

Approximately 5% of Wilms tumors are bilateral. Multidisciplinary care including surgery, chemotherapy, and radiation has greatly improved the survival rates. With long-term survivorship, treatment should be planned to ensure quality survival. Nephron-sparing surgery (NSS) is now a recommended alternative to bilateral nephrectomy with renal replacement therapy in bilateral Wilms tumors. However, the feasibility of bilateral NSS is dependent on multiple factors like the size, location of the tumor, and response to chemotherapy. In advanced bilateral tumors, a) prolonging preoperative chemotherapy to achieve optimum response for performing a salvageable renal surgery and b) administering chemotherapy in between the staged nephrectomies, is an effective strategy. Response assessment with imaging will help in a) selection of appropriate surgery, b) timing and c) sequencing of surgery. We present a patient with bilateral Wilms tumor managed with neoadjuvant chemotherapy followed by staged bilateral NSS followed by adjuvant chemotherapy at our institute. The patient is alive with a follow-up of 5 years.
Approximately 5% of Wilms tumors are bilateral. Multidisciplinary care including surgery, chemotherapy, and radiation has greatly improved the survival rates. With long-term survivorship, treatment should be planned to ensure quality survival. Nephron-sparing surgery (NSS) is now a recommended alternative to bilateral nephrectomy with renal replacement therapy in bilateral Wilms tumors. However, the feasibility of bilateral NSS is dependent on multiple factors like the size, location of the tumor, and response to chemotherapy. In advanced bilateral tumors, a) prolonging preoperative chemotherapy to achieve optimum response for performing a salvageable renal surgery and b) administering chemotherapy in between the staged nephrectomies, is an effective strategy. Response assessment with imaging will help in a) selection of appropriate surgery, b) timing and c) sequencing of surgery. We present a patient with bilateral Wilms tumor managed with neoadjuvant chemotherapy followed by staged bilateral NSS followed by adjuvant chemotherapy at our institute. The patient is alive with a follow-up of 5 years.
Bilateral tumors account for 5%–7% of all nephroblastoma patients [1]. The goal of treatment in bilateral Wilms tumors is oncological control and preserving as much renal parenchyma as possible to prevent end-stage renal disease. Renal failure develops in 15% of stage V Wilms tumor patients treated, by the age of 20 years [2]. Bilateral nephron-sparing surgery (NSS) is a very good option to preserve adequate renal parenchyma. Both Clinical Oncology Group (COG) and the International Society of Pediatric Oncology (SIOP) recommend surgery after 6 weeks in patients with good response. If the response is felt inadequate to perform NSS, extended chemotherapy should be offered. These protocols have led to improved outcomes [3]. Bilateral Wilms tumor poses challenges to treating surgeons concerning the timing of surgery, which kidney to be operated upon first, a requirement of meticulous dissection to achieve tumor-free margin and preserve sufficient normal renal parenchyma.
We present a patient with metastatic bilateral Wilms tumor managed with Neoadjuvant Chemotherapy and bilateral NSS at our institute.
A 2-year-old boy presented with progressive abdominal distension of a 1-month duration. Examination revealed a firm mass of 10×10 cm in the left loin and a 5×5 cm mass in the right loin. Contrast-enhanced computed tomography (CECT) showed an 18 cm × 10.2 cm × 9.6 cm heterogeneously enhancing mass in the upper pole of the left kidney with renal vein thrombosis. The right kidney had a similar lesion of 7 cm × 6 cm × 5 cm in the lower pole. There were three space-occupying lesions in the liver. Multiple metastatic nodules were present in both the lung fields (7 in the right lung and 6 in the left lung). Biopsy from the left renal mass was suggestive of Wilms tumor.
Since the patient had bilateral Wilms tumor with metastasis he was managed according to SIOP 2001 protocol for stage IV disease.
The patient received neoadjuvant chemotherapy for 6 weeks with vincristine, actinomycin D, and doxorubicin. Vincristine was given at 1.5 mg/m2 weekly for 6 doses, actinomycin D at 45 μg/kg once in 2 weeks for 3 doses, and doxorubicin was given at a dose of 50 mg/m2 on week 1 and week 5. Reassessment CECT at 6 weeks, showed partial response with a decrease in the size of renal masses, the disappearance of the liver lesion and decrease in size, number of lung lesions (3 on each side). The response however was not adequate to perform a bilateral NSS. Hence, the patient was continued on the same chemotherapy for another 5 weeks with similar doses as mentioned (total of 11 weeks).
On TC-99m DTPA scan, the Glomerular filtration rate (GFR) was 55 mL/min for the right kidney and 38.6 ml/min for the left kidney (Fig. 1A). CECT showed a 10.7 cm × 8 cm × 7.2 cm heterogeneously enhancing mass in the upper pole of the left kidney with renal vein thrombosis and a 4.7 cm × 4.2 cm × 4 cm mass in the lower pole of the right kidney. A staged bilateral NSS was planned with the less affected kidney operated upon first. The patient underwent open right NSS using the non-clamping technique. Histopathology revealed Wilms tumor with resected margin and all the lymph nodes being free of tumor. The tumor was composed of blastemal and rhabdoid elements with a 25% tumor response. Based on histology he was stratified as having a high-risk tumor and was started on chemotherapy for high-risk tumors starting 2 weeks after surgery to increase the feasibility of performing NSS on the left side. Two combinations of drugs were used: Etoposide (150 mg/m2) and carboplatin (200 mg/m2), and cyclophosphamide (450 mg/m2) combined with doxorubicin (50 mg/m2). The patient received 2 cycles of chemotherapy with Adriamycin (day 1)/cyclophosphamide (days 1-3) on week 1 and then etoposide/carboplatin on week 4 (days 1-3). CECT done showed a good response in the left kidney with no focal space-occupying lesions in the liver. Both lung fields showed tiny subpleural opacities measuring less than 5 mm (3 in the right lung, 2 in the left lung). On Tc-99m DTPA scan GFR was 20.7 mL/min for the right kidney and 57.1 mL/min for the left kidney (Fig. 1B). He underwent open left NSS using the non-clamping technique. There was a thrombus in the upper polar vein extending into the main left renal vein and was not adherent to the vessel wall. Only the renal vein was clamped after tumor mobilization and before approaching the renal vein thrombus. The extraction of the thrombus with the vascular repair was done. The patient had an uneventful recovery.
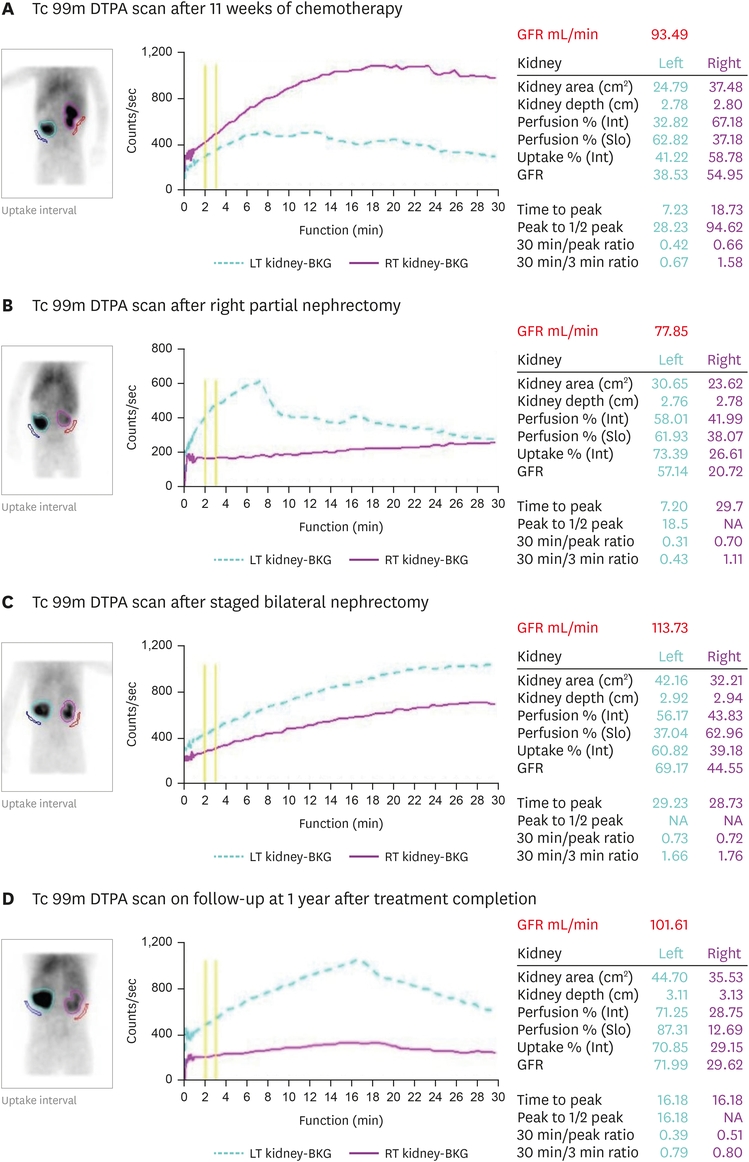
Fig. 1
Tc 99m DTPA scan results of the patient during the course of treatment.
Histopathology revealed Wilms tumor. The surgical margins, hilar and paraaortic nodes were free of tumor and the tumor response was 30%. He received whole lung radiation of 12 Gy in 8# with 6 Mv X-ray beam therapy and then was continued remaining postoperative chemotherapy with adriamycin, cyclophosphamide on weeks 1, 13, and 25, and etoposide, carboplatin on weeks 4, 7, 10, 16, 19, 22, 28 (total 34 weeks of postoperative chemotherapy). Radiation to the abdomen was not offered as the parents were unwilling for it, even after explaining the implications of avoiding it.
The patient was regularly followed up using renal function tests, ultrasound imaging of kidneys, and chest X-ray. Tc 99m DTPA scan was done 2 times in this interim postoperative period and the kidney function was stable (Fig. 1C and D). He has now a disease-free survival of 5 years. His latest renal function tests show urea of 21 mg/dL and creatinine of 0.6 mg/dL.
Survival from bilateral Wilms now approaches 73% with proper management, including surgery, chemotherapy, and radiation [4]. The SIOP current bilateral Wilms tumor management protocol includes neoadjuvant chemotherapy consisting of Vincristine, Dactinomycin, and Doxorubicin given for 6 weeks followed by reassessment for the feasibility of NSS, if it is deemed that adequate renal parenchyma cannot be preserved, chemotherapy for an additional 6 weeks is administered. It is advised to continue chemotherapy as long as the tumors show signs of regression and up to the time of NSS if deemed possible. Surgery is generally done at week 12. A recently completed multi-institutional COG study (AREN0534) has standardized the approach to neoadjuvant therapy and timing of surgical resection, resulting in good results in bilateral Wilms tumor [5]. On reassessment at six weeks, it was felt surgery would entail bilateral nephrectomy with the need for permanent renal replacement therapy. It is recommended to wait for 2 years on renal replacement therapy after bilateral nephrectomy before contemplating for transplantation. However, in our country, the logistics for regular dialysis and the very long waiting time for acquiring a donor’s kidney deterred us from considering early surgery and additional chemotherapy was given for a total of 11 weeks.
Surgery maintains an important role in the treatment of Wilms Tumor [6]. Different surgical approaches can be used for bilateral Wilms tumors. Simultaneous or a staged approach, decision of which kidney to be operated first, type of surgery (radical vs. NSS) depends on the size of the tumor, position, and the response of the tumor to neoadjuvant therapy [7, 8].
In this patient, the left-sided tumor was large with a tumor thrombus, with a high chance of radical nephrectomy. The right side was amenable for NSS but there was doubt if the residual renal function alone would be adequate to sustain life. The decision was therefore taken to perform NSS on the right renal tumor first and assess the residual renal function with a Tc-99m DTPA scan. If the residual renal function was inadequate, logistics for dialysis after surgery for the left side could be arranged electively and if the residual right renal function was adequate, the surgery for the left side could proceed routinely. Chemotherapy was administered between surgery for the right and left renal tumors to a) decrease the left renal tumor further and b) buy sufficient time for residual right renal function to stabilize. The left renal tumor decreased further during this interim chemotherapy and became amenable for NSS. We used an off-clamping technique to prevent damage to the kidneys as proven in other studies [9].
It was reported that satisfactory renal function after renal salvage surgery can be achieved if 30% of the renal volume can be saved. The incidence of renal failure in bilateral Wilms tumors was reported as 16.4% by the National Wilms tumor study group (NWTS) 1, 9.9% by NWTS-3, and 3.8% by NWTS-4 [10]. This progressive improvement was the result of improvement in chemotherapy regimens, the adoption of neoadjuvant chemotherapy, and renal preservation surgeries.
In advanced bilateral Wilms tumor, to achieve optimal outcomes a) additional preoperative chemotherapy should be considered to bring the patient in the purview of bilateral NSS, b) Staged bilateral partial NSS is an effective and safe option, timing and sequencing should be personalized c) Multimodality treatment should be individualized achieve optimal outcomes.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: R.A.
Data curation: R.K.M.
Formal analysis: R.A., M.K.
Investigation: R.K.M.
Supervision: R.V., R.A.
Writing - original draft: R.K.M.
Writing - review & editing: R.A., M.K., R.V.
