

Purpose
Although total parenteral nutrition (TPN) is essential for patients with intestinal failure, intensive monitoring and management are required to provide sufficient nutrition and prevent complications. The adverse effects of prolonged TPN >5 years were evaluated in pediatric patients, and preventative methods and treatments were analyzed.
Methods
Pediatric surgery patients at a single center who had received parenteral nutrition (PN) for more than 5 years at a single center were analyzed retrospectively. Adverse effects and treatments were determined by review of their medical records. Complications were defined as catheter-related, metabolic, or nutritional.
Results
Seven patients receiving long-term PN had short bowel syndrome (SBS), including two each with necrotizing enterocolitis, congenital atresia, and pseudo-obstruction, and one with Hirschsprung’s disease. Six patients had a mean 6.4 ± 4.4 line infections (median: 6, range: 3–15). Central venous catheters were replaced a mean 7.3 ± 4.5 times (median: 8.5, range: 1–12). None of these patients had bilirubin concentrations above 2 mg/mL, and none experienced acute or chronic kidney injuries. Six children received vitamin D supplements, and one experienced rickets. Laboratory tests revealed a temporary lack of zinc or selenium, but no associated clinical symptoms. None had a vitamin B12 or folate deficiency. All seven patients were hospitalized for electrolyte imbalance a median 2.5 times (range: 1–17); all recovered with hydration and TPN. At the time of this writing, all seven patients remained alive, with below-average growth, and two were treated with growth hormones.
Conclusion
Appropriate catheter insertion, guardian education and management, as well as active responses to complications, are important-required to safely maintain long-term parenteral nutrition.
Although total parenteral nutrition (TPN) is essential for patients with intestinal failure, intensive monitoring and management are required to provide sufficient nutrition and prevent complications. The adverse effects of prolonged TPN >5 years were evaluated in pediatric patients, and preventative methods and treatments were analyzed.
Pediatric surgery patients at a single center who had received parenteral nutrition (PN) for more than 5 years at a single center were analyzed retrospectively. Adverse effects and treatments were determined by review of their medical records. Complications were defined as catheter-related, metabolic, or nutritional.
Seven patients receiving long-term PN had short bowel syndrome (SBS), including two each with necrotizing enterocolitis, congenital atresia, and pseudo-obstruction, and one with Hirschsprung’s disease. Six patients had a mean 6.4 ± 4.4 line infections (median: 6, range: 3–15). Central venous catheters were replaced a mean 7.3 ± 4.5 times (median: 8.5, range: 1–12). None of these patients had bilirubin concentrations above 2 mg/mL, and none experienced acute or chronic kidney injuries. Six children received vitamin D supplements, and one experienced rickets. Laboratory tests revealed a temporary lack of zinc or selenium, but no associated clinical symptoms. None had a vitamin B12 or folate deficiency. All seven patients were hospitalized for electrolyte imbalance a median 2.5 times (range: 1–17); all recovered with hydration and TPN. At the time of this writing, all seven patients remained alive, with below-average growth, and two were treated with growth hormones.
Appropriate catheter insertion, guardian education and management, as well as active responses to complications, are important-required to safely maintain long-term parenteral nutrition.
Total parenteral nutrition (TPN) to treat infants with intestinal failure was first initiated in 1967 [1], with the use of parenteral nutrition (PN) for pediatric patients and premature infants increasing over the past 30 years [1, 2]. Greater experience with PN has resulted in the identification of many complications, enhancing the understanding of energy metabolism and allowing for implementation of safer PN methods. TPN is indicated if complete or partial loss of intestinal function prevents enteral nutrition for more than 1 week or if enteral nutrition is insufficient for less than 1 week. Despite surgery reducing the numbers of patients receiving PN, its incidence in premature infants, especially those with low birthweight of less than 1,500 g, has increased significantly due to increases in the incidence of impaired gastrointestinal function [2]. Despite the advantages of PN, it has been associated with various side effects, including mechanical, metabolic, infectious, and hepatic biliary tract complications, making it important to monitor patients receiving PN [3].
Understanding the disease characteristics of patients who are prescribed PN, preparing for possible complications, and tailoring nutrition are essential for patient management. The present study therefore evaluated the incidence of complications in patients receiving prolonged PN, as well as methods that may be employed to prevent and treat these complications.
The medical records of 14 patients receiving home TPN and seven who had received TPN for more than 5 years at the Asan Medical Center, Seoul, South Korea, were retrospectively reviewed. Factors recorded included patient age and sex, and the duration of TPN. Complications analyzed included central vein catheter-associated complications (e.g., infection, thrombus, mechanical, number of replacements, and number of intact vessels), metabolic complications (e.g., liver, biliary, and renal infections) and nutritional complications (e.g., those associated with trace elements and vitamins). Patients administered TPN for <5 years and those lost to follow-up were excluded.
Home PN teams from Asan Medical Center provide TPN throughout Seoul and surrounding areas, allowing for daily visits and evaluations.
At each visit, the home PN team examined the patients, including measurements of weight. Basic blood tests, including complete blood cell (CBC) counts, blood chemistry, and concentrations of phosphorus, electrolytes, blood urea nitrogen (BUN), magnesium, C-reactive protein (CRP), and triglycerides, were measured once per week and a trace element test once a month. Concentrations of 25-OH-vitamin D3, prealbumin, total iron binding capacity (TIBC), and ferritin, as well as the trace elements copper, zinc, and magnesium, were measured once per month.
Tailored PN suitable for individual children up to age 6 years is produced by and supplied to our center. Use of tailored PN can prevent hyperphosphatemia or electrolyte imbalances associated with continuous application of commercial PN. Children aged >6 years are administered commercial TPN. Infants are administered TPN one to five times per week, with crystalloid fluid (dextrose 5%/Na/K-2 or dextrose 5%/Na/K-3) administered on weekends. Additionally, a short bowel clinic for children receiving PN was opened and evaluated once every 2 months, providing treatment for individual children with home care.
Catheter infection was defined as bacteremia originating from an intravenous catheter [4]. It is not related to infection at other sites within 48 hours of a central line placement. Clinical manifestations are important. Fever and chills are the most common symptom. Patients may experience pain, redness, or discharge surrounding the exit site of the tunneled catheter or along the line. Catheter infection was diagnosed based on the results of a physical examination and laboratory tests, with blood culture being the most important step. Leukocytosis and elevated CRP may be other indicators of central venous infection [4]. If central venous infection was suspected, samples from the central venous tube and from the periphery cultures were cultured separately [5].
The most common method of diagnosing catheter-related bloodstream infection (CRBSI) was central venous catheter culture. Briefly, a 5 cm piece was cut from the end of the central venous tube and rolled onto the medium. CRBSI could also be diagnosed without removing the central venous catheter by quantitative paired blood cultures. Because the central venous tube in CRBSI is the primary infectious lesion, the volume of blood culture from the central vein was higher than that from the peripheral blood culture. CRBSI was diagnosed when bacteria were more abundant in central venous than in peripheral blood cultures by more than a certain ratio [6]. Patients who did not experience improvements in the symptoms or signs of infection with antimicrobial treatment alone, but showed improvement within 24–48 hours after removal of the central venous catheter, were suspected of having central catheter-related infection [4].
Categorical data were reported as percentages and frequencies, and compared using two-tailed Fisher’s exact tests or χ2 tests, as appropriate. Continuous data were reported as means ± standard deviations (SD) and compared using Student’s t-tests. All statistical analyses were performed using SPSS 21.0 statistical software (IBM Corp., Armonk, NY, USA), with statistical significance defined as a p-value <0.05.
The seven children who experienced complications of PN included four boys and three girls. Their median age of PN initiation was 2 years (range: 0.8–6 years) and their median TPN duration was 97 months (range: 68–117 months). The demographic characteristics of these patients are presented in Table 1. At present, their mean age is 11 years and none has died. Evaluation of diseases requiring TPN showed that two patients each had necrotizing enterocolitis (NEC), congenital intestinal obstruction, and chronic pseudo-obstruction, and one had Hirschsprung’s disease (Table 1). All seven patients were able to take some foods by mouth, consuming a minimum of 100 mL of balanced amino acid nutrition, such as “Monowell,” and as much porridge or rice as desired. In addition, two children had gastrostomy, requiring enteral feeding.
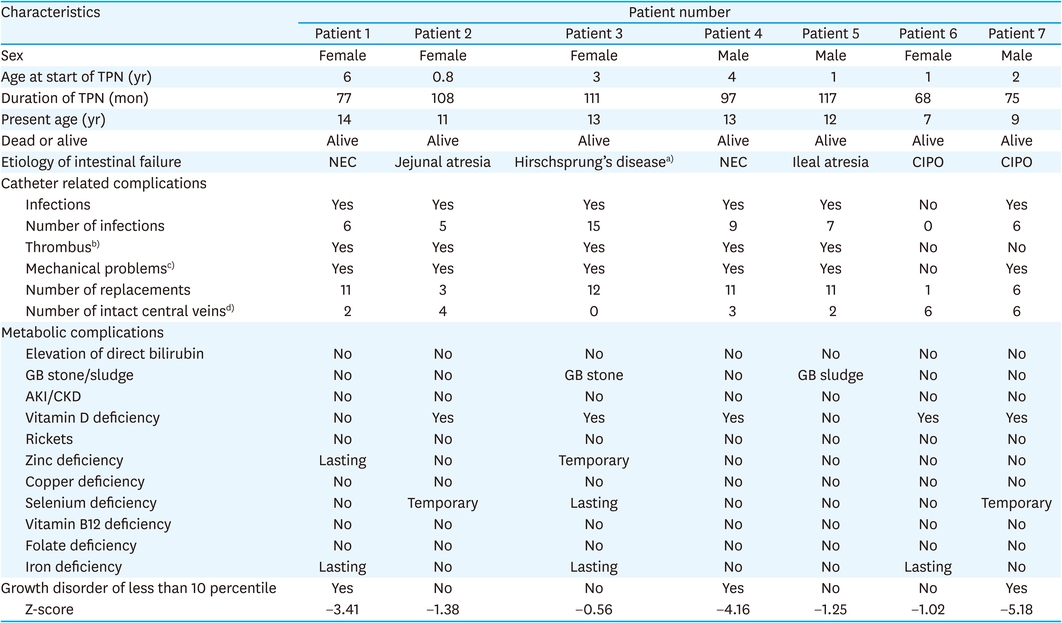
Table 1
Clinical characteristics of patients receiving TPN for more than 5 years
Six of the seven patients experienced central catheter infections. The median number of infections per patient was six (range: 0–15). Five patients had thrombus and six had mechanical problems, such as tearing or loss of function of the central catheter. The median number of central venous catheter replacements was 11 (range: 1–12). Of the six central veins (i.e., the two internal jugular, subclavian, and femoral veins), three per patient (range: 0–6) were found to be intact (Table 1).
Other diseases that increase bilirubin, none of the patients experienced hyperbilirubinemia for more than 2 weeks, although some experienced temporary increases in bilirubin. However, two patients had gallstone and gallbladder sludge, with one undergoing a laparoscopic cholecystectomy. None showed a temporary or permanent reduction in glomerular filtration rate (GFR). Of the seven included patients, five received vitamin D supplementation. No cases of rickets were observed (Table 1).
One patient lacked zinc and recovered, whereas one received supplementation. Two patients had temporary selenium deficiency, with one still receiving treatment to replenish normal levels. None of these seven patients had vitamin B or folate deficiency, whereas three had iron deficiency anemia (Table 1).
Six patients (85.7%) were hospitalized a median of two times (range: 0–17) for dehydration and electrolyte imbalance. Most of these hospitalized patients had gastroenteritis, which was treated with a fluid-containing TPN with correcting electrolytes for dehydration.
Four of the seven children were in the 10th percentile for growth, and all seven were in the 50th percentile for height and weight. However, height and weight slope were almost the same as the average for children of the same age (Fig. 1).
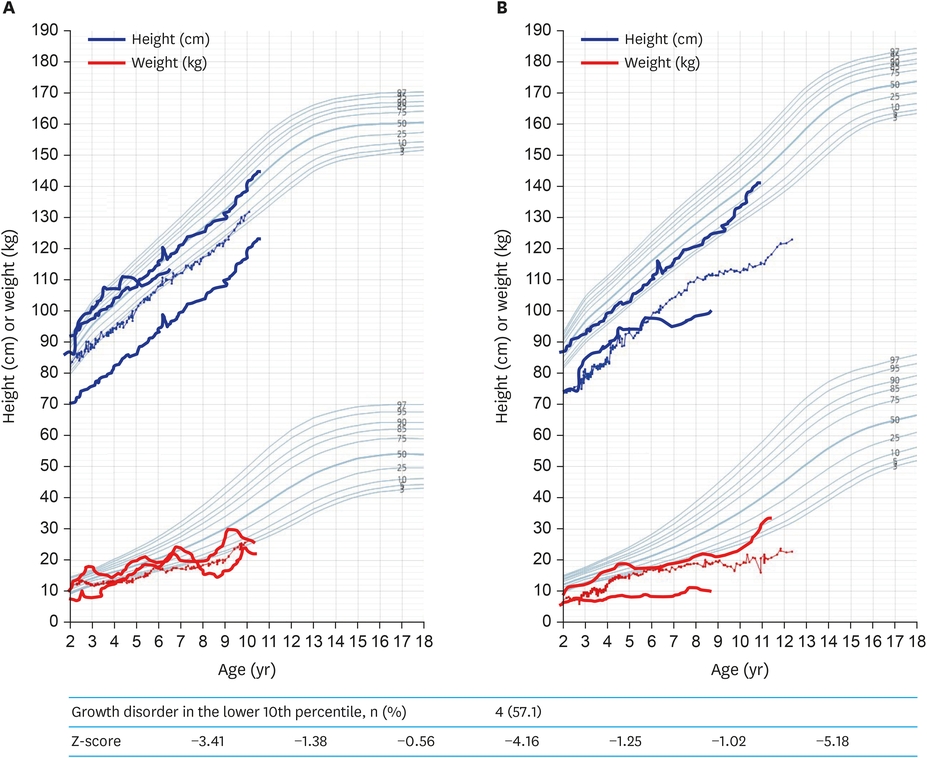
Fig. 1
Growth curves of patients receiving long-term PN. All seven patients were in the 50th percentile for height and weight, whereas four patients were in the 10th percentile for growth. Development curve of (A) girls and (B) boys aged 2–18 year.
PN, parenteral nutrition.
PN is primarily used to treat intestinal failure or insufficient nutrition [1]. Adverse events associated with PN can include mechanical, metabolic, and renal and hepatic biliary tract complications, as well as infections, making regular monitoring paramount. The most common indication for surgery in children requiring PN is intestinal obstruction, resulting from gastrointestinal deformities or congenital causes, with other indications including ileus, necrotizing enteritis, and intestinal failure [3].
Sepsis has been observed at least once in children who undergo surgery and receive PN, with approximately 30% developing sepsis after culture of blood bacteria [7]. In this study, central catheter infections occurred in six of the seven children, mostly between 2011 and 2012, but only once since 2019. Six of these children were infected with a cluster of Gram-positive cocci (85.7%), but other species were also present, including Enterococcus, Streptococcus, Leuconostoc sup, and Candida.
Patients were infected a median six times (range: 0–15). In addition, six patients experienced some mechanical problems such as tearing or loss of function of the central catheter and thrombus of the catheter. Thus, one of the seven patients did not have any intact central veins. The maximal number of central venous catheter replacements was 12. These findings indicate the importance of proper management and proper protocols for central vein catheter placement. Because fever was suggestive of a central line-associated bloodstream infection (CLABSI), central line and peripheral cultures were performed immediately after patients developed a fever, followed by treatment primarily with intravenous vancomycin for 10 to 14 days. Antibiotics were administered to the infected central catheter, TPN was halted, and fluids were supplied through the peripheral vein. The central venous catheter was maintained if the fever subsided within 72 hours of antibiotic use; however, if fever persisted or the patient developed septic shock or repeat infection, ultrasound was performed to check for thrombus in the central veins, followed by removal of the catheter [7, 8]. CLABSI can also be prevented by using 2% chlorhexidine before the procedure or during the dressing, with the wound being dressed with transparent polyurethane film (OPSITE ◊ Flexifix; Smith & Nephew, London, UK and 3M™ Tegaderm™; 3M, Saint Paul, MN, USA), which is replaced every seven days [7, 8]. Catheter infections can be prevented with sufficient care, so diligent monitoring is required.
Parenteral nutrition-associated cholestasis (PNAC) is the most common biliary complication in children with PN and is diagnosed by excluding other bilirubin-increasing conditions (e.g., inborn error of metabolism, biliary atresia, choledochal cyst) [9]. None of the patients in the present study experienced hyperbilirubinemia for more than 2 weeks, although several showed a temporary increase in bilirubin. Two of these patients, however, had gallstones and gallbladder sludge, with one undergoing laparoscopic cholecystectomy. This complication was first reported in 1971 [10], with data suggesting that younger age increased the risk for more serious biliary stasis and more frequent occurrence of fatty liver in adults than PNAC. Adverse effects of PN can include liver hypertrophy, liver function decline [11] (increased serum ammonia, elevated AST, and ALT), jaundice (elevated total bilirubin and direct bilirubin), fatty liver, liver fibrosis, bile duct proliferation, and cirrhosis. Increases in direct bilirubin are indicative of adverse events, whereas transaminase concentrations do not increase markedly, even after 2 weeks of biliary congestion [3, 12]. Premature infants and newborns are most at risk of developing bile congestion due to the toxic effects of certain amino acids in venous fluids or endotoxins (especially infections with gram-negative organisms such as Escherichia coli) [13], which are related to the fat content of PN supplements [14]. Therefore, many hospitals use preventative treatments, such as 10% fish oil fat preparations, preparations of long-chain triglycerides (LCT) and medium-chain triglycerides (MCT), or soybean, MCT, olive, and fish triglycerides [15]. To prevent PNAC, patients in our center are administered fish oil fat preparations, whereas PN is discontinued in patients who develop PNAC. Blood glucose trends are monitored to adjust the amount of PN administered per day and the number of PN treatments per week.
Patients receiving TPN can experience reduced GFR, with patients who experience intestinal failure on long-term PN being at risk of nephrolithiasis [16, 17, 18]. Although the etiology of this decline is unknown, reduced GFR has been associated with patient age, nephrotoxic drug use, and previous bloodstream infections [17]. None of the children in the present study experienced a temporary or permanent reduction in GFR. TPN-induced nephropathy may be prevented by close monitoring and routine determinations of renal function in patients receiving home PN.
Dehydration can be caused by insufficient hydration or excessive use of diuretics, loss of intestinal fluid through diarrhea or vomiting, or fever [19]. Dehydration is accompanied by reduced urine production; orthostatic hypotension; increased serum Na, BUN, and hemoglobin concentrations; decreased skin elasticity; complaints of thirst; and rapid weight loss. Preventative measures can include ensuring sufficient fluid intake to compensate for insensible fluid and intestinal loss. Additionally, weight and electrolytes should be monitored daily at the beginning of treatment [19]. If there is a stoma, we define as high output stoma in case of the drainage of stoma exceeding 40 mL per kg. The amounts of stoma with 40 mL/kg − 20 mL/kg is divided and replaced per hour. But, the max fluid should not exceed 150%.
Monthly laboratory tests and subsequent supplementation, if appropriate, are required to prevent trace element deficiency. Trace elements in PN include zinc, copper, manganese, and chromium; in Korea, 10 mL of the PN brand Furman® contains 220 mg zinc sulfate, 39.3 mg cupric sulfate, 15.4 mg manganese sulfate, and 0.51 mg chromium sulfate. Copper and manganese are excreted through bile, so they should not be administered to patients with biliary stasis. Selenium, chromium, and molybdenum should not be administered to patients with renal dysfunction [20, 21]. Selenium and carnitine are administered to patients who have fasted for more than 30 days. Trace elements in our center are assayed once per month by the nutrition intensive support team (NST) and the short bowel clinic team, allowing intensive administration of any the missing nutrients. Selenium can be administered both orally and intravenously, with patients administered 1 to 20 mL of 3 µg/kg selenium one to three times per week.
Fatal vitamin deficiency can occur in patients receiving TPN without vitamin supply for as little as a few weeks. Although complex intravenous vitamin preparations are commonly used in Korea, patients should also receive supplementation with vitamins not included in these preparations, such as vitamin K, B12, biotin, folate, niacin, and pantothenic acid, all of which are usually included in preparations in the United States. At present, there are no intravenous vitamin preparations for premature babies [20]. Vitamin preparations available for children and adults over age 11 years, which contain propylene glycol and polysorbate additives, should not be administered to infants due to concerns over toxicity. Due to the limited transfer of fat-soluble vitamins through the placenta, premature infants have low body storage of fat-soluble vitamins, therefore requiring a sufficient supply of vitamins from birth [20].
Bone demineralization can occur when premature or newborn infants receive PN over a long period, resulting in osteomalacia, osteoporosis, and rickets [22, 23]. The causes of occurrence are complex, including changes in vitamin D metabolism [23], aluminum toxicity, protein calcium loss, drugs (diuretics), inactivity, and lack of calcium, phosphorus, and vitamin D. However, the metabolism of vitamin D varies among patients, with some developing rickets despite a sufficient supply of vitamins [22, 24]. These complications may be prevented by administering sufficient amounts of vitamin D (400 IU/day), calcium (0.5–2.5 mEq/kg), and phosphorus (1–2 mM/kg), particularly when supplying aluminum. Infants with a serious vitamin D deficiency and those with suspected rickets despite supplementation should be administered vitamin D and calcium supplements, in cooperation with pediatric endocrinologists. Moreover, X-rays should be taken at least once every 6 months to monitor bone. At our center, patients are administered 400 to 1,000 IU/day of oral vitamin D or 100 to 300,000 IU/week intramuscular vitamin D.
Iron is not uniformly added to venous nutrition and is not included in commercially available trace element formulations. Thus, prolonged treatment with PN risks iron deficiency and requires supplementation [20]. Excess iron, however, can accumulate in hepatocytes and Kupffer cells, affect immune function, and increase the risk of infection by pathogens that require iron [25]. Although most side effects are mild and occur spontaneously, caution should be exercised in administering iron dextran, as it can occasionally cause anaphylaxis [26, 27]. By contrast, iron sucrose preparations are relatively safe, as the frequency of severe adverse events is much lower, and only minor adverse events, such as vomiting, abdominal pain, diarrhea, and temporary hypotension, have been reported to date in children [27]. The addition of iron preparations to TPN for at least 3 weeks is recommended, at doses of 50–100 μg/kg per day in infants and children, and 200 μg/kg per day in premature infants [28]. Although our center prefers to administer iron orally, iron can also be administered intravenously once per week.
Of the seven patients included in the present study, four were in the 10th percentile for growth, and all were below the 50th percentile in height and weight. Despite their being similar to the mean for small-for-gestational age infants, catch-up growth was considered necessary. In our hospital, growth hormone is tested in patients with growth disorder, defined as <10th percentile. In the present study, two children were injected with growth hormones at the endocrine clinic, whereas hormone concentrations were not tested in the other five. The oldest of the seven patients was aged 14 years, whereas most of these patients were preschool children. Therefore, they had not undergone proper testing for growth hormone. These children may subsequently require treatment with growth hormone.
Although TPN provides nutritional support via a multidisciplinary approach, complex complications such as sepsis and biliary congestion can occur. Analyses of these complications may provide clues to preventative measures and treatments. Monitoring is crucial in children receiving TPN, especially in the early stages of PN. Patients should be monitored for possible complications by determining their clinical status, analyzing test results, and evaluating their characteristics and conditions.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: N.J.M.
Data curation: H.S.
Formal analysis: H.S., N.J.M.
Investigation: H.S.
Methodology: N.J.M.
Project administration: K.H., N.J.M.
Resources: K.H.
Software: N.J.M.
Supervision: N.J.M.
Visualization: H.S.
Writing - original draft: K.H.
Writing - review & editing: H.S.
