

Purpose
The
objective
of this study, conducted at a single center, was to determine the appropriate subgroup of pediatric appendicitis patients for nonoperative management (NOM) and evaluate the effectiveness of this approach. Furthermore, the study aimed to identify the factors that influence the likelihood of treatment failure.
Methods
Out of the 37 children diagnosed with acute appendicitis who underwent NOM, 31 patients successfully completed the treatment without the need for appendectomy. However, 6 patients experienced recurrence of symptoms and subsequently required appendectomy.
Results
The two groups of patients who experienced successful NOM and those who required appendectomy did not exhibit significant differences in terms of baseline characteristics, laboratory findings, or antibiotic treatment. Furthermore, factors such as the presence of appendicolith or perforation did not demonstrate a significant association with treatment failure. Additionally, the multivariable logistic regression analysis did not identify any predictors of recurrence.
Conclusion
The study emphasizes the viability of NOM even in cases of complicated appendicitis, especially in the era of coronavirus disease 2019 limiting the chance of surgical treatment. It has shown potential in reducing the risk of complications that may arise from early surgical intervention in high-risk patients.
The objective of this study, conducted at a single center, was to determine the appropriate subgroup of pediatric appendicitis patients for nonoperative management (NOM) and evaluate the effectiveness of this approach. Furthermore, the study aimed to identify the factors that influence the likelihood of treatment failure.
Out of the 37 children diagnosed with acute appendicitis who underwent NOM, 31 patients successfully completed the treatment without the need for appendectomy. However, 6 patients experienced recurrence of symptoms and subsequently required appendectomy.
The two groups of patients who experienced successful NOM and those who required appendectomy did not exhibit significant differences in terms of baseline characteristics, laboratory findings, or antibiotic treatment. Furthermore, factors such as the presence of appendicolith or perforation did not demonstrate a significant association with treatment failure. Additionally, the multivariable logistic regression analysis did not identify any predictors of recurrence.
The study emphasizes the viability of NOM even in cases of complicated appendicitis, especially in the era of coronavirus disease 2019 limiting the chance of surgical treatment. It has shown potential in reducing the risk of complications that may arise from early surgical intervention in high-risk patients.
Acute appendicitis is widely acknowledged as the most common reason for surgery in both adults and children. In South Korea, the overall occurrence of appendicitis was found to be 22.71 per 10,000 individuals annually, with a total of 13.56 appendectomies performed per 10,000 individuals each year [1]. In the textbook of pediatric surgery by Holcomb et al., both surgical removal of the appendix (appendectomy) and nonoperative management (NOM) are presented as viable treatment options for nonperforated appendicitis [2].
Compared to initial appendectomy, NOM resulted in fewer complications, less pain, and shorter hospital stays. This is particularly applicable to patients who exhibit severe inflammation of the cecum and distal ileum, as they are at a higher risk of stump leak following standard appendectomy. However, a meta-analysis indicated a 1-year failure rate of 20%–30%, requiring readmission or subsequent surgery [3, 4, 5, 6]. In pediatric population, the success rate of NOM has been reported to range from 75%–80%, with a meta-analysis study reporting as high as 97% effectiveness [7, 8, 9]. This approach has gained recognition as a safe and effective method for treating pediatric patients.
Since the onset of the coronavirus disease-2019 (COVID-19) outbreak, the necessity of a negative pressure operating room for patients with fever symptoms, such as those undergoing appendectomy, resulted in several limitations in their surgical procedures. Consequently, meeting the surgical demands for appendicitis at the same level as before became challenging for many hospitals. A recent meta-analysis unveiled an average decrease of 20.9% in adult appendectomy cases, while there was a notable increase of 13.4% in children [10]. In this situation, there has been a growing interest in exploring NOM as a treatment option for patients with acute appendicitis. In this context, a number of patients, both adults and children, received antibiotic treatment as an alternative approach.
As of now, there are no established guidelines or principles determining which patients should undergo medical management for acute appendicitis. Due to the lack of consensus on the specific patient population that would benefit from medical treatment, the decision to pursue medical management was often left to the discretion of individual centers based on their respective experiences.
Therefore, in this study, we aimed to investigate the appropriate subgroup of pediatric appendicitis patients for medical treatment. Also, we tried to analyze the effectiveness of this approach and identify factors associated with treatment failure.
During the period from March 25, 2021, to February 28, 2022, the medical records of all patients under 18 years old diagnosed with acute appendicitis and got medical treatment were reviewed retrospectively. This study was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No.: 2023-0136)
Flow of NOM was detailed described in Fig. 1. The diagnosis of acute appendicitis was confirmed radiologically using computed tomography (CT) and/or ultrasonography (US). Laboratory test was conducted including inflammatory markers. To assess the severity of appendicitis, several parameters were used, including the Alvarado score, neutrophil to lymphocyte (NL) ratio, appendix diameter, the presence of appendicolith, and CT grade. The CT grade was divided into four stages based on imaging findings, ranging from simple inflammation of the appendix to the presence of a periappendiceal abscess. This classification system allowed for a more precise categorization of the severity and extent of the appendicitis based on the CT scan results. We developed our own grade to CT findings (Grade 1: appendicitis limited to inflammation in the appedix only; Grade 2: appendicitis with periappendiceal infiltration; Grade 3: appendicitis with periappendiceal abscess; Grade 4: appendicitis with perforation). These parameters were utilized to evaluate and categorize the severity of the appendicitis.

Fig. 1
Flow of medical management of acute appendicitis.
US, ultrasonography; CT, computed tomography; CRP, C-reactive protein.
The choice of initial antibiotics was determined based on the severity of appendicitis. Depending on the severity, antibiotics such as 3rd-generation cephalosporin, piperacillin/tazobactam, or meropenem were selected as the initial treatment option. The decision on which antibiotic to administer was made in accordance with the severity assessment of the appendicitis case. Initial antibiotics of choice was 3rd generation cephalosporine. Whenever perforation of the appendix was suspected, metronidazole was added. In cases of periappendiceal abscess, piperacillin/tazobactam was selected as initial antibiotics. The escalation/de-escalation of antibiotics was determined according to changes in vital signs and follow-up laboratory results done by every 2–3 days. For periappendiceal abscess, percutaneous drainage was conducted. Follow-up US was performed based on worsening clinical course during hospitalization (persistent fever, elevated C-reactive protein [CRP], continued abdominal pain, etc.) or if there was a huge abscess evident at the time of hospitalization, percutaneous catheter drainage (PCD) insertion was considered. All patients were discharged when serum level of CRP reached to below 1 mg/mL.
The follow-up for patients was conducted on an outpatient basis. US was used for determination of resolution and recurrence of appendicitis. Two follow visit takes about 2.5 months. Typically, the first follow-up visit was conducted 2 weeks after discharge, and the patient visited the outpatient clinic for the second time 2 months later with US and CRP. When no recurrence was observed during two follow-up visits, follow-up was discontinued.
The criteria used to define treatment failure included the recurrence of symptoms, which resulted in readmission to the emergency room. In cases where recurrence occurred, laparoscopic appendectomy was performed. If an appendicolith was initially detected during the ultrasound examination and remained present during outpatient follow-up, an interval appendectomy was scheduled to take place 8 weeks later. For interval appendectomy in patients with appendicolith, appendicolith was identified in 14 patients during the initial work up. Recurrence occurred in 4 patients and all of them got appendectomy. For rest 10 patients did not show recurrence and we didn’t do appendectomy to them. It was because they were our initial patients. This is because these were the initial patients in our study. Recent patients underwent interval appendectomy after 8 weeks but were not included in this study.
Categorical variables were compared using Pearson chi-square testing, while continuous variables were reported as means ± standard deviations and compared using 2-tailed unpaired t-tests. Statistical significance was determined at a p-value of less than 0.05. Data management and analysis were conducted using IBM® SPSS® software, version 21 (IBM Corp., Armonk, NY, USA).
During the study period, a total of 37 patients underwent NOM, with 31 patients successfully completing the treatment and 6 patients experiencing treatment failure. In the case of these 6 patients who had recurrence of symptoms, all of them required readmission through the emergency room and subsequently underwent laparoscopic appendectomy.
In Table 1, the baseline characteristics of the patients who received NOM are presented. The age range of the patients was between 4 and 16 years, with 23 boys and 14 girls included in the study. The most common symptom observed at the time of admission was right lower quadrant tenderness. A significant difference in the Alvarado score was observed in the group that experienced treatment failure (p=0.003). However, there were no significant differences between the successful NOM group and the failed NOM group in terms of the initial white blood cell count, NL ratio, and serum CRP level measured upon admission to the emergency room.
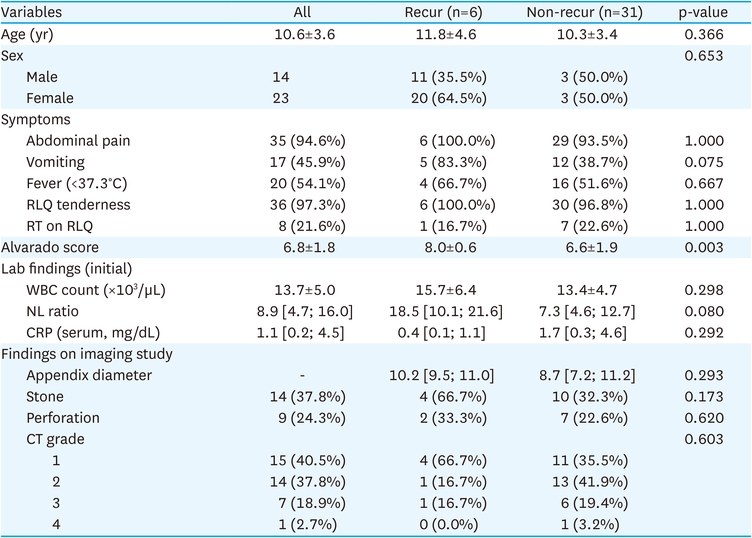
Table 1
Characteristics of patients who got non-operative treatment for acute appendicitis (n=37)
Among the patients who received NOM, appendicolith was found in 14 patients in imaging diagnosis. Out of these 14 patients, 10 were successful with NOM, while 4 experienced treatment failure. Perforation was confirmed in a total of 9 patients, with 7 succeeding with NOM and 2 experiencing treatment failure. However, there was no statistically significant association found between the presence of perforation or appendicolith and treatment failure.
The antibiotic usage and duration in patients who received NOM are presented in Table 2. Among the patients, 13 (35.1%) received 3rd generation cephalosporin initially, 21 (56.8%) received Piperacillin/tazobactam, and 3 (8.1%) received Meropenem. Antibiotic escalation was required in 29.6% of the patients. The duration of intravenous antibiotic use did not show a statistically significant difference between the recurrence and non-recurrence groups, with 7.5 days and 6.0 days, respectively.
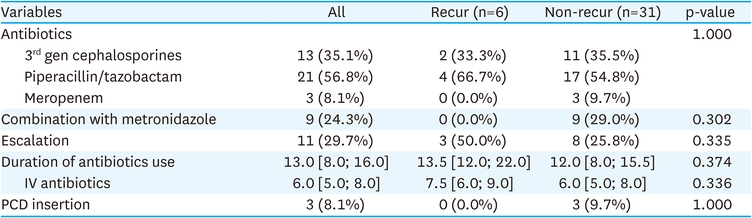
Table 2
Summary on medical treatment on acute appendicitis
There were no significant differences observed in terms of hospital stays, highest serum CRP levels, or days until CRP normalization between the two groups. The recurrence-free period in the recurrence group was found to be 76 days (Table 3). No surgical complication was reported related with interval appendectomy. Multivariable logistic regression analysis was performed to identify factors that may influence the recurrence of appendicitis. However, no specific factor was found to be significantly associated with recurrence. The analysis did not reveal any specific variables that could reliably predict the occurrence of recurrence after medical treatment for appendicitis.

Table 3
Treatment outcome
Traditionally, appendectomy has been established as the standard treatment for acute appendicitis. However, recent studies have provided evidence supporting the effectiveness of NOM as an alternative approach [11]. While laparoscopic appendectomy is generally considered a safe and straightforward surgical procedure, it requires general anesthesia and is associated with complications in approximately 10% of cases [12]. Also, complication rates tend to be higher in complicated cases, and delayed appendectomy has been preferred as a safer approach [13]. In contrast, several studies have reported that the presence of an appendicolith increases the risk of recurrence in cases of appendicitis [14, 15, 16].
In our study, we achieved a successful NOM rate of 83.7%. It was safely applied even in cases of complicated appendicitis, such as those with the presence of appendicolith or perforation, as there was no significant increase in recurrence rates. This suggests that NOM can be a potential alternative to early surgical intervention. Taking this into consideration, it may be deemed a safer approach to initially attempt NOM rather than opting for early surgery, particularly in patients in situations where emergency surgery is not available.
While individual factors such as the presence or absence of appendicolith and perforation may not have shown a significant relationship with recurrence in our study, the Alvarado score, the comprehensive indicator of severity, was higher in recurrence group (Table 1). This suggests this traditional factor used to assess appendicitis severity could serve as potential predictors in determining the outcome of NOM. By considering these established indicators, clinicians can better evaluate the likelihood of recurrence and make informed decisions regarding the implementation of NOM.
This study revealed several limitations. First, it is a single-center study that included pediatric patients admitted under the care of a few surgeons. This may introduce a potential bias and limit the generalizability of the findings to a broader population. Also, the sample size was relatively small, and the observation period was relatively short. Therefore, the results may not fully capture the long-term outcomes and recurrence rates associated with NOM in pediatric appendicitis. Second limitation was that there was no direct comparison between operative and non-operative management. However, through enough literatures and comparison with the results of existing non-operative treatments, we sought to demonstrate the feasibility of non-surgical treatment not only for simple appendicitis but also for complicated appendicitis in situations where surgical access is limited [3, 4, 5, 6, 7, 8, 9]. However, at the time of conducting this study, most operators at our center chose non-surgical treatment, so biases such as learning curve and single port vs. multiport approach were expected during the comparative study. In that, we decided to forgo direct comparison.
To address these limitations and improve the generalizability of the findings, future studies should aim for larger sample sizes, involve multiple centers, and consider longer follow-up periods. A prospective study excluding bias would be essential. This would provide a more comprehensive understanding of the effectiveness and outcomes of NOM in pediatric appendicitis.
Another limitation of the study is the lack of investigation into the medical costs and disability days in comparison to surgical cases. Research focusing on these aspects would provide valuable insights into the economic implications and quality of life for patients and caregivers. Considering that the duration of treatment, including disability days, can influence the decision-making process of caregivers regarding treatment methods, it would be beneficial to include this factor in future studies. This would contribute to a more comprehensive understanding of the overall impact and outcomes associated with NOM in pediatric appendicitis.
In conclusion, NOM can be considered as a feasible treatment option for management of acute appendicitis, especially in the era of COVID-19 limiting the chance of surgical treatment. It has shown potential in reducing the risk of complications that may arise from early surgical intervention in high-risk patients. However, it is important to individualize the decision-making process by severity of appendicitis, such as Alvarado score. Close monitoring of the patient's response to NOM is crucial, and if there are signs of clinical deterioration or worsening infection, various measures can be considered such as escalation of antibiotics or PCD insertion.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: K.H.J., K.D.Y.
Data curation: K.H.J.
Formal analysis: K.H.J., G.S.
Methodology: G.S.
Project administration: K.D.Y.
Software: K.H.J., G.S.
Supervision: K.D.Y.
Validation: K.D.Y.
Visualization: K.H.J., G.S.
Writing - original draft: K.H.J.
Writing - review & editing: K.D.Y.
