

Posterior reversible encephalopathy syndrome (PRES) is a distinctive neurological disorder characterized by specific clinical and radiological features. While its etiology is multifaceted, the vasogenic theory provides a comprehensive framework for understanding its pathogenesis. Notably, PRES has been observed in cancer patients undergoing cytotoxic chemotherapy, immunotherapy, and select neurosurgical interventions. In this context, we present an unprecedented case involving a 7-year-old girl who developed PRES subsequent to abdominal surgery for adrenal neuroblastoma, a scenario hitherto unreported in medical literature. The patient’s medical history encompasses a diagnosis of stage IV neuroblastoma - high risk. Her treatment course comprised six cycles of neoadjuvant chemotherapy, followed by an open right adrenalectomy coupled with retroperitoneal lymph node dissection. Following surgery, the patient’s clinical profile evolved to encompass the classic symptoms of PRES, including headache, blurred vision, and elevated blood pressure. Neuro-imaging confirmed the diagnosis, with subsequent robust clinical recovery achieved by day 12. Continuation of adjuvant therapy in accordance with established protocols was pursued. Successful management of PRES pivots on several crucial principles: timely recognition, meticulous hydration, vigilant blood pressure control, and attentive intensive care. By adhering to these tenets, complete clinical recuperation can be realized, sparing patients enduring neurological deficits or vision impairment. This case underscores the importance of remaining vigilant for PRES in postoperative settings, particularly in pediatric patients undergoing surgical interventions for malignancies. Further studies and vigilance are warranted to expand our understanding of this intriguing condition and optimize therapeutic strategies.
Posterior reversible encephalopathy syndrome (PRES) is a distinctive neurological disorder characterized by specific clinical and radiological features. While its etiology is multifaceted, the vasogenic theory provides a comprehensive framework for understanding its pathogenesis. Notably, PRES has been observed in cancer patients undergoing cytotoxic chemotherapy, immunotherapy, and select neurosurgical interventions. In this context, we present an unprecedented case involving a 7-year-old girl who developed PRES subsequent to abdominal surgery for adrenal neuroblastoma, a scenario hitherto unreported in medical literature. The patient’s medical history encompasses a diagnosis of stage IV neuroblastoma - high risk. Her treatment course comprised six cycles of neoadjuvant chemotherapy, followed by an open right adrenalectomy coupled with retroperitoneal lymph node dissection. Following surgery, the patient’s clinical profile evolved to encompass the classic symptoms of PRES, including headache, blurred vision, and elevated blood pressure. Neuro-imaging confirmed the diagnosis, with subsequent robust clinical recovery achieved by day 12. Continuation of adjuvant therapy in accordance with established protocols was pursued. Successful management of PRES pivots on several crucial principles: timely recognition, meticulous hydration, vigilant blood pressure control, and attentive intensive care. By adhering to these tenets, complete clinical recuperation can be realized, sparing patients enduring neurological deficits or vision impairment. This case underscores the importance of remaining vigilant for PRES in postoperative settings, particularly in pediatric patients undergoing surgical interventions for malignancies. Further studies and vigilance are warranted to expand our understanding of this intriguing condition and optimize therapeutic strategies.
Posterior reversible encephalopathy syndrome (PRES) is a complex neurological disorder characterized by a range of signs and symptoms, along with distinct neuroimaging findings reflecting vasogenic edema involving the cortical grey matter and subcortical white matter of the bilateral parietal to occipital regions [1]. While the etiology of this syndrome is multifactorial, it has been most commonly associated with conditions such as hypertensive encephalopathy and eclampsia, wherein vasogenic edema is a prominent feature. Additionally, chemotherapy and immunosuppressive drugs have been proposed as potential triggers, particularly in cancer patients [2]. Despite these known associations, our report presents an unprecedented case of PRES occurring subsequent to surgery for adrenal neuroblastoma in a seven-year-old girl, a scenario not previously documented in literature.
A seven-year-old girl presented with a year-long history of dull aching abdominal pain. Although her clinical examination was largely unremarkable, a contrast-enhanced computed tomography (CT) scan revealed a 4.6×4.3 cm right suprarenal mass, raising suspicion of neuroblastoma. She defaulted for further evaluation and treatment due to the severe acute respiratory syndrome coronavirus (SARS-COVID-19) pandemic. She returned two years later with persistent abdominal pain, at which point an 18-fluorodeoxyglucose positron emission tomography CT scan revealed of a mildly enhancing irregular large abdominopelvic, soft tissue mass measuring 12.4×15.2×25 cm with enlarged retroperitoneal and iliac nodes. The mass encased the abdominal vascular structures with the narrowing of both renal vessels (SUVmax - 3.99). Increased marrow activity was seen in the axial and appendicular skeleton (SUVmax - 2.51).
Image-guided core needle biopsy revealed a malignant round cell tumor with immuno histochemistry study positive for synaptophysin, neurofilament, CD56; negative for CD99, desmin, keratin, and leukocyte common antigen with a Ki67 value of 90%, suggestive of neuroblastoma, undifferentiated type with low mitotic karyorrhectic index (<2%). Fluorescence in situ hybridization was positive for N-MYC gene amplification. Bone marrow biopsy was suggestive of marrow involvement by malignant round cells. Diagnosis of stage IV Neuroblastoma - high risk was confirmed, and she was treated as per Children’s Cancer Group (CCG) 3891 protocol [3]. She received six cycles of neoadjuvant chemotherapy. Post-chemotherapy imaging revealed a partial response of the primary with residual retroperitoneal nodes (Fig. 1). She underwent open right adrenalectomy with retroperitoneal lymph node dissection (RPLND). Histopathology was reported as Neuroblastoma with treatment effect - viable tumor being 30%. The resected margins were free of tumors, RPLND - 10 of 10 lymph nodes had metastatic Neuroblastoma with extranodal extension.
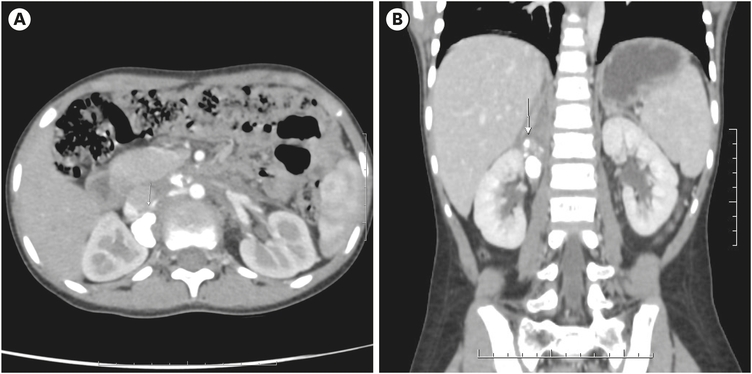
Fig. 1
Preoperative contrast enhanced computed tomography of the abdomen: images showing a large right suprarenal tumour with extensive calcification, marked by arrow head. (A) Axial, (B) coronal.
On the postoperative day (POD) 2, the patient had multiple spikes of fever with leukopenia. Antibiotics were escalated. On POD 6, the patient had a headache and blurring of vision with elevated blood pressure (134/110 mmHg). Tab Amlodipine, 2.5 mg stat, was administered. Due to persistent high blood pressure recordings, inj. Labetalol infusion was started. On POD 7, magnetic resonance imaging (MRI) revealed T2/ FLAIR hyperintensity in bilateral parieto-occipital lobes with restricted diffusion and minimal heterogeneous leptomeningeal enhancement (Fig. 2). The clinical and radiological features were representative of PRES. The patient was treated with intravenous fluids, antibiotics, anti-hypertensive drugs, and supportive care in the pediatric Intensive care unit. There was a gradual clinical improvement with decreased headache and improved vision on POD 9. Labetalol infusion was stopped on POD 10, and adequate blood pressure control was obtained with Tab. Amlodipine 2.5 mg per day. The patient’s vision had improved, and she was discharged on POD 12.
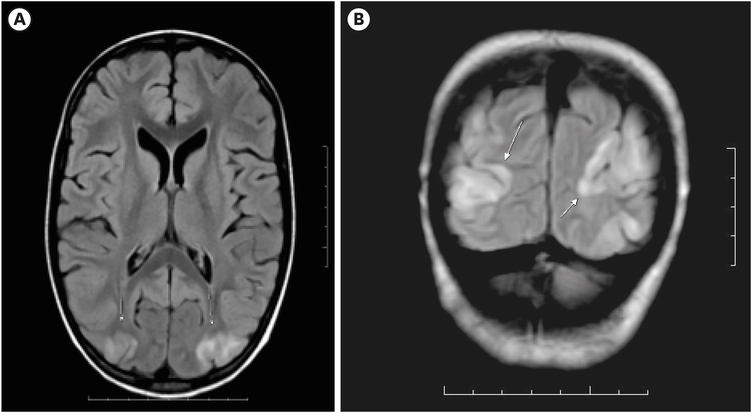
Fig. 2
Magnetic resonance imaging brain showing features characteristic of posterior reversible encephalopathy syndrome. (A) Axial and (B) coronal views. Bilateral symmetrical parieto-occipital white matter hyperintensities (indicated by arrow mark in B).
On follow-up after two weeks, an ophthalmology evaluation was done. The patient had an improvement of vision to 6/6, and the fundus examination was normal. Tab. Amlodipine was stopped after one month. Neurological imaging was not repeated to confirm resolution, as the patient had a complete clinical recovery. The patient continues to be on adjuvant therapy per protocol.
PRES is an acute neurological condition initially described in 1996 by Hinchey et al. [4]. Although often associated with elevated systemic blood pressure, this is not always the case. PRES can present with symptoms such as headaches, visual disturbances, altered consciousness, and seizures, if not promptly recognized and treated, it can progress to coma and even result in death. In cases where early identification and aggressive intervention are implemented, clinical recovery tends to precede radiological improvement, which might take several weeks.
The brain's vasculature has a remarkable ability to maintain steady blood flow even when systemic blood pressure fluctuates, owing to various regulatory mechanisms. However, when the mean arterial pressure surpasses the range of 150–160 mmHg, or higher in chronic hypertensive individuals [5], this equilibrium is disrupted. According to the vasogenic theory [6], rapid and uncontrolled hypertension triggers dysregulation in cerebral blood flow, leading to the breakdown of the blood-brain barrier. This breakdown causes proteins and fluids to leak into the interstitial space, ultimately resulting in edema. The relatively diminished sympathetic innervation in the vertebrobasilar circulation could explain the selective involvement of the posterior regions, as commonly observed in PRES cases. This theory gains further support from the rapid recovery, both clinically and radiologically, achieved through the prompt normalization of blood pressure.
An alternative perspective suggests that a systemic inflammatory state causing endothelial dysfunction might underlie PRES [7]. This theory is particularly relevant as PRES is frequently associated with systemic inflammatory conditions such as eclampsia, chronic renal disease, transplantation, autoimmune disorders, cancer chemotherapy, and sepsis. Angiography studies have demonstrated reversible focal and diffuse abnormalities consistent with endothelial dysfunction. Acute hypertension induces cerebral vasoconstriction, potentially leading to hypoxia and subsequent vasogenic edema. Restoring normal systemic blood pressure alleviates vasoconstriction, facilitating recovery, as observed in PRES cases [7].
The clinical manifestations of PRES are diverse [2]. Visual disturbances can range from mild blurriness to more severe conditions like homonymous hemianopia or cortical blindness. Altered mental states encompass a spectrum from slight confusion and agitation to coma. Additional symptoms can include nausea, vomiting, and brainstem deficits, with seizures being a common occurrence, either focal or generalized. In a study by Fugate et al. [6], seizures (70%) and hypertension (60%) were the most prevalent symptoms, followed by encephalopathy, headache, and visual disturbances.
MRI reveals distinct features, primarily characterized by bilaterally symmetrical parieto-occipital white matter hyperintensities. Some cases may show atypical features such as hemorrhage and restricted diffusion [1]. While the parieto-occipital lobes are most frequently affected, other areas like the frontal lobes, cerebellum, and temporal lobes can also be involved. In some instances, atypical regions such as the basal ganglia, brainstem, and thalamus may be affected [1].
Effectively managing PRES necessitates early recognition and aggressive supportive care. The patients must be monitored in an intensive care setting, with appropriate measures based on the etiology [8]. Treatment strategies include,
1. Addressing underlying triggers
2. Correcting dehydration and electrolyte imbalances
3. Ensuring airway management for patients with altered consciousness
4. Gradual reduction of blood pressure, avoiding rapid fluctuations.
5. Considering haemodialysis or delivery, if the cause is renal or pregnancy-induced.
6. Managing seizures with appropriate anti-epileptic medication
In cancer patients, chemotherapy and immunosuppressive drugs have been proposed as potential etiological factors. Hematological malignancies, especially in children, have a higher incidence of PRES. Notably, the use of bevacizumab, either alone or in combination with other treatments, has been linked to PRES [2].
PRES has been reported in neuroblastoma following the administration of anti-GD2 Monoclonal antibody immunotherapy [9] and vascular endothelial growth factor receptor inhibitor lenvatinib [10]. In the context of surgery, PRES has been documented primarily in neurosurgical procedures, such as resection of posterior fossa tumors [11] and ventriculoperitoneal shunting for fourth ventricle ependymoma [12]. To the best of our knowledge, this report presents the first documented instance of PRES triggered by abdominal surgery for a solid organ malignancy, specifically in a pediatric patient with adrenal Neuroblastoma.
PRES can be triggered by a range of underlying conditions. Timely identification and proactive management involving intensive care, anti-hypertensive agents, anti-epileptic medications, and adequate hydration can mitigate severe consequences and facilitate a return to the patients’ baseline health. Although the prognosis is generally optimistic, some individuals with more severe presentations might experience lasting neurological deficits. Despite growing awareness and reporting, PRES remains enigmatic. Future research endeavors are imperative to unravel the complexities of this potentially devastating yet manageable disorder.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: R.V., R.A.
Data curation: M.A.
Formal analysis: M.A., R.A.
Investigation: T.K.B.
Methodology: M.A., T.K.B.
Project administration: R.A.
Resources: R.V., R.A.
Software: M.A.
Supervision: R.V., R.A.
Validation: T.K.B.
Visualization: M.A.
Writing - original draft: M.A., T.K.B.
Writing - review & editing: R.V., R.A.
