

Entomophthoromycosis is a rare fungal infection, infecting the immune competent children, in the tropical and sub-tropical areas. It is caused by Basidiobolus ranarum, which belongs to the order Entomophthoral. The diagnosis is delayed, as it presents with non-specific symptoms. The disease occurs following a trivial injury or insect bites and therefore presents as subcutaneous nodules over the trunk, buttock and thighs. Gastrointestinal (GI) infection and invasive spread are very rare. Very few cases of GI disease and liver entomophthoromycosis have been reported in the English literature. The diagnosis is confirmed on histopathology and fungal cultures. We discuss a case of liver entomophthoromycosis in a 3-year-old child, who presented with non-specific symptoms and palpable lump in the epigastric region. The child was worked up for malignancy and underwent left hepatectomy. Later, the histopathology report revealed entomophthoromycosis. Delay in diagnosis can be fatal. Entomophthoromycosis is an emerging fungal infection and should be an important differential in patients presenting with vague symptoms and lump abdomen.
Entomophthoromycosis is a rare fungal infection, infecting the immune competent children, in the tropical and sub-tropical areas. It is caused by Basidiobolus ranarum, which belongs to the order Entomophthoral. The diagnosis is delayed, as it presents with non-specific symptoms. The disease occurs following a trivial injury or insect bites and therefore presents as subcutaneous nodules over the trunk, buttock and thighs. Gastrointestinal (GI) infection and invasive spread are very rare. Very few cases of GI disease and liver entomophthoromycosis have been reported in the English literature. The diagnosis is confirmed on histopathology and fungal cultures. We discuss a case of liver entomophthoromycosis in a 3-year-old child, who presented with non-specific symptoms and palpable lump in the epigastric region. The child was worked up for malignancy and underwent left hepatectomy. Later, the histopathology report revealed entomophthoromycosis. Delay in diagnosis can be fatal. Entomophthoromycosis is an emerging fungal infection and should be an important differential in patients presenting with vague symptoms and lump abdomen.
Entomophthoromycosis is a rare fungal infection reported from tropical and subtropical areas. It belongs to class Zygomycetes, which is subdivided into order Entomophthorales (Genus Basidiobolus and Conidiobolus) and order Mucorales (Genus Mucor and Rhizopus). Interestingly both orders infect humans; however, the clinical features of entomophthoromycosis infections are diametrically opposite when compared with those of Mucorales [1, 2].
The common clinical presentation includes subcutaneous nodules but rarely can cause systemic infection involving the lung, liver, and the gastrointestinal (GI) tract. It usually affects the immune-competent hosts and manifests with non-specific symptoms [3]. This disease affects all age groups with more predisposition to children less than 10 years of age [1]. Gastrointestinal basidiobolomycosis (GIB) is overlooked and presents with delayed diagnosis, especially in patients with normally functioning immune systems [4]. Most children are extensively investigated for malignancy or tuberculosis before reaching this diagnosis. The outcome of visceral GIB can be fatal if not diagnosed and treated promptly. We report the management and outcome of a case of entomophthoromycosis of the liver in a 3-year-old child.
A 3-year-old male child presented with a high-grade fever associated with chills and rigors for the past 8 months. The fever was associated with abdominal pain and distension for the past 3 months. There was no history suggestive of night sweats, weight loss, loss of appetite, malaise, shortness of breath, chest pain, cough with bloody sputum, or jaundice. He was initially referred from the Department of Pediatric Haemato-oncology, where he was being worked up for liver malignancy. On examination, the child was pale but moderately built and nourished. The child was active and hemodynamically stable. The abdomen was distended with a firm mass, 6×7 cm palpable in the left upper quadrant-umbilical and left hypochondrium regions. The mass was continuous with the liver dullness and was moving cephalo-caudally with respiration. There was no evidence of ascites or any other organomegaly. Laboratory values of hemoglobin 12 g/dL, total leucocyte count 21,500 with eosinophilia of 3,440 (neutrophils 57%, lymphocytes 26%, eosinophils 16% and monocytes 1%), platelets 5.2 lakhs, electrolytes (sodium 140 mEq/L, potassium 4.2 mEq/L and chloride 103 mEq/L), urea 23 mg/dL and urea 0.4 mg/dL and liver function tests, were within normal limits. The serum alpha-fetoprotein was 0.797, contrast-enhanced computed tomography (CECT) abdomen showed a large focal lesion of size 7.3×5.8×4.7 cm involving segments IVa, II, III with central necrosis (Fig. 1). There was no evidence of air or calcification. The arterial phase showed hypervascularity or centripetal enhancement enhancing the terminal part of the left hepatic vein. The left branch of the portal vein was attenuated in its proximal part and not visualized in the distal part. No satellite lesions were appreciated.
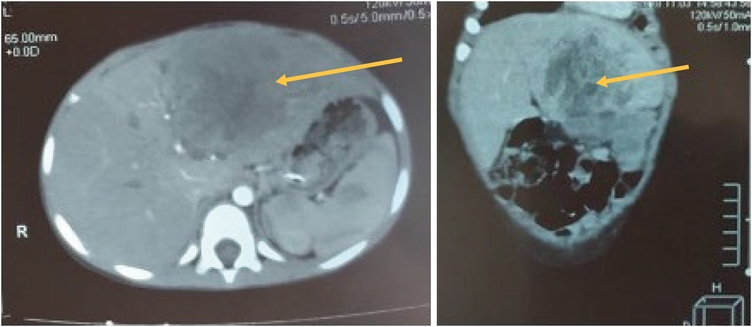
Fig. 1
Heterogenous liver mass in left lobe (yellow arrow).
Fine needle aspiration cytology (FNAC) done elsewhere was suggestive of fungal infection, and the trucut liver biopsy showed extensive lobular inflammation, necrosis, and nuclear debris with plasma cell infiltrates, with no evidence of tumor cells. Intra-sinusoidal fibrosis was seen with fibrin-rich thrombi in the hepatic veins suggestive of veno-occlusive disease. The child was planned for a left hepatectomy.
A large mass was noted in the left lobe of the liver in segments IVa, IVb, and III, 10×10 cm in size, hard in consistency, and irregular surface, with contiguous involvement of greater omentum (Fig. 2). Adhesions are present between the mass and the transverse colon. Inflow control was taken by portal dissection, and the left hepatic duct, left branch of the portal vein, and left branch of the hepatic artery was looped. A clear line of demarcation appeared extending from gallbladder fossa to left hepatic vein. The tumor with the left lobe of the liver has been excised in toto. The cut section showed a solid, grey-white, irregular tumor with bile staining and peripheral congested liver parenchyma (Fig. 3). The bowel and rest of the solid organs, appeared healthy. His postoperative course was uneventful, and he was discharged on postoperative day 12.
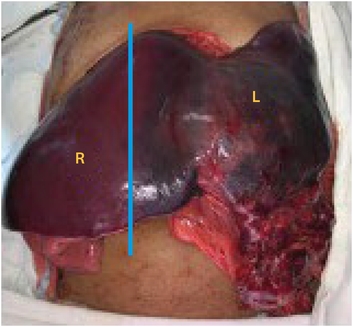
Fig. 2
Line of demarcation after vascular control (blue line).
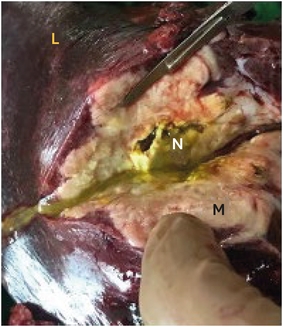
Fig. 3
Cut section of left lobe of liver.
L, liver tissue; N, necrotic material; M, fungal mass.
The histopathology revealed multiple suppurative large coalescing granulomas with broad aseptate periodic acid-Schiff-positive hyphae, surrounded by eosinophilic granular material (Splendore-Hoeppli phenomenon)—features suggestive of entomophthoromycosis, and the child was treated with long term amphotericin and voriconazole for 6 months. He had one episode of adhesive intestinal obstruction and was managed conservatively for the same. He is doing well at a 24-month follow up.
Entomophthoromycosis is a rare disease, seen in tropical and sub-tropical countries, caused by fungi belonging to the phylum Entomophthoral, which includes basidiobolomycosis and conidiobolomycosis [1, 5]. Unlike Mucor, they infect the immune-competent patients and do not usually cause angio-invasion. Conidiomycosis is an indolent infection of the face and presents as nasal discharge, nasal obstruction, or sinusitis [2]. Basidiomycosis, caused by B. ranarum, is a chronic subcutaneous infection of thigh, buttocks, or trunk. It resides in decaying plant material, and the leaves used as “toilet paper” are the usual source of infection. Traumatic implantation of the fungi or insect bites is the usual mode of transmission [6]. Painless erythematous indurated lesions are characteristic of basidiomycetes. Basidiomycosis has a male predisposition, with a male to female ratio of 3:1 [3]. Rarely, it can cause disseminated disease in both immune-compromised as well as immune-competent hosts. Transient immune suppression following surgery or viral infections may be the cause of invasive or disseminated disease [6]. Only 71 cases of GIB have been reported since 1964 [7]. Similar to Crohn’s disease, mural thickening, nodules, and ulcerations are seen in GIB [2]. Isolated liver involvement is very unusual and children are more prone than adults [8].
The disease presents with non-specific symptoms and can cause a diagnostic dilemma. Culture is the gold standard for diagnosis. It presents with abdominal pain, fever, vomiting, and sometimes constipation. Imaging studies usually reveal a mass either in the bowel or the liver. The mass has similar features as malignancy, Crohn’s disease, or tuberculosis. Leukocytosis marked eosinophilia, and elevated erythrocyte sedimentation rate and C-reactive protein are usually seen, also demonstrated in our case. The characteristic histopathological features are of chronic granulomas rich in eosinophils and the Splendore-Hoeppli phenomenon [1]. Most of the cases are diagnosed in post-operative histopathology reports. In the index case, there was suspicion of fungal infection on the FNAC, and the diagnosis was confirmed on the post-operative histopathological examination.
El-Shabrawi et al. [6] studied GIB in 14 adults and 12 children. All children in this study presented with fever, abdominal pain with mass, and eosinophilia. All the children had bowel involvement, and only 3 of them, between the age group of 3–7 years, also had a liver mass. They received surgical treatment like gastrectomy, resection and anastomosis of bowel or stoma, biliary and renal stenting, and itraconazole. The liver lesions were only biopsied and treated with anti-fungal agents. Five out of twelve patients have succumbed to the disease. Mortality can be as high as 20% [9]. Management of invasive visceral fungal infections like Mucor and basidiobolomycosis include aggressive surgical resection, which aids in decreasing the dosage of parenteral anti-fungal therapy.
Geramizadeh et al. [7] reviewed 14 cases of GIB and found that the most common complaint was abdominal pain. Interestingly, all were taken up for surgery suspecting lymphoma but were diagnosed post-operatively as entomophthoromycosis. One out of 14 had simultaneous bowel and liver involvement, and the liver biopsy was suggestive of eosinophilic granuloma. Out of 14, 9 were in the pediatric age group, supporting the fact that it is more common in the pediatric age group. All of them underwent surgical resection of the mass. They received anti-fungal therapy for 2 years period.
Geramizadeh et al. [10] reported the so-called first case of isolated liver entomophthoromycosis in a 2-year-old child. The clinical presentation was similar to our index case and had significant eosinophilia. The imaging was suggestive of a liver abscess and the patient was taken for surgery. Intra-operatively, there were multiple non-encapsulated liver masses, with ill-defined borders, without any other GI lesions. Excision of the mass with anti-fungal therapy was given for 6 months.
Entomophthoromycosis presents in immunocompetent individuals as a firm to hard mass with hepatomegaly, rapid increase in size, eosinophilia and Splendore-Hoeppli phenomenon on histopathology. Whereas the other liver fungal infections, which usually are seen in immunocompromised individuals, cavitating lesions filled with pus and necrosis, only fungal hyphae may be seen without eosinophilic granules, the most common organism being Candida species. On CECT, the lesion is hypoattenuating, involving one or more segments of the liver with inflammatory changes, necrosis and fat stranding. It is difficult to differentiate from other fungal lesions and tumours radiologically. Tissue confirmation is the gold standard [11].
The diagnosis of entomophthoromycosis is usually delayed due to the non-specific symptoms. Almost all cases of GIB reported have synchronous or metachronous involvement of the bowel and liver and have been initially misdiagnosed as malignancy or chronic inflammatory disease [12]. Abdominal mass with eosinophilia should raise the suspicion of basidiomycetes [13]. The management of this disease usually involves prolonged treatment with anti-fungal agents like itraconazole and surgical resection. Delay in the diagnosis can be fatal, and so surgical management becomes the cornerstone of the management algorithm in these patients, requiring major hepatic resection and prolonged anti-fungal treatment, to prevent a recurrence. It is a potentially curable disease and prolonged follow-up is required to monitor the rate of regression of the mass and response to treatment.
In conclusion, entomophthoromycosis is increasingly being seen in the pediatric age group, and yet poses a diagnostic challenge. Abdominal mass with eosinophilia is the clue to the diagnosis. Delay in diagnosis increases morbidity and mortality. It is a treatable condition and must be considered an important differential diagnosis in children presenting with non-specific abdominal symptoms, presenting with a liver mass.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: P.N.J.
Data curation: V.S., P.N.J.
Formal analysis: V.S., P.N.J., M.M.A., S.S.
Methodology: V.S., P.N.J.
Supervision: V.S., P.N.J., S.R., D.S.
Visualization: P.N.J., S.R., M.M.A.
Writing - original article: V.S., P.N.J.
