidly from the genitalia and inguinal area to the abdominal wall and flank. Ultrasonography and computed tomography demonstrated air bubbles in the subcutaneous layer of the suprapubic and inguinal areas, which strongly indicated Fournier’s gangrene. An emergency operation was performed; a low transverse incision was made in the suprapubic area to open subcutaneous tissue from skin to fascia and curettage and irrigation were performed. Necrotizing fasciitis improved dramatically after surgical treatment. The baby is now in good condition and has grown normally after discharge from the hospital. Clinical suspicion of Fournier’s gangrene and quick decision to surgery contributed to good prognosis. This report would be helpful to clinicians in diagnosing and treating infant patients with Fournier’s gangrene.
Fournier’s gangrene is characterized by the rapid spread of necrotizing fasciitis along the abdominal wall and flank initiating from the urogenital area and perineum, resulting in high mortality and morbidity [1]. Fournier’s gangrene commonly affects men with diabetes in their 50s and 60s and the immunocompromised [2, 3]. It is a very rare disease in infants and presents a diagnostic and therapeutic challenge for pediatric surgeons [4]. We report a case of Fournier’s gangrene in a female infant and expect that our experience will help healthcare professionals diagnose and manage Fournier’s gangrene in infants. This manuscript was prepared following the CARE guidelines (https://www.care-
A 1-month-old girl was admitted to the emergency room (ER) at night with fever and skin discoloration at mons pubis. Before her admission, the baby exhibited inexplicable irritability and developed a fever of 39.2°C; skin discoloration at mons pubis was observed 4 hours later, prompting her admission. She appeared unwell with the following vital signs: pulse rate, 164 beats per minutes; respiratory rate, 32 breaths per minutes; and body temperature, 39.4°C. Discoloration, swelling, and tenderness at mons pubis were observed.
She was born prematurely at a gestational age of 30 weeks and 4 days, and her birth weight was 1,580 g. Her mother had no significant medical history during pregnancy; however, 18 hours of preterm premature rupture of membrane developed, necessitating an emergency cesarean section during delivery. Histological examination of the placenta revealed acute chorioamnionitis, and maternal cervix culture showed the presence of Enterococcus faecalis and Streptococcus agalactiae. Enterococcus faecalis was also cultured from the baby’s umbilical cord blood, and she was treated with intravenous antibiotics. Medical care for prematurity was provided to her in the neonatal intensive care unit (NICU), with no need for invasive procedures. She had no neonatal complications of prematurity, and no systemic infection was detected at discharge from the NICU. She was admitted to the ER after staying at home for 11 days.
Laboratory tests at the ER indicated leukopenia (white blood cell count, 1,760/μL; neutrophil, 41%; absolute neutrophil count, 720/μL). Consequently, subcutaneous administration of granulocyte colony-stimulating factor (10 mcg/kg) was initiated, along with the administration of broad-spectrum empirical antibiotics. Ultrasonography demonstrated air bubbles in the subcutaneous layer of the discolored mons pubis and inguinal areas. The skin discoloration rapidly extended to labia majora, abdominal wall and flank area. Fig. 1 illustrates the rapid progression of the skin lesion in several hours. A computed tomography (CT) scan was performed to determine the extent of necrotizing fasciitis. There were air bubbles in the subcutaneous tissue and fascia of the right groin and proximal thigh on the CT scan (Fig. 2). Based on the clinical features and radiologic findings, she was diagnosed with Fournier’s gangrene, and an emergency operation was scheduled. The patient was placed in a supine position under general anesthesia. A low transverse incision was made at mons pubis to open subcutaneous tissue from skin to fascia (Fig. 3). The tissue at the subcutaneous and the fascia layer was vulnerable, with evident exudates, and necrosis was advancing. Curettage was performed to remove necrotic tissue, followed by irrigation using a solution of betadine diluted with saline. Subsequently, the wound was covered with a dressing soaked in betadine; and it was left open and not sutured.
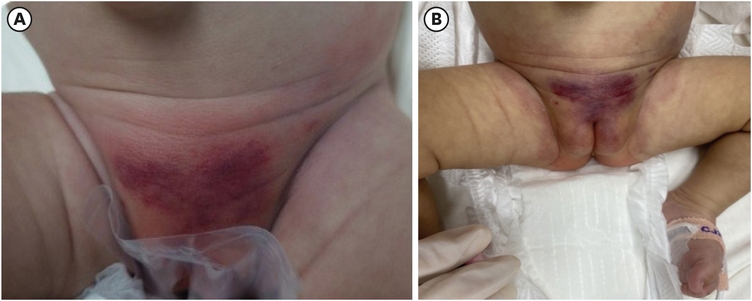
Fig. 1
Rapid progression of necrotizing fasciitis from suprapubic to flank area. (A) Discoloration at mons pubis. (B) Four hours after the photo in (A) was taken. The discoloration spread rapidly to the flank area.
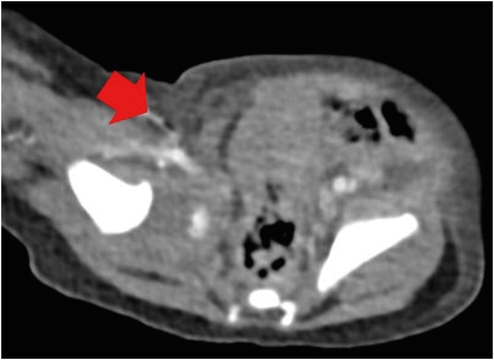
Fig. 2
Abdominal computed tomography; air bubbles in the subcutaneous tissue of the right groin and proximal inner thigh (arrow).
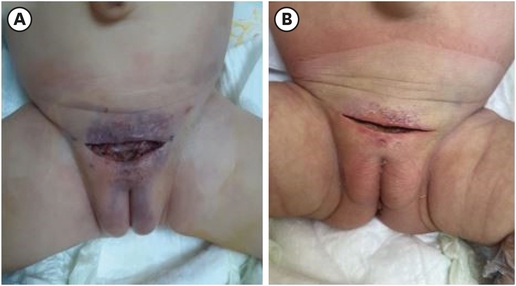
Fig. 3
The surgical wound was left open and irrigated with normal saline. The surgical wound (A) immediately after surgery and (B) three days after the operation. The discolored areas were gradually recovering.
Wound irrigation with normal saline and the application of gauze soaking dressing were performed three times a day until delayed wound closure. The wound was closed using nylon 3-0 and 5-0 sutures on post-operation day 7.
S. agalactiae was cultured from the cerebrospinal fluid (CSF) and blood, thus targeted antibiotics (cefotaxime, ampicillin/sulbactam) were administered for approximately two weeks until negative cultures were obtained from the CSF and blood. One year after the surgery, the baby is now healthy and growing normally.
This study was approved by the Medical Research Ethics Review Committee of Keimyung University Dongsan Medical Center (2022-08-052), and the need for informed consent was waived owing to the retrospective nature of the study. No personally identifiable information is included.
Fournier’s gangrene was named by Jean Alfred Fournier in 1883 [5]. It is rarer in children than in adults. Underlying conditions, including diabetes mellitus; an immunosuppressive state, such as human immunodeficiency virus infection; chronic steroid therapy; malnutrition; and a low socio-economic status are predisposing factors for the disease [2]. Disease severity increases with age in adults. Early diagnosis and surgical debridement with antibiotics are essential for the treatment of Fournier’s gangrene. Despite advances in medical technology, mortality remains high, averaging 20%–30% [6].
Low birth weight, preterm labor, trauma, circumcision, burns, systemic infections, and immunocompromised states are predisposing factors in children [4]. In our case, the patient had a systemic infection of S. agalactiae, found in the peripheral blood stream and CSF. She was also born preterm and needed NICU care. Moreover, she had been treated for neonatal sepsis. These are thought to be risk factors contributing to Fournier’s gangrene.
Complement (C3, C4, CH50) and gene testing (next generation sequencing-based gene panel test) were performed to investigate the possibility of a hidden immunocompromised state as a contributing factor to Fournier’s gangrene. For this test, we paid attention to the IL10RA receptor mutation. IL10RA receptor mutations are associated with inflammatory bowel disease, immunosuppression, and, in severe cases, sepsis in children [7]. The test revealed no genetic mutation in the patient.
Rapid diagnosis and prompt treatment reduce disease progression and toxicity. In our case, the clinical symptoms improved dramatically after surgery; the skin color change, which had spread to the flank area, improved noticeably immediately after the surgery, and the fever also subsided. Recent studies have shown that, in some cases, initially using selective surgical treatment (only debridement of confirmed necrotic tissue) is better than immediate extensive radical resection [8, 9]. We also extensively discussed the extents of the incision before the surgery. An incision was made only at the suprapubic area where the skin color change was most severe, that is, where necrotizing fasciitis had progressed the most. No additional extensive incisions were added. If the clinical course worsened after surgery, extensive incisions would have been considered in the second operation.
Ameh et al. [9] reported on 12 neonates and infants who were treated for Fournier’s gangrene, and there was no mortality. The prognosis of Fournier’s gangrene is better in children than in adults [10]. This may be because it is easier to control risk factors in children than in adults [9].
Although rare in infants, Fournier’s gangrene can still occur and might have a better prognosis with prompt surgical intervention and medical antibiotic treatment. In our experience, the diagnosis was difficult, and there were many concerns in deciding surgical treatment. Characteristic clinical features were very important in diagnosing Fournier’s gangrene, and the assistance of an expert radiologist was also crucial. We envisage that this case report will be helpful to clinicians treating patients with similar conditions.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.E.J., L.H.J.
Data curation: K.J.
Formal analysis: K.J., K.E.J.
Investigation: K.J.
Methodology: K.E.J.
Project administration: K.E.J.
Resources: K.J.
Software: K.J., K.E.J.
Supervision: L.H.J.
Validation: K.E.J.
Visualization: K.J., L.H.J.
Writing - original draft: K.J.
Writing - review & editing: K.E.J.
The authors thank the registered nurses Yun Ji-hee, Lee Seul-gi, and Lee Su-bin for their devoted help in caring for the patients at the Pediatric Surgery Department.
