

Purpose
Intense multidisciplinary team effort is required for the intestinal rehabilitation of pediatric patients afflicted with intestinal failure (IF). These include enteral and parenteral nutrition (PN) support, monitoring of complications related to treatment, and considering further medical or surgical options for intestinal adaptation.
Methods
In the intestinal rehabilitation team (IRT) at our center, we have experienced 25 cases of pediatric IF requiring multidisciplinary intestinal rehabilitation. This study is a retrospective review of the collected medical records.
Results
Of the 25 subjects treated, 18 were boys and 7 were girls. At the time of referral to the IRT, the mean age was 1.6 years. Median follow-up was 42.9 months. The causes of IF were short bowel syndrome in 18 cases and motility-related in 7 cases. There are 24 patients alive at last follow-up: 12 patients have been weaned off PN, whereas 12 are still dependent on PN. Median time to weaning off PN was 4.8 months. There were 2 cases of IF-associated liver disease. Fifteen cases of central line associated blood stream infections occurred in 9 patients (0.82/1,000 PN days).
Conclusion
We report the results of multidisciplinary intestinal rehabilitation of pediatric IF patients in a Korean IRT. Further studies are required to improve survival and enteral tolerance of these patients.
Intense multidisciplinary team effort is required for the intestinal rehabilitation of pediatric patients afflicted with intestinal failure (IF). These include enteral and parenteral nutrition (PN) support, monitoring of complications related to treatment, and considering further medical or surgical options for intestinal adaptation.
In the intestinal rehabilitation team (IRT) at our center, we have experienced 25 cases of pediatric IF requiring multidisciplinary intestinal rehabilitation. This study is a retrospective review of the collected medical records.
Of the 25 subjects treated, 18 were boys and 7 were girls. At the time of referral to the IRT, the mean age was 1.6 years. Median follow-up was 42.9 months. The causes of IF were short bowel syndrome in 18 cases and motility-related in 7 cases. There are 24 patients alive at last follow-up: 12 patients have been weaned off PN, whereas 12 are still dependent on PN. Median time to weaning off PN was 4.8 months. There were 2 cases of IF-associated liver disease. Fifteen cases of central line associated blood stream infections occurred in 9 patients (0.82/1,000 PN days).
We report the results of multidisciplinary intestinal rehabilitation of pediatric IF patients in a Korean IRT. Further studies are required to improve survival and enteral tolerance of these patients.
Pediatric intestinal failure (IF) is a condition in which the function of the intestine is insufficient to sustain adequate growth and development [1]. With reduced intestinal function to absorb nutrients, fluids and electrolytes, patients require long-term supplementation with parenteral nutrition (PN). In children, IF is usually caused by extensive resection of the small intestine due to a variety of causes, including congenital malformations, thrombosis of the mesenteric vessels, or Crohn's disease [2, 3]. Previous studies have reported mortality rates of 15% to 47%, depending on the age, underlying disease, and duration of venous nutrition, and the economic and social burden due to long-term venous nutritional complications [4].
The goal of this study is to report the process and outcome of multidisciplinary intestinal rehabilitation of pediatric IF patients in a Korean intestinal rehabilitation team (IRT).
Retrospective review of medical records of all patients who were managed by our IRT from October 2014 to June 2019 was done. Patients younger than 18 years of age were selected and clinical data including age, gender, etiology, complications, and outcome of intestinal rehabilitation were collected.
All patients received management by a multidisciplinary IRT, as previously described [5, 6]. Briefly, the IRT consists of a pediatric surgeon, pharmacist, clinical dietitian, inpatient and home nursing staff focused on the care of pediatric patients with IF. Upon presentation to the IRT, a thorough work-up of the patient was performed to assess the nutrition status, length and anatomy of remnant bowel, and complications. Patients were prescribed a combination of PN and enteral nutrition (including oral intake) based upon their enteral tolerance. Enteral nutrition was encouraged as much as possible. Patients were monitored daily with vital signs, urine output, stool output, and body weight measurements. Blood was drawn weekly to analyze complete blood counts, electrolytes, liver enzymes, bilirubin, creatinine, albumin, and C-reactive protein. Trace elements and vitamins levels were checked monthly to bimonthly. Patients were encouraged to be discharged as early as possible and receive home PN. Home PN was applied to patients that satisfied our center's criteria for home PN (Table 1).

Table 1
Indications for home PN application
IF-associated liver disease (IFALD) was diagnosed when 2 consecutive measurements taken more than 1 week apart showed direct bilirubin >2.0 mg/dL and the patient did not have other apparent causes of cholestatic liver dysfunction including viral hepatitis, metabolic liver disease, structural anomalies of the hepatobiliary system, ongoing infection or sepsis, and prolonged use of hepatotoxic drugs. All patients' PN was administered via a tunneled single lumen central venous catheter (4.2 Fr Broviac catheter; BARD, Covington, GA, USA) which was preferably inserted into the right internal jugular vein. Central line-associated blood stream infection (CLABSI) was diagnosed according to the surveillance definition by the Centers for Disease Control and Prevention/National Healthcare Safety Network [7].
Twenty-five patients younger than 18 years were managed during this period and were included in the analysis. There were 18 boys and 7 girls. Median age at presentation to the IRT was 1.6 years (range, 0.1–11.0 years). Median length of follow-up was 42.9 months (range, 2.3–58.8 months).
Cause of IF was short bowel syndrome in 18 patients (Table 2). Underlying pathology to short bowel were necrotizing enterocolitis in 8 cases, midgut volvulus in 4 cases, intestinal atresia in 4 cases, and Hirschsprung's disease in 2 cases. Seven patients with non-short bowel syndrome IF included chronic intestinal pseudo-obstruction (CIPO, 4 cases), megacystis microcolon intestinal hypoperistalsis syndrome (1 case), radiation enteritis (1 case), and autoimmune leiomyositis of small bowel (1 case).
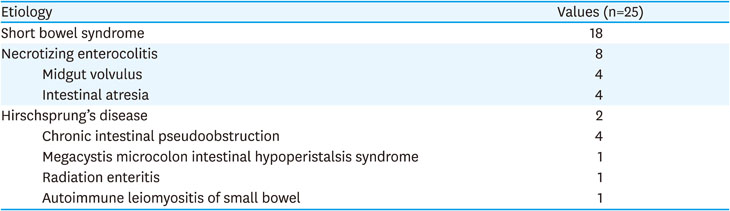
Table 2
Etiology of intestinal failure
Twenty-four patients are alive at last follow-up (Table 3). The single mortality case was due to progression of his original malignancy (desmoplastic small round cell tumor of the retroperitoneum). Overall 12 patients have weaned off PN (12/24, 50%): 10 out of 18 patients (55.5%) with short bowel and 2 out of 6 patients (33.3%) with other causes of IF. Median time to weaning off PN was 4.8 months (range, 2.0–34.3 months) after management by multidisciplinary IRT and 9.4 months (range, 2.0–72.6 months) after initial surgery leading to IF. The remaining 12 patients are receiving home PN. The clinical and anatomical characteristics of IF patients are outlined in further detail in Tables 4, 5, 6, 7.

Table 3
Patient outcome
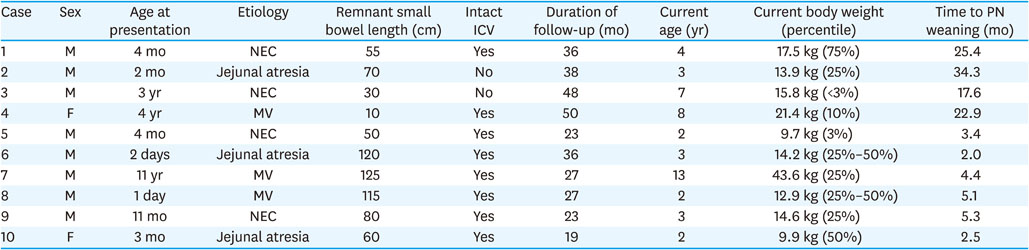
Table 4
Clinical and anatomical characteristics of short bowel syndrome-intestinal failure: patients weaned off parenteral nutrition
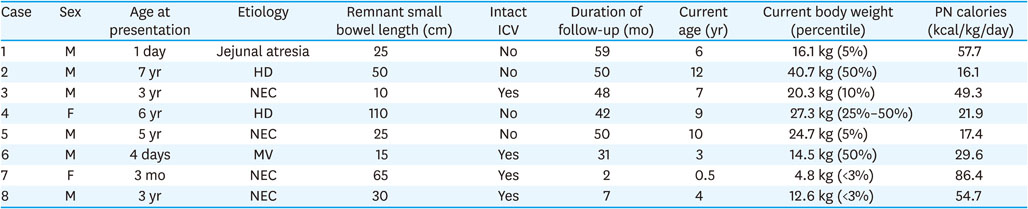
Table 5
Clinical and anatomical characteristics of short bowel syndrome-intestinal failure: patients on parenteral nutrition support

Table 6
Clinical and anatomical characteristics of intestinal failure (other causes): patients weaned off parenteral nutrition

Table 7
Clinical and anatomical characteristics of intestinal failure (other causes): patients on parenteral nutrition support
IFALD occurred in 2 patients with CIPO, following 7 years and 11 years of PN use. Both cases were managed by switching the lipid emulsion to 100% fish oil (Omegaven; Fresenius Kabi Austria Gmbh, Graz, Austria) from their baseline lipid emulsion, SMOFlipid (Fresenius Kabi Austria Gmbh).
Fifteen cases of CLABSI were diagnosed in 9 patients. Incidence of CLABSI was 0.82/1,000 PN days.
Serial transverse enteroplasty procedures were done in 3 patients 5.2 months, 50.8 months, and 52.3 months following each patients' initial surgical procedures. There were no patients receiving intestinal transplants during the study period.
Management of patients with IF has undergone drastic changes in recent decades with widespread implementation of multidisciplinary intestinal rehabilitation programs in dedicated centers around the world [8, 9]. The application of multidisciplinary team approach in pediatric intestinal rehabilitation has allowed IF patients to be provided with timely and successful integration of medical, surgical, and nutritional care. In turn, this has led to positive outcomes in terms of survival, sepsis events, and IFALD [10, 11, 12]. We report the outcome of multidisciplinary intestinal rehabilitation in pediatric patients since the initiation of an IRT in our institute. This is, to the best of our knowledge, the first report of multidisciplinary intestinal rehabilitation in pediatric patients from a Korean IRT. This study does not provide an analysis of improved outcomes according to the application of multidisciplinary IRT care because we have been employing multidisciplinary team approach since the beginning of our IRT. However, our current outcome results are comparable to those reported from North American centers that actively promote multidisciplinary intestinal rehabilitation programs.
It is well known that central venous catheter-related complications are important factors affecting outcome of pediatric IF patients [13]. In a report by Merras-Salmio et al. [14] the incidence of CLABSI was 1.01/1,000 PN days. The authors ascribed their good outcomes to the use of commercially manufactured 3-in-1 PN bags and taurolidine central venous catheter locks for CLABSI prevention. We have not utilized taurolidine locks in our program but have been routinely using commercial 3-in-1 PN bags in all of our patients on home PN. We also believe that this practice has contributed to the relatively low incidence of CLABSI in our pediatric IF patients.
Although fractures of central venous catheters are not well described in the literature, we have encountered several cases of catheter fractures that require surgical revision. It has proven to be a significant complication requiring more attention when managing IF patients. We have also experienced one severe case of central venous catheter-related thrombosis that extended from the left internal jugular vein to the superior vena cava. This 7-year-old boy required thrombectomy via open thoracotomy and temporary placement of a central venous catheter in the inferior vena cava.
Liver dysfunction is a major concern in pediatric IF patients in need of long term PN support. It is believed that lipids, specifically lipids from soy are one of the main causes of liver dysfunction in IF patients manifesting as progressive cholestasis. We did not actively perform liver biopsies in any of our patients and employed the criteria of direct bilirubin > 2.0 mg/dL for diagnosis of IFALD. We experienced 2 cases of IFALD among our cohort of patients and both were successfully managed by the strategy of fish oil monotherapy, as previously published describing our group's earlier experience [5]. This novel approach of eliminating soybean oil and exclusively providing fish oil was successfully applied to the 2 children with CIPO.
In conclusion, pediatric IF is a heavy burden for both patients and their medical staff. However, few centers have sufficient experience or dedicated personnel to provide necessary care for these children. Particularly important factors are IFALD and catheter-related complications, which may lead to patients requiring invasive procedures such as intestinal transplant. Team-based multidisciplinary approach and treatment protocols is important in improving outcomes in terms of enteral autonomy, survival, and quality of life.
Conflict of Interest:No potential conflict of interest relevant to this article was reported.
Author Contributions:
Conceptualization: L.S., P.H.J.
Data curation: K.H.J., M.J.K.
Formal analysis: L.C.
Methodology: S.J.M., L.S.
Supervision: S.J.M.
Validation: P.H.J., L.C., K.H.J.
Writing - original draft: L.C., L.S.
Writing - review & editing: L.S.
